295,00 € – 895,00 €
Product details
Synonyms = Major synaptic vesicle protein p38; MRX96; MRXSYP; Syn p38; Syp; SYPH
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = MSVA-462R
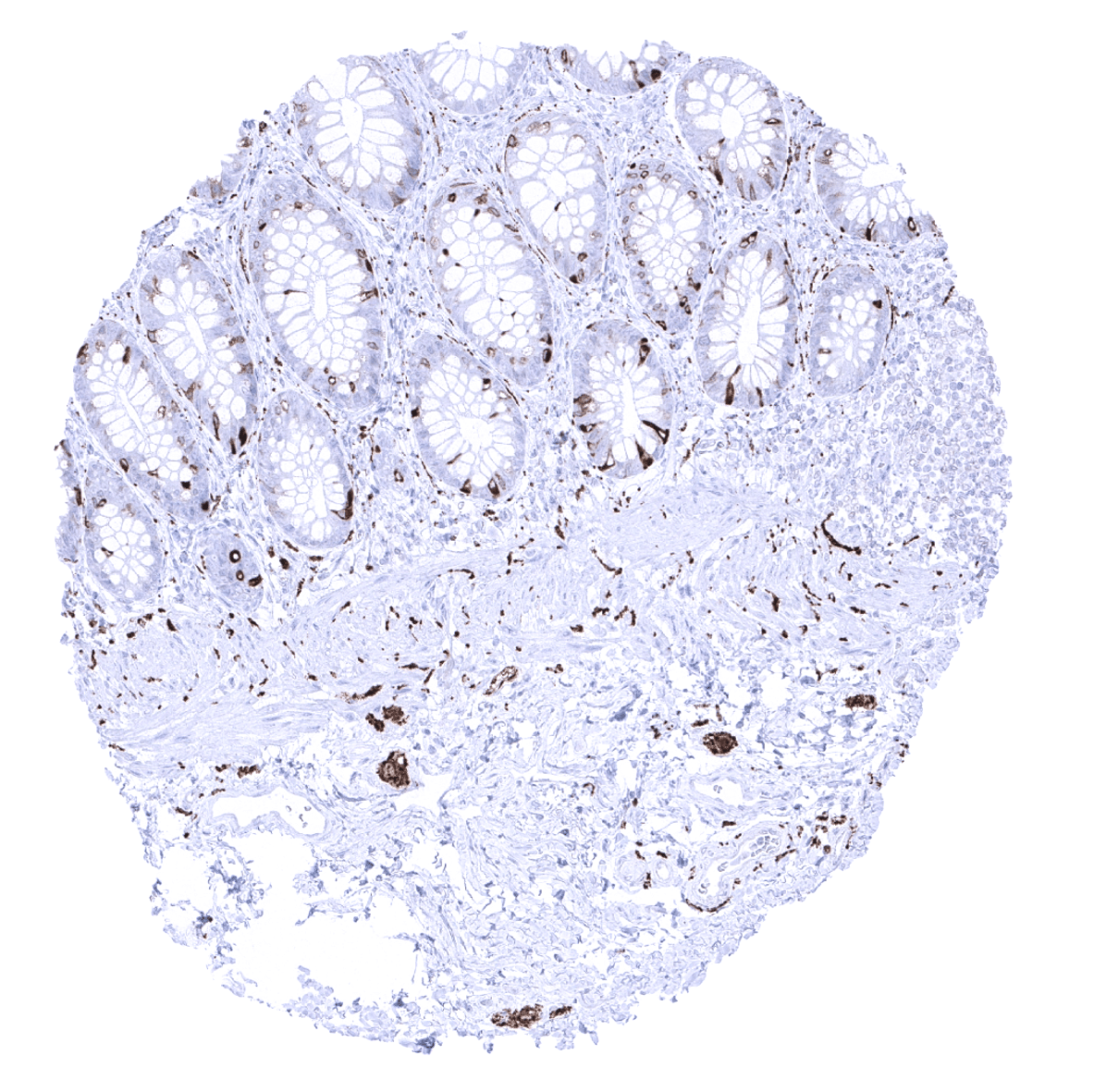
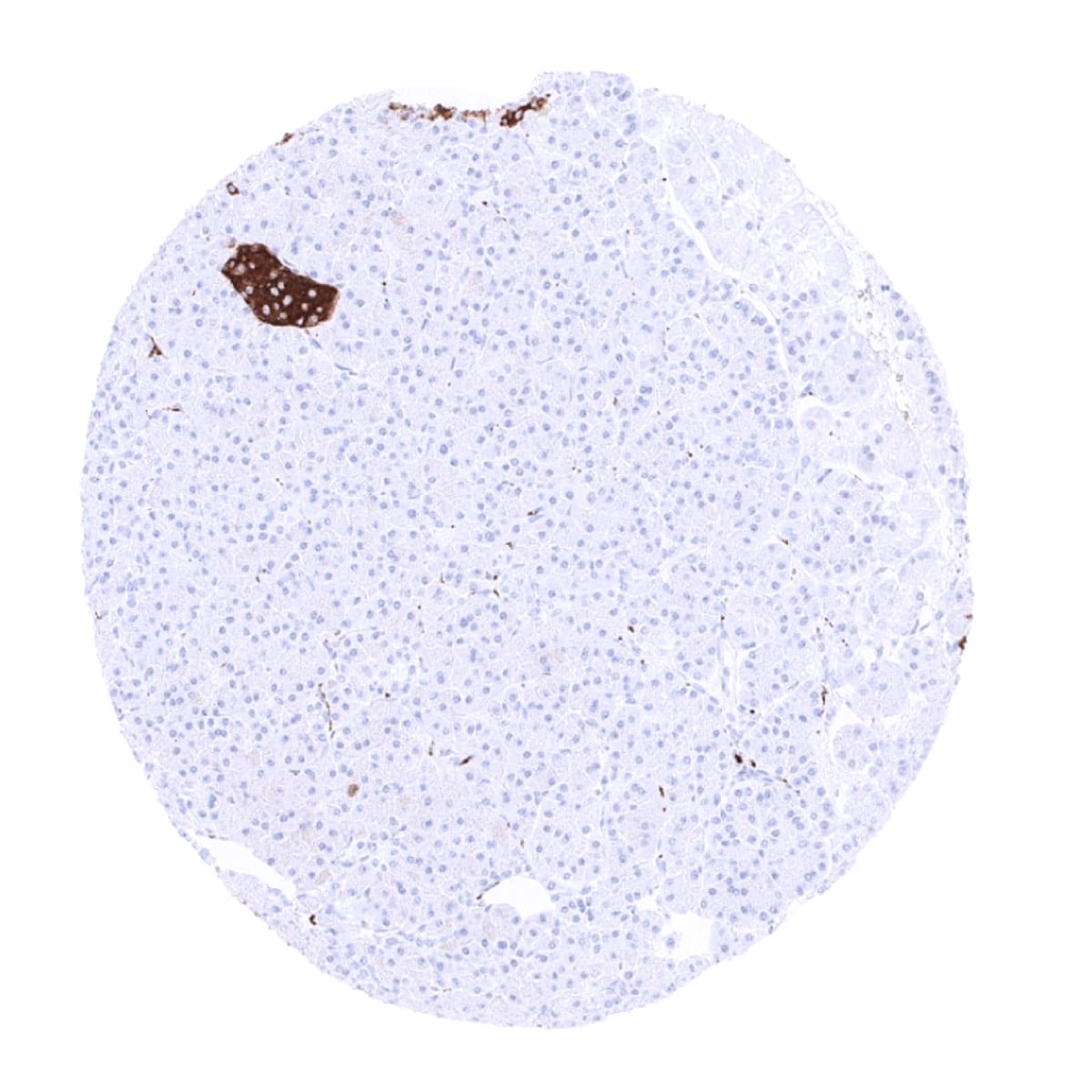
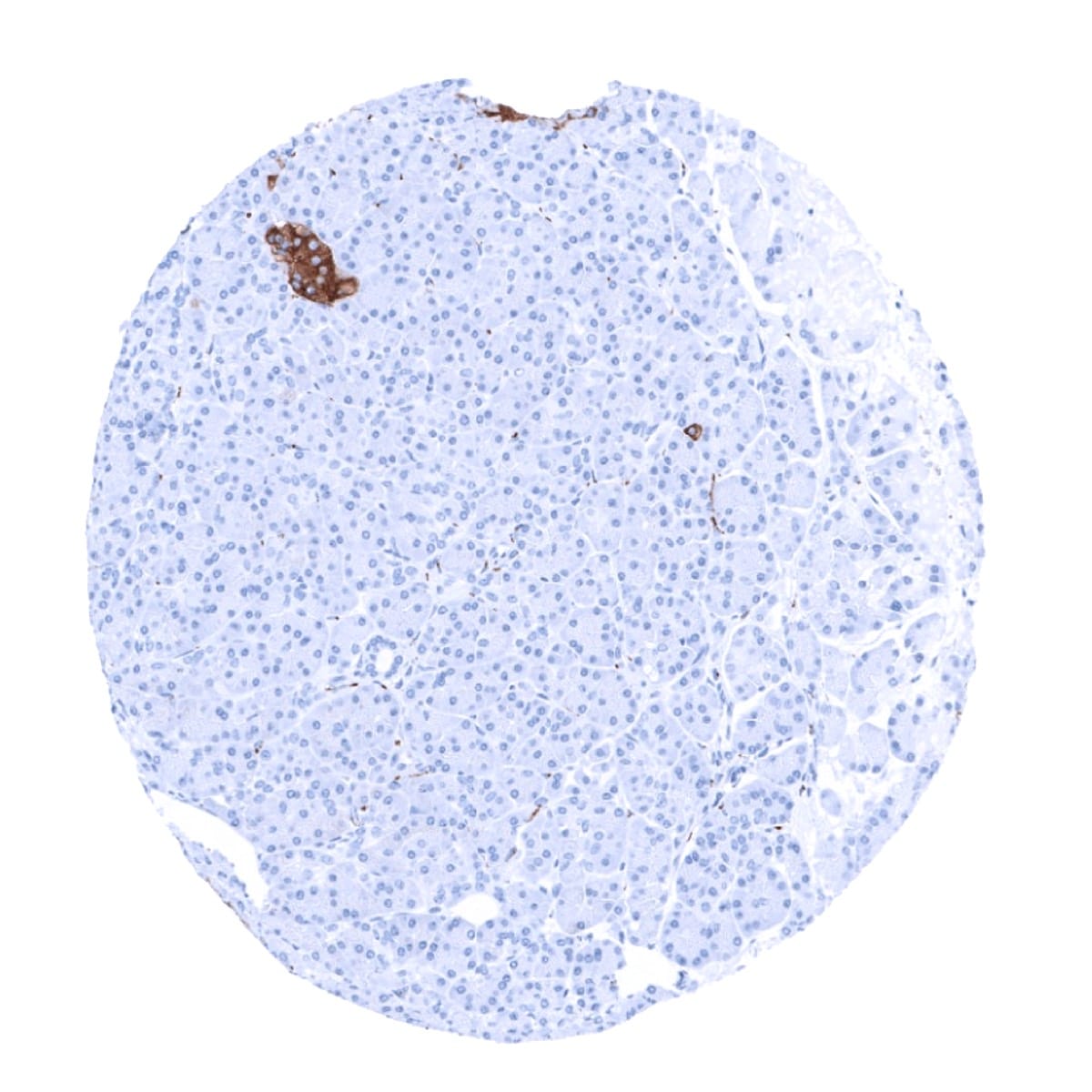
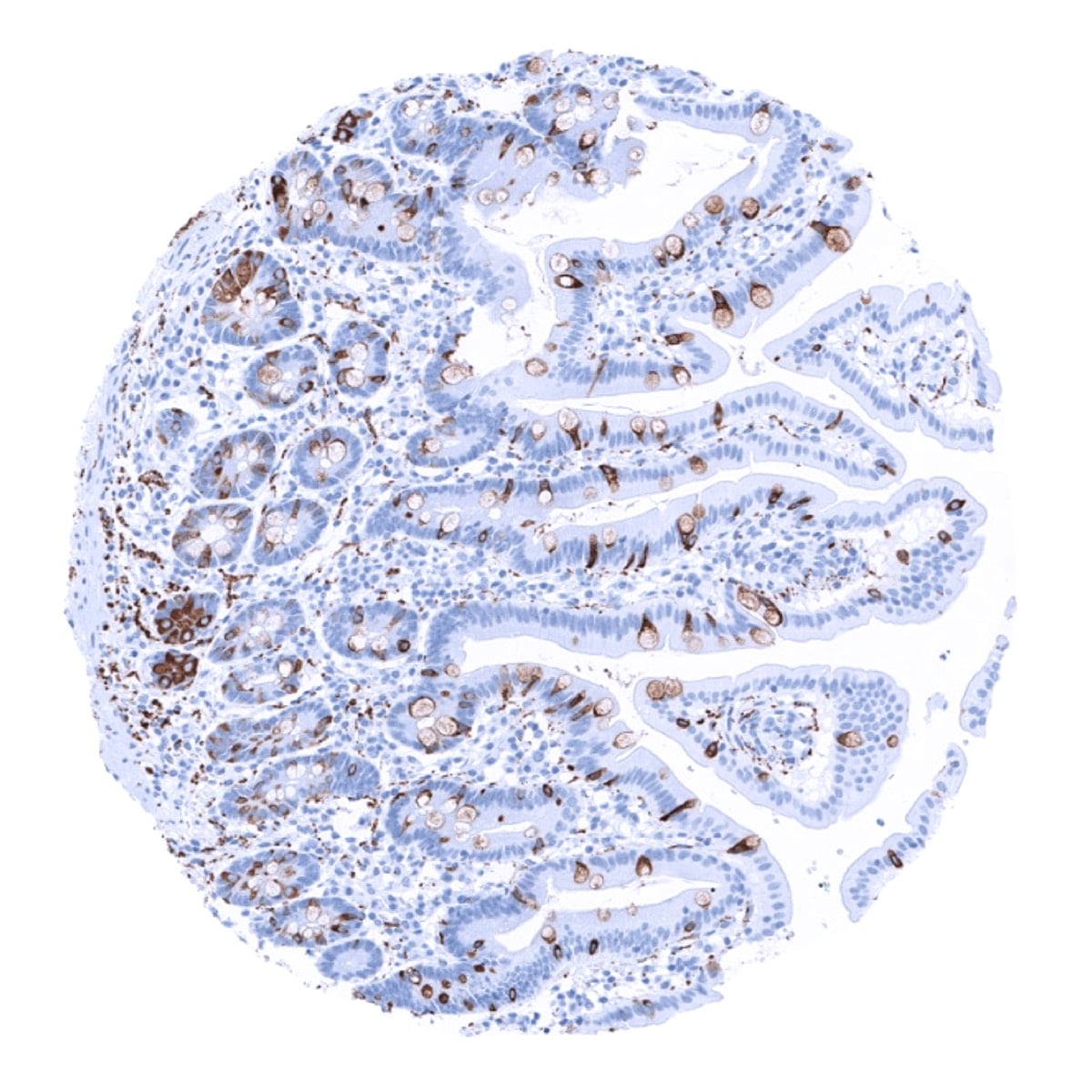
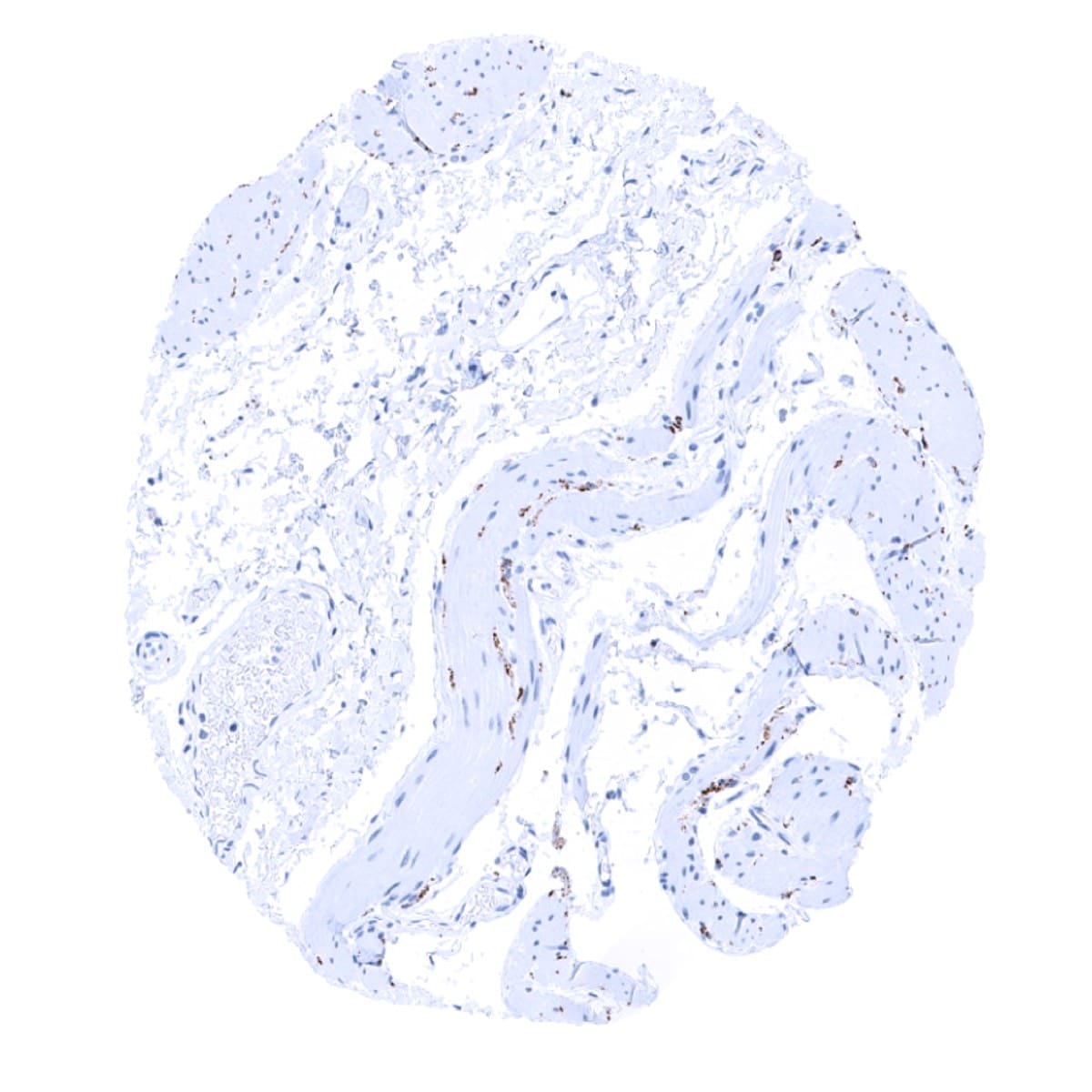
Positive control = Colon: A moderate to strong staining of the axons of the Auerbach’s and Meissner’s plexus should be seen while the endocrine cells of the mucosa and the peripheral nerves in the mucosa must show an at least a weak to moderate staining. Pancreas: A strong staining should be seen in islets of Langerhans and in peripheral nerve fibres located between the exocrine cells.
Negative control = Colon: All non-endocrine epithelial cells and lymphocytes should not show any staining.
Cellular localization = Cytoplasmic
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
Synaptophysin is expressed in neuronal and neuroendocrine cells.
Biology Behind
Synaptophysin is a 38kDa calcium binding integral-membrane glycoprotein protein coded by the SYP gene located at Xp11.23-p11.22. It is also termed as “major synaptic vesicle protein p38” reflecting the fact that it is the most abundant synaptic vesicle membrane glycoprotein, present in neuronal presynaptic vesicles. It is present in virtually all neurons in the brain and spinal cord that participate in synaptic transmission. Because of its ubiquity at the synapse, synaptophysin quantification by immunostaining is used for quantification of synapses. Synaptophysin interacts with the essential synaptic vesicle protein synaptobrevin but its exact function is not known. Elimination of synaptophysin in mice results in behavioral changes such reduced spatial learning. Synaptophysin has been suggested to play a role in X linked intellectual disability. Synaptophysin is also regularly expressed in neuroendocrine cells and its immunohistochemical detection is thus used to diagnose neuroendocrine tumors.
Staining Pattern in Normal Tissues
Synaptophysin staining pattern in Normal Tissues with antibody MSVA-462R (images are shown in our “Normal Tissue Gallery”)
| Brain | Cerebrum | Strong synaptophysin positivity. |
| Cerebellum | Strong synaptophysin positivity. | |
| Endocrine Tissues | Thyroid | Strong synaptophysin positivity of T-cells.. |
| Parathyroid | Negative. | |
| Adrenal gland | Strong synaptophysin positivity of all cells from the medulla. Weak to moderate synaptophysin staining can occur in a fraction of adrenocortical cells. | |
| Pituitary gland | Strong synaptophysin positivity of the posterior lobe and of all epithelial cells of the anterior lobe. | |
| Respiratory system | Respiratory epithelium | Strong synaptophysin positivity of scattered neuroendocrine cells. |
| Lung | Negative. | |
| Gastrointestinal Tract | Salivary glands | Synaptophysin positivity of nerve fibres in the stroma. Epithelial cells are negative. |
| Esophagus | Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Stomach | Strong synaptophysin positivity of scattered neuroendocrine cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Duodenum | Strong synaptophysin positivity of scattered neuroendocrine cells and of goblet cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Small intestine | Strong synaptophysin positivity of scattered neuroendocrine cells and of goblet cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Appendix | Strong synaptophysin positivity of scattered neuroendocrine cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Colon | Strong synaptophysin positivity of scattered neuroendocrine cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
| Rectum | Strong synaptophysin positivity of scattered neuroendocrine cells. Variable (weak to strong) synaptophysin staining of axons and ganglion cells of the peripheral nerves in the gastrointestinal wall. | |
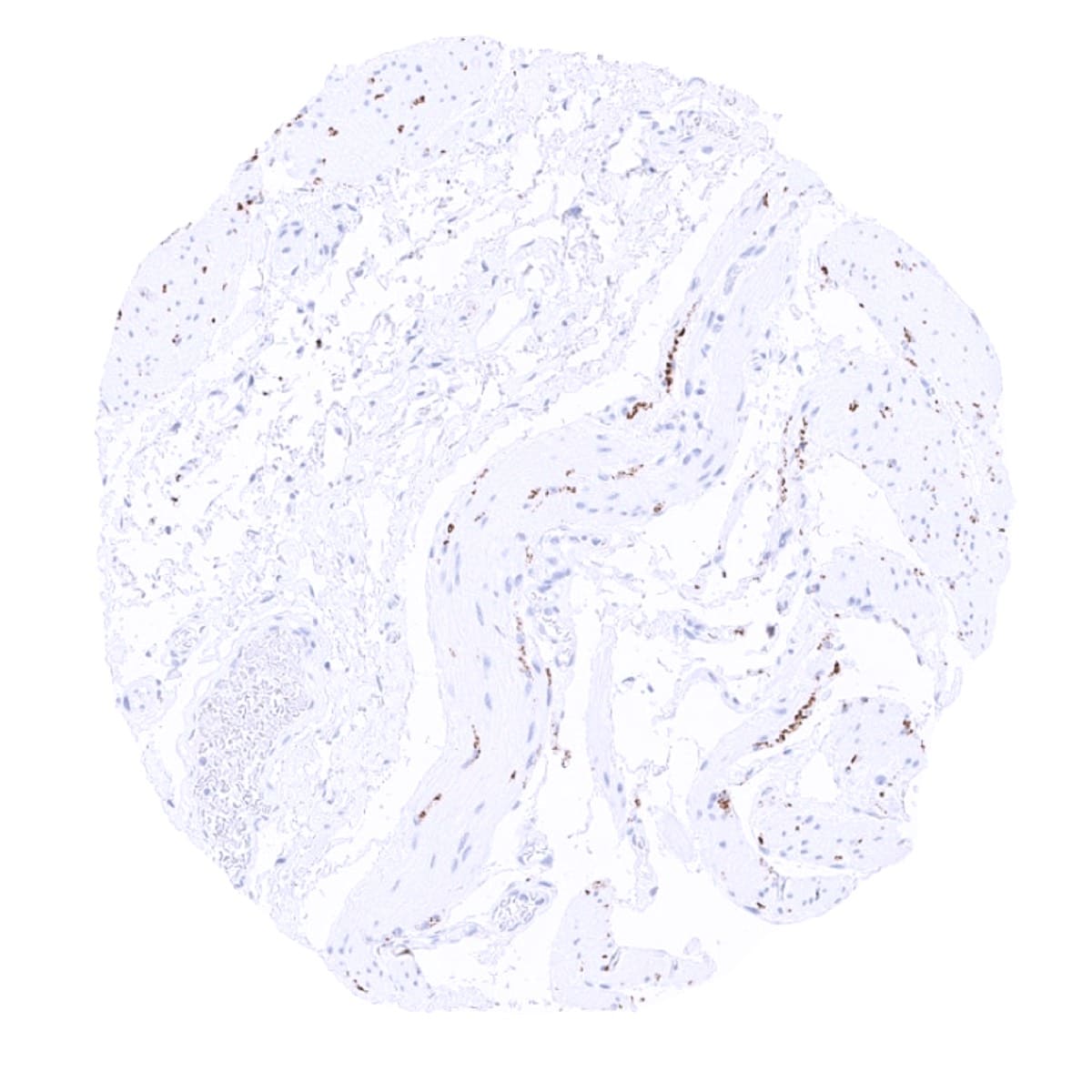
| Liver | Negative. But nerve fibres are synaptophysin positive. | |
| Gallbladder | Negative. But some nerve fibres may be synaptophysin positive. | |
| Pancreas | Strong synaptophysin positivity of islet cells. | |
| Genitourinary | Kidney | Negative. |
| Urothelium | Negative. | |
| Male genital | Prostate | Synaptophysin positivity of nerve fibres in the stroma. Epithelial cells are negative. |
| Seminal vesicles | Synaptophysin positivity of nerve fibres in the stroma. Epithelial cells are negative. | |
| Testis | Negative. | |
| Epididymis | Negative. | |
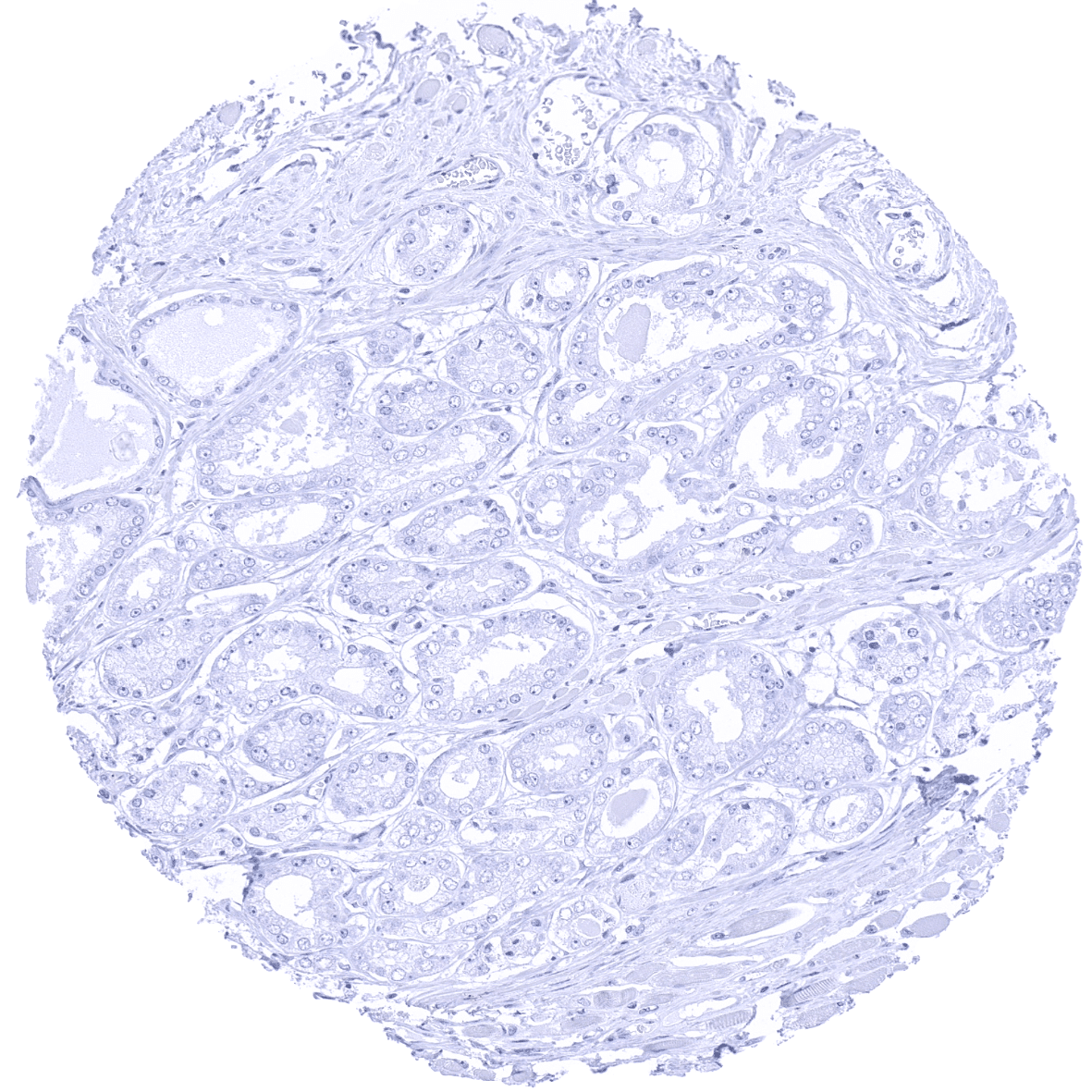
| Female genital | Breast | Negative. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Negative. | |
| Uterus endocervix | Strong synaptophysin positivity of scattered neuroendocrine cells. | |
| Uterus, endometrium | Negative. | |
| Fallopian Tube | Negative. | |
| Ovary | Synaptophysin positivity of nerve fibres in the stroma. | |
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | Negative. | |
| Chorion | Negative. | |
| Skin | Epidermis | Strong synaptophysin positivity of scattered neuroendocrine cells. |
| Sebaceous glands | Negative. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Synaptophysin positivity of nerve fibres in the stroma of many organs. | |
| Endothelium | Negative. | |
| Bone marrow/ lymphoid tissue | Bone marrow | Negative. |
| Lymph node | Negative. | |
| Spleen | Negative. | |
| Thymus | Negative. | |
| Tonsil | Negative. | |
| Remarks |
These findings are largely comparable to the RNA and protein data summarized in the Human Protein Atlas (Tissue expression Synaptophysin)
Suggested Positive control: Colon: A moderate to strong staining of the axons of the Auerbach’s and Meissner’s plexus should be seen while the endocrine cells of the mucosa and the peripheral nerves in the mucosa must show an at least a weak to moderate staining. Pancreas: A strong staining should be seen in islets of Langerhans and in peripheral nerve fibres located between the exocrine cells.
Suggested Negative control: Colon: All non-endocrine epithelial cells and lymphocytes should not show any staining.
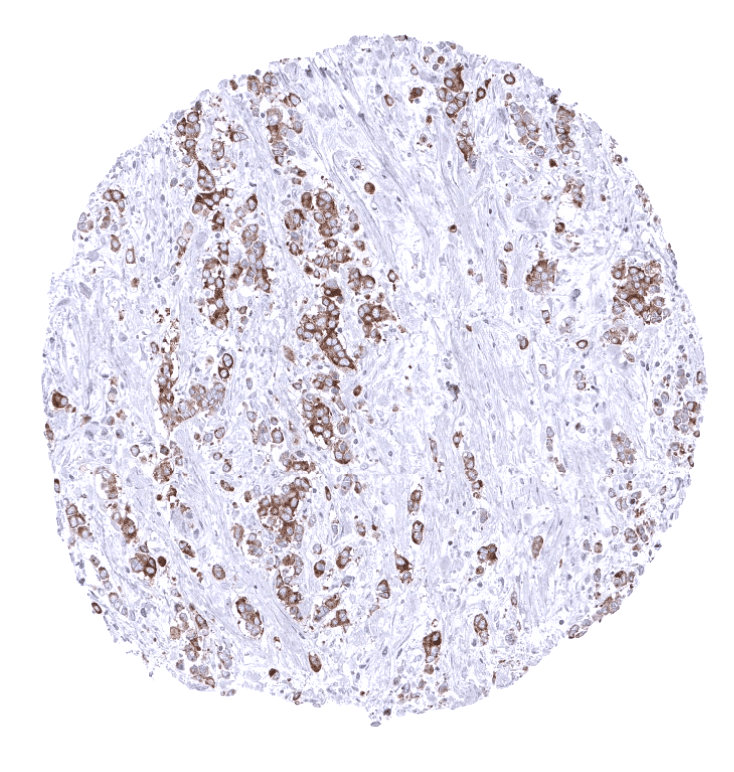
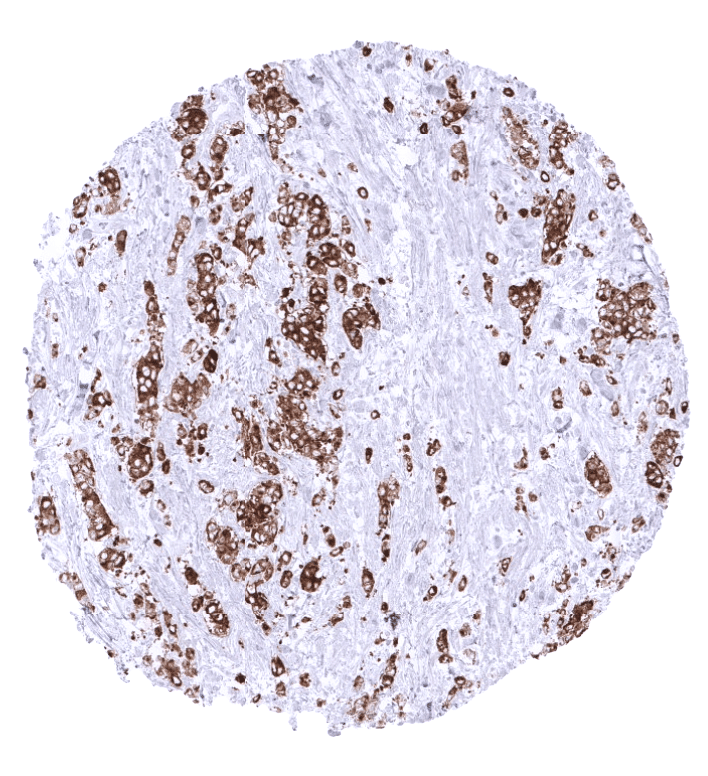
Staining Pattern in Relevant Tumor Types
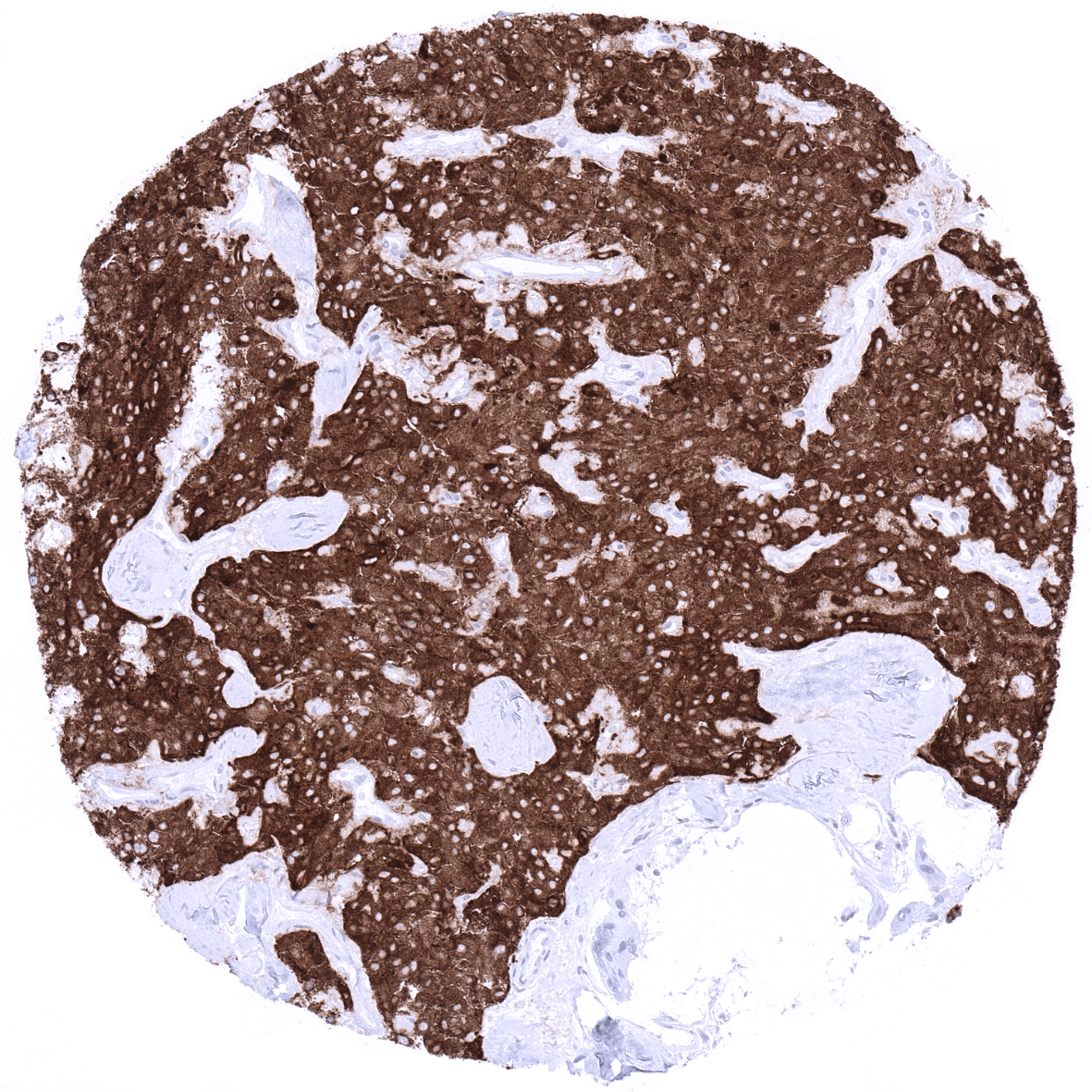
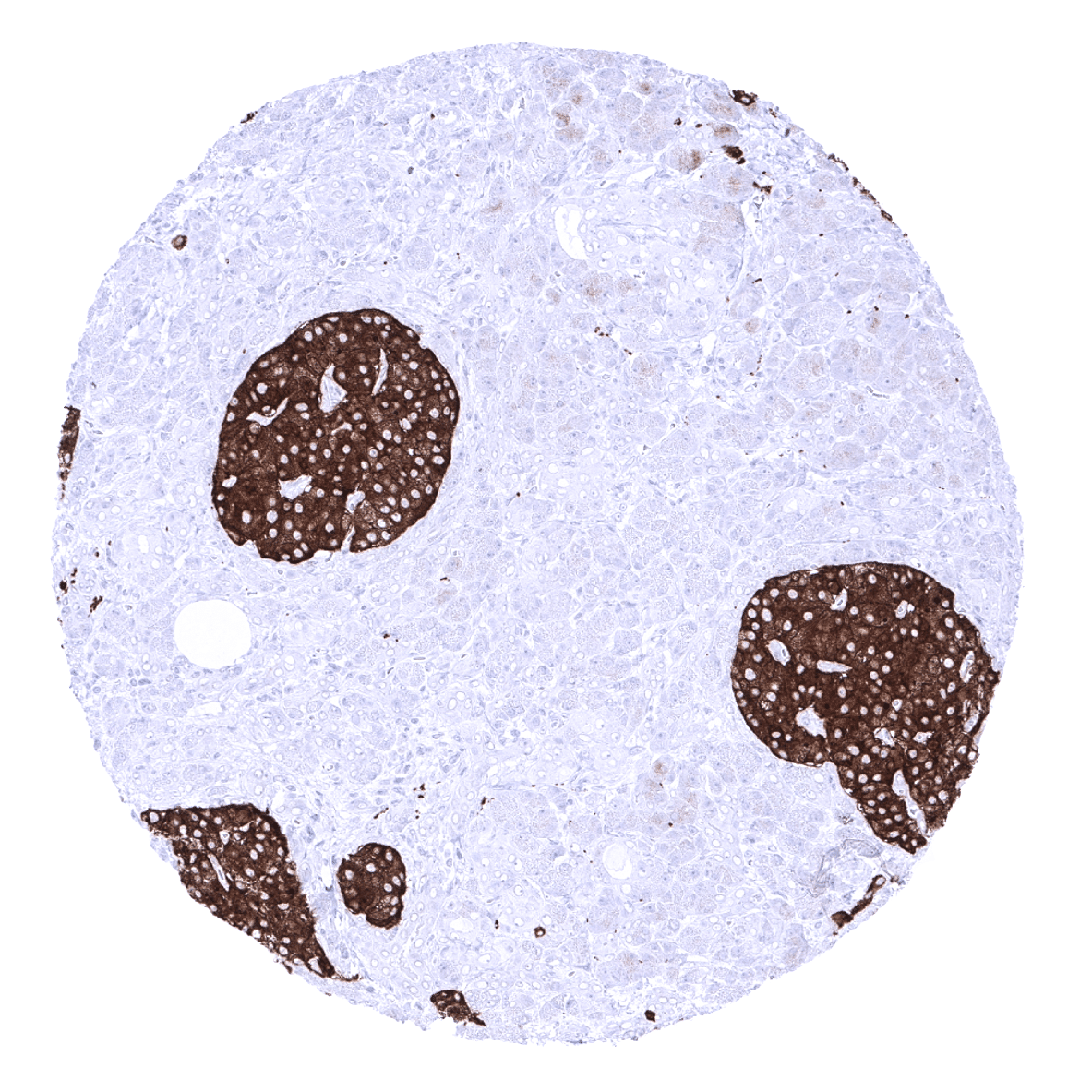
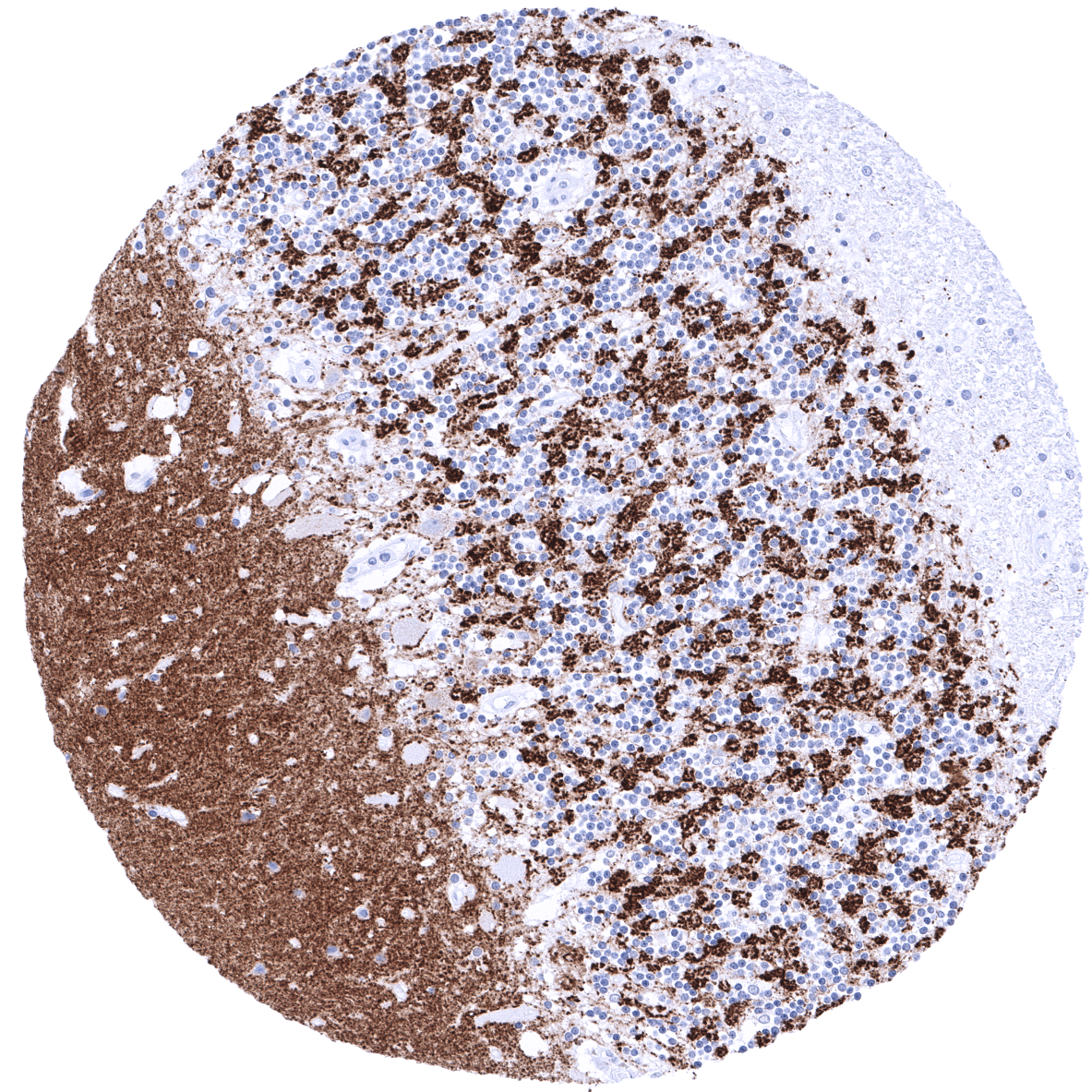
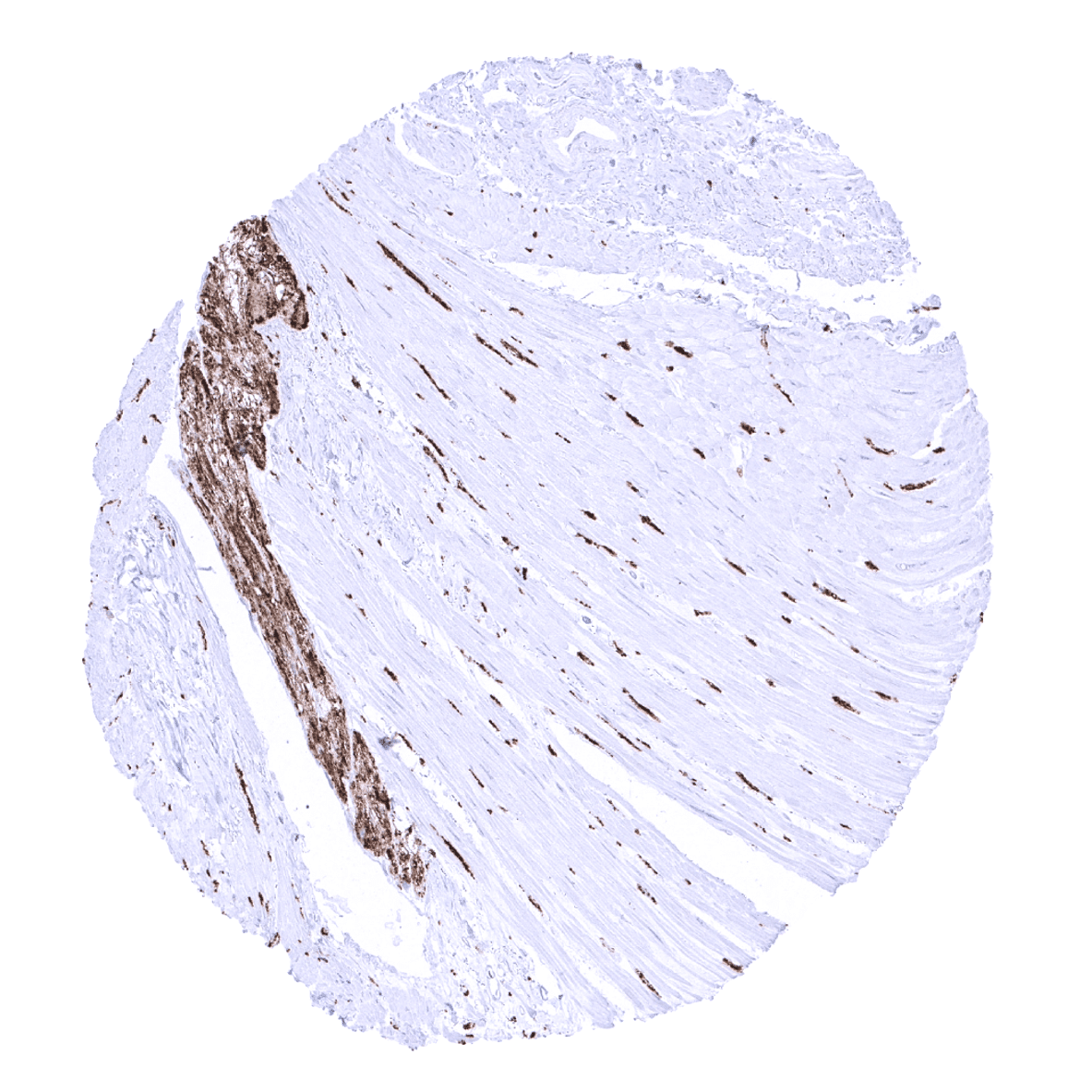
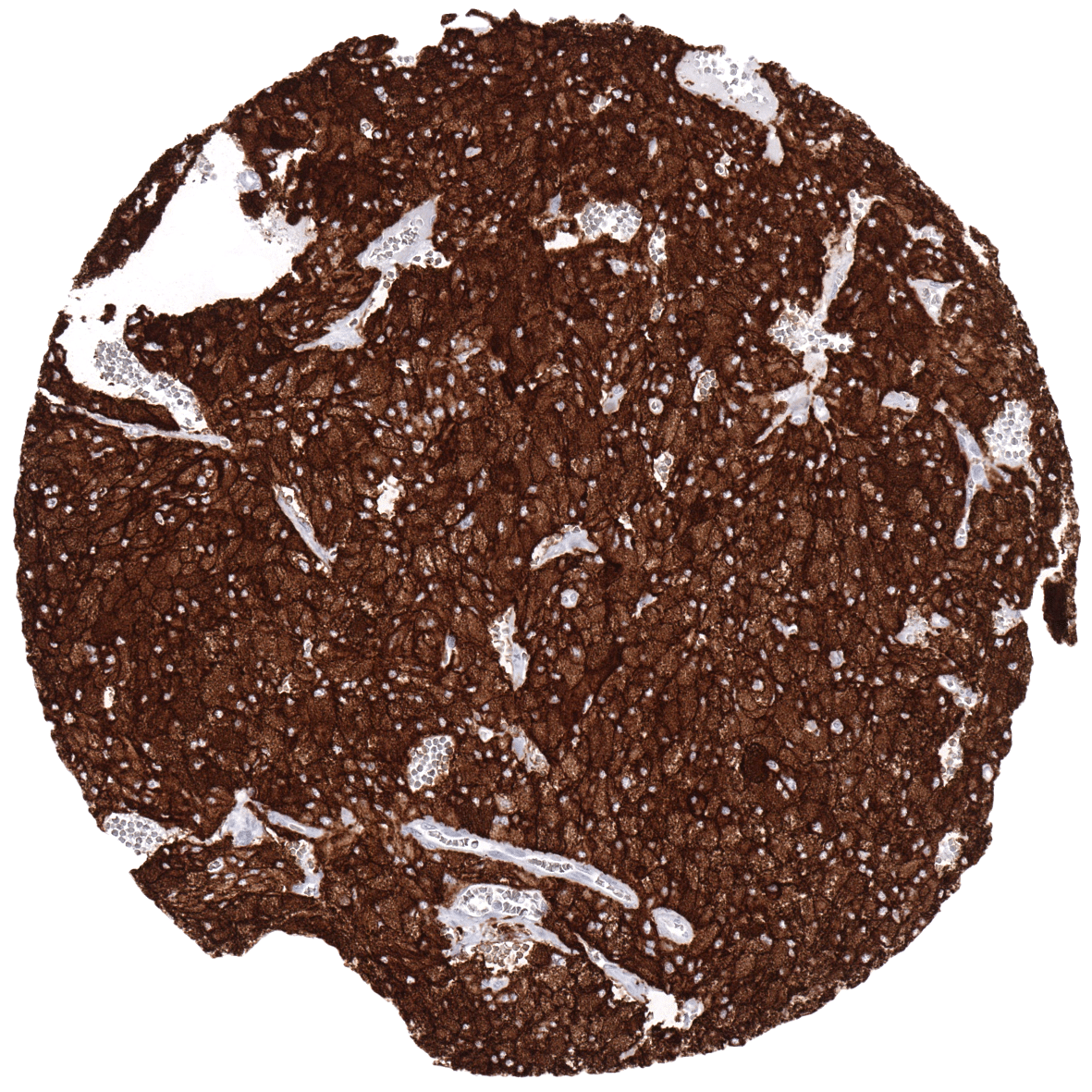
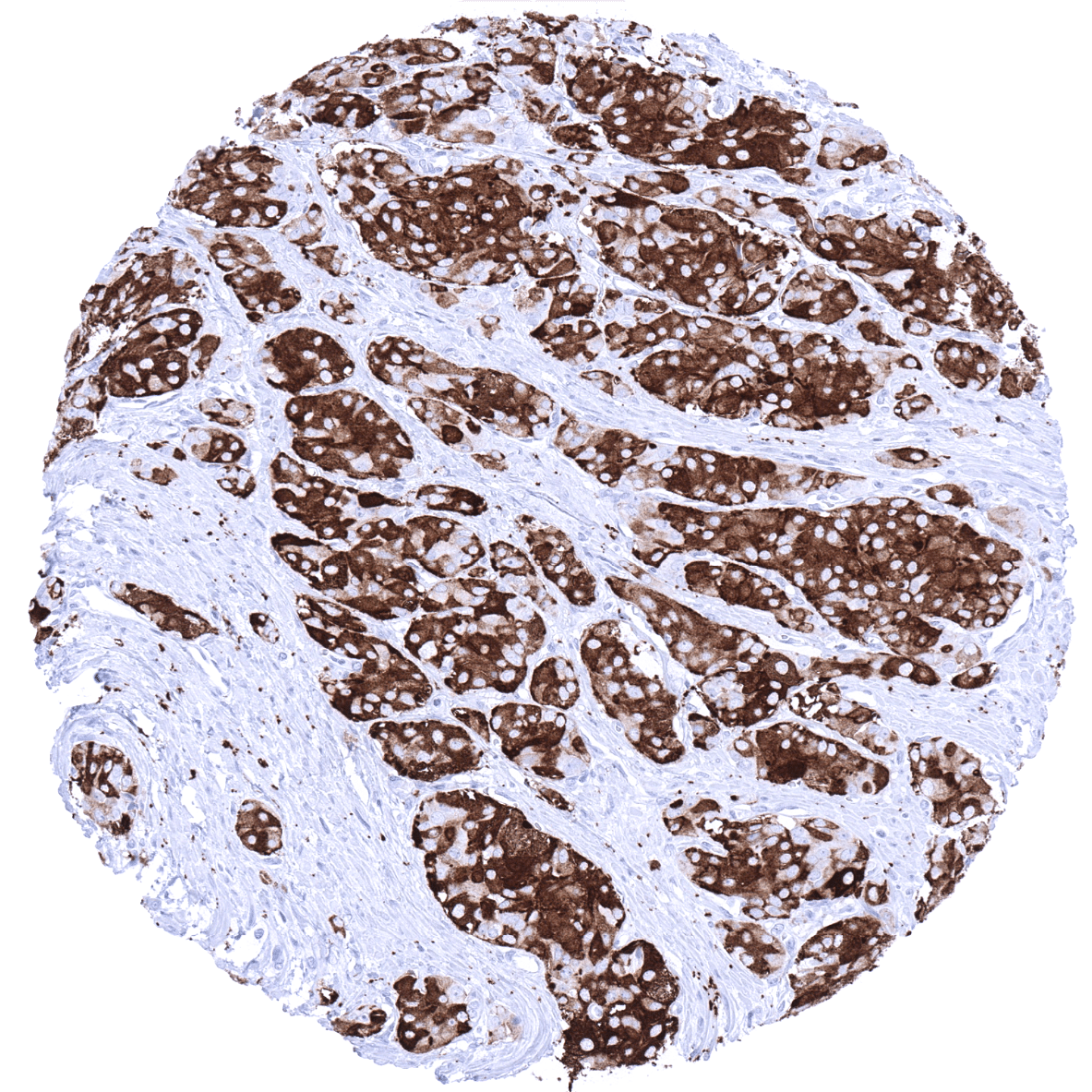
Synaptophysin is typically expressed at high levels in pheochromocytoma, neuroendocrine tumors, neuroendocrine carcinomas, medullary carcinomas of the thyroid, pituitary adenomas, Merkel cell carcinomas and in small cell carcinomas irrespective of their site of origin. Synaptophysin immunostaining is also seen in various neuronal tumors such as neuroblastoma, ganglioneuroblastoma, ganglioneuroma, and ganglioglioma. Synaptophysin may also be detected in brain tumors like oligodendroglioma, astrocytoma and ependymoma, however, to a varying extent. Moreover, synaptophysin can be detected in a small fraction of various other tumor entities, such as for example breast, prostate or ovarian cancers if these tumors exhibit neuroendocrine differentiation.
The TCGA findings on Synaptophysin RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
Synaptophysin (MSVA-462R) publication summary
Relevant publication: Uhlig et al.“Synaptophysin and chromogranin A expression analysis in human tumors”. Published in Mol Cell Endocrinol. 2022 Sep 15;555:111726. PMID: 35921917.
A total of 13’405 tumors from 120 different tumor categories were successfully analyzed by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH7,8 Target Retrieval Solution buffer. MSVA-462R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
In this study, at least one synaptophysin positive case was seen in 61 (50.8%) of 120 tumor categories and 37 (30.8%) tumor categories included at least one case with strong positivity. The highest frequencies of synaptophysin positivity (and the highest levels of expression) were seen in various types of neuroendocrine neoplasms (77.8-100%), pheochromocytoma (100%), paraganglioma (100%), Merkel cell carcinoma of the skin (95.7%), medullary thyroid carcinoma (94.4%), adrenocortical carcinoma (88%), small cell carcinoma of the lung (71.4%), adrenocortical adenoma (50%), mucinous carcinoma of the ovary (26.8%), ganglioneuroma (22.2%), Ewing sarcoma (22.2%), mucinous breast cancer (18.8%), acinar cell carcinomas of the pancreas (18.8%), and in high grade endometrial carcinoma (15.4%). 38 additional entities showed (a usually weak) synaptophysin positivity in <12% of cases. The distribution of positive staining results is shown in an “organ-systematic” and in a “ranking order” figure below (images based on data from Uhlig et al.). Results on possible associations with histopathological and clinical parameters of tumor aggressiveness are also summarized below (table based on data from Uhlig et al.).
Authors conclusions on diagnostic utility of synaptophysin immunohistochemistry with respect to the distinction of different tumor entities (Uhlig et al.):
- Distinction of neuroendocrine tumors or tumors with neuroendocrine differentiation from other tumors (as part of a panel).
Authors conclusions on potential diagnostic pitfalls of synaptophysin immunohistochemistry (Uhlig et al.):
- Synaptophysin positivity can – in principle – occur in every tumor entity. Do not overinterpret expression of neuroendocrine markers in tumors lacking neuroendocrine-like morphology.
- Synaptophysin positive adrenocortical tumors must not be misinterpreted as pheochomocytoma.
- Synaptophysin positive acinar cell carcinoma of the pancreas must not be misinterpreted as neuroendocrine tumor/carcinoma.
Authors conclusions on prognostic/predictive role of synaptophysin expression (Uhlig et al.):
- Synaptophysin positivity was largely unrelated to histopathological features of cancer aggressiveness in endometrium cancers, pancreatic adenocarcinomas, gastric adenocarcinomas and colorectal adenocarcinomas.
- Synaptophysin positivity was linked to high pT stage (p=0,0427), poor grade (p=0,0319), and ER loss in breast cancer (p=0,0061).
Because synaptophysin is typically used in combination with chromogranin A, data on 9’697 tumors that were successfully analyzed for both markers (Uhlig et al) are shown below in a combined ranking order. These combined set of data shows that both antibodies usually stain the same tumors but also highlights two major exceptions: Basal cell carcinomas of the skin are positive for chromogranin A but not for synaptophysin. Adrenocortical adenomas and carcinomas are often positive for synaptophysin but not for chromogranin A.
Figure 1. Synaptophysin staining in cancer (“organ-systematic”; according to Uhlig et al.)

Figure 2. Synaptophysin staining in cancer (“ranking list”; according to Uhlig et al.)

Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein. Accordingly, multiple different protocols can generate identical staining results.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH9 Target Retrieval Solution buffer. Apply MSVA-462R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Agilent / Dako – Autostainer Link 48
Pretreatment in PT-Link for 30 minutes at 95°C (pH high); FLEX peroxidase blocking for 5 minutes (room temperature), MSVA-462R 1:150 for 20 minutes (room temperature), FLEX+ mouse/rabbit (LINKER) for 15 minutes (room temperature), horseradish peroxidase (HRP) for 20 minutes (room temperature), FLEX DAB+Sub-Chromo for 10 minutes (room temperature), FLEX hematoxylin for 5 minutes (room temperature).

These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, and a longer incubation time of FLEX+LINKER result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Leica – BOND RX
Dewax at 72°C for 30 seconds; Pretreatment in Bond Epitope Retrieval Solution (ER2 – EDTA pH9) for 20 minutes at 100°C; Peroxidase blocking for 5 minutes (room temperature), MSVA-462R 1:150 for 15 minutes (room temperature), Post primary (rabbit anti mouse) for 8 minutes (room temperature), Polymer (goat anti rabbit) for 8 minutes (room temperature), mixed DAB refine for 10 minutes (room temperature), hematoxylin for 5 minutes (room temperature).



These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of Post primary and or the Polymer result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Roche – Ventana Discovery ULTRA
Pretreatment for 64 minutes at 100°C (pH 8,4); CM peroxidase blocking for 12 minutes (room temperature), MSVA-462R 1:150 for 20 minutes at 36°C, secondary antibody (anti-rabbit HQ) for 12 minutes at 36°C, anti-HQ HRP for 12 minutes at room temperature, DAB at room temperature, hematoxylin II at room temperature for 8 minutes, bluing reagent at room temperature for 4 minutes.
These images depict staining results obtained by the protocol described above. It is of note, that the Ventana machines generally require higher antibody concentrations than other commonly used autostainers because the antibodies are automatically diluted during the procedure. Various other protocols can result in an identical result as shown above. A longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of secondary antibody and or the anti-HQ HRP result in stronger staining, potentially at the cost of more background staining.
Impact of pH

The strongest Synaptophysin staining by MSVA-462R is obtained at a pH 9,0. However, pH 7,8 results in only a slight reduction of the staining intensity as compared to pH9. We thus consider pH7,8 as optimal for manual staining because of the better tissue preservation at pH7,8 than at pH 9,0.
Potential Research Applications
- The clinical significance of neuroendocrine differentiation of cancers not originating from neuroendocrine precursor cells is still not clear. This especially applies for its prognostic and therapeutic implications.
- Synaptophysin interacts with the essential synaptic vesicle protein synaptobrevin but its exact function is not known.
- Because of its ubiquity at the synapse, synaptophysin quantification by immunostaining is used for quantification of synapses.
Evidence for Antibody Specificity in IHC
Specificity of MSVA-462R is documented by strong positive staining in cell types that are well documented to express synaptophysin such as islets of Langerhans, the adrenal medulla, and in scattered cells of the diffuse neuroendocrine system in combination with absence of staining in all tissues known to not express synaptophysin such as non-neuroendocrine epithelial cells, lymphocytes and muscle cells.
