295,00 € – 995,00 €
Product details
Synonyms = Nectin-4, Nectin cell adhesion molecule 4, PVRL4, PRR4, Poliovirus receptor-related protein 4, poliovirus receptor- related 4, Processed poliovirus receptor-related protein 4, Ig superfamily receptor LNIR, Ig superfamily receptor LNIR family
Antibody type = Mouse monoclonal / IgG
Clone = MSVA-304M
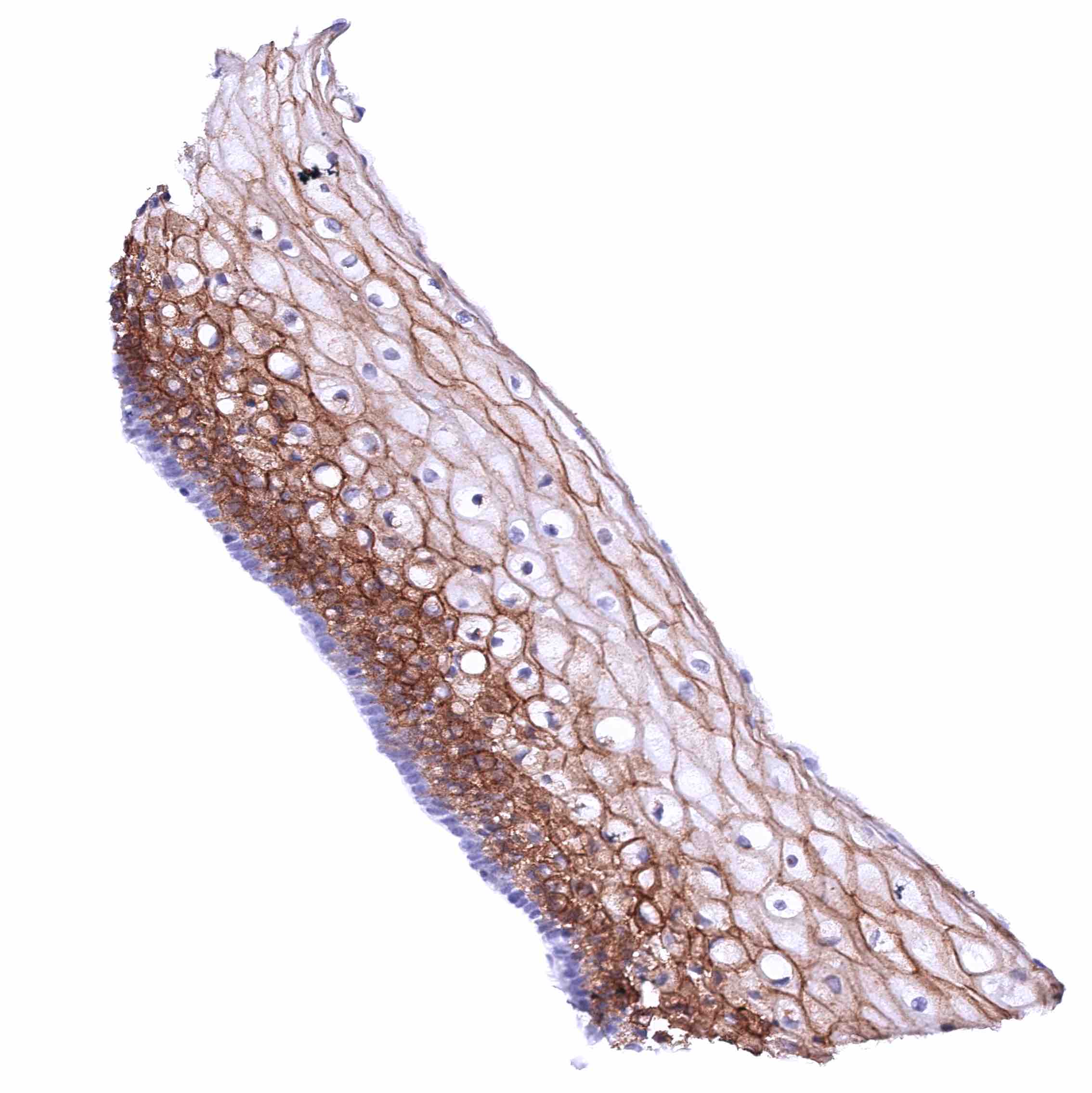
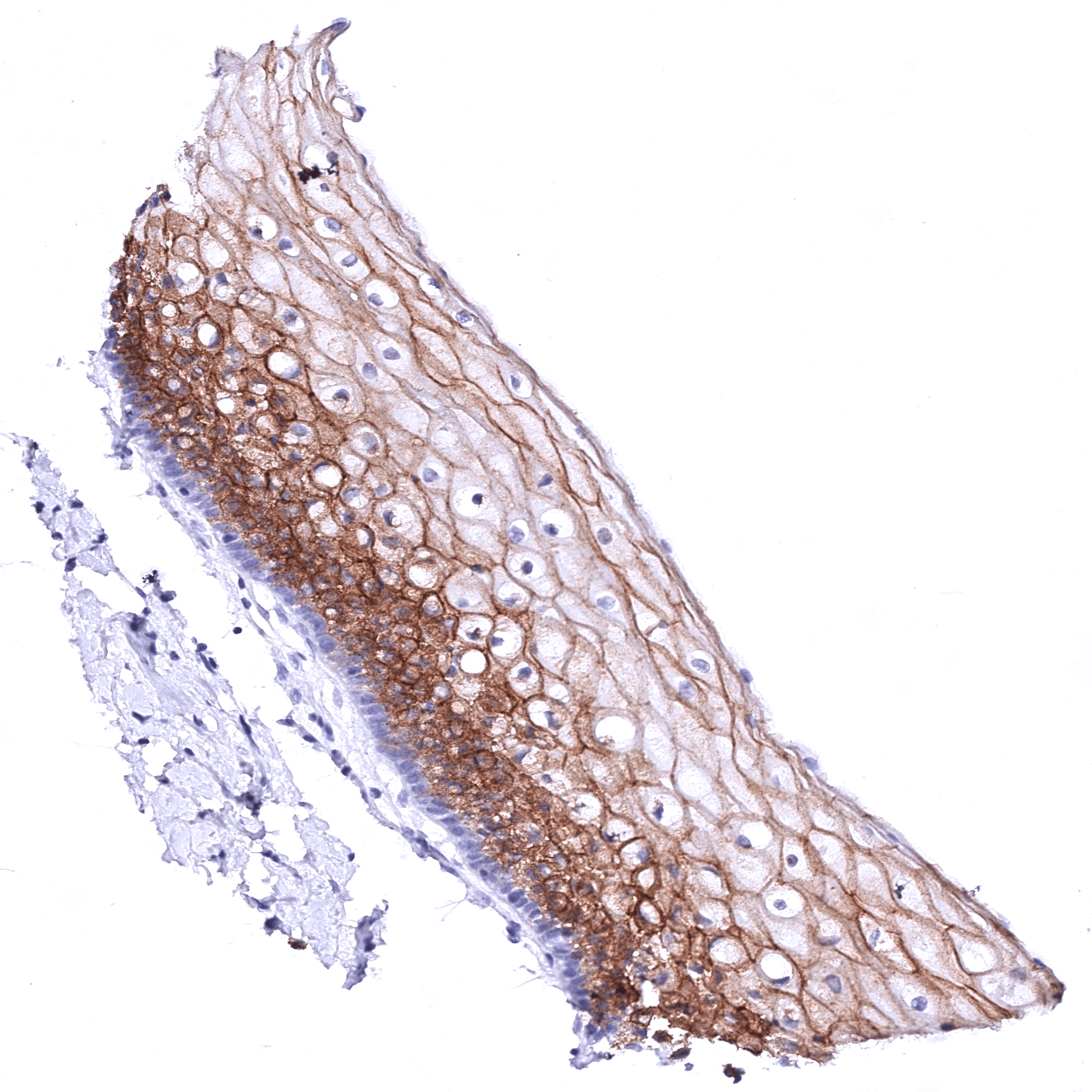
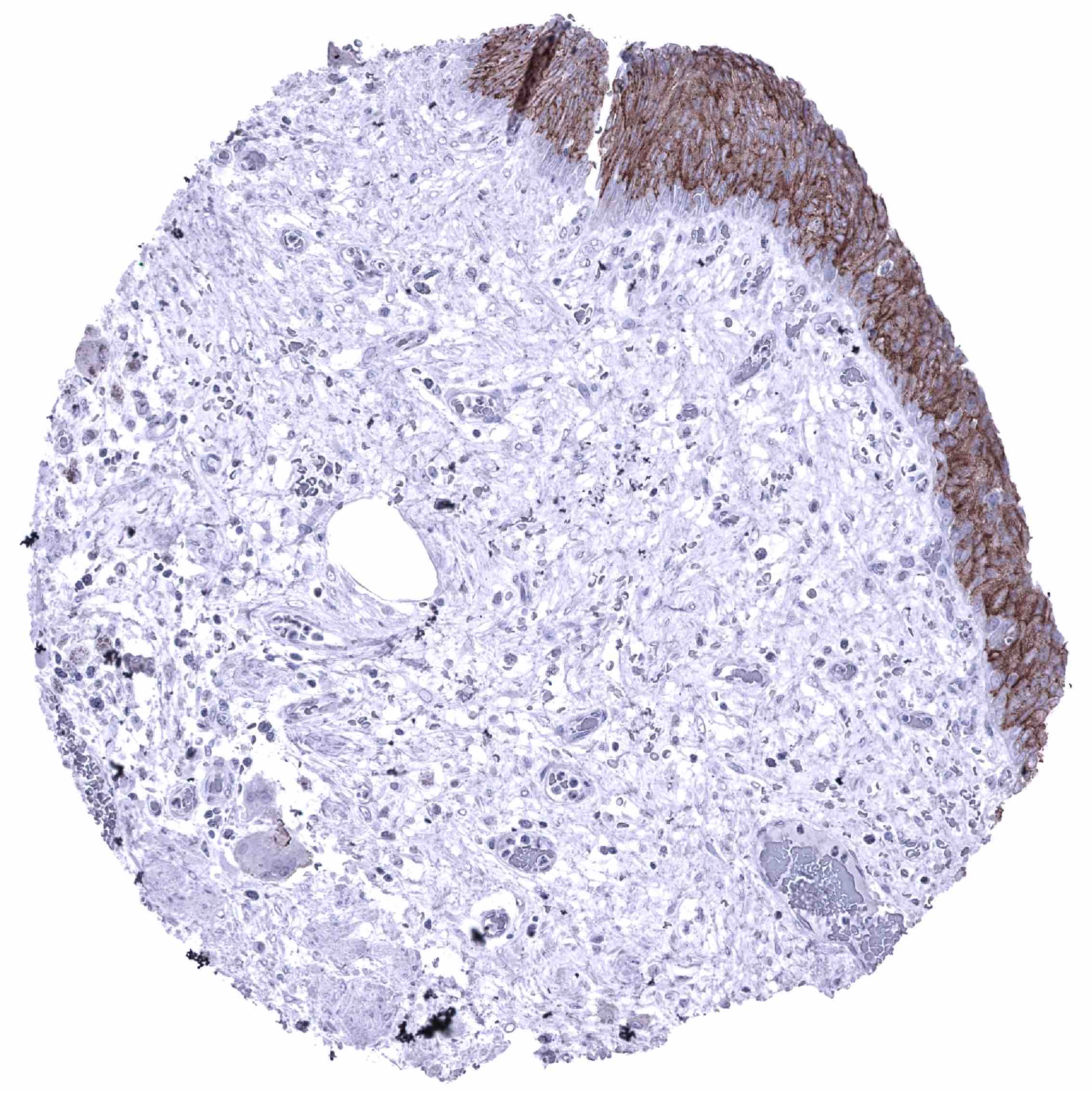
Positive control = Tonsil: A strong membranous Nectin-4 staining must be seen in squamous epithelial cells while inflammatory cells must remain nectin-4 negative.
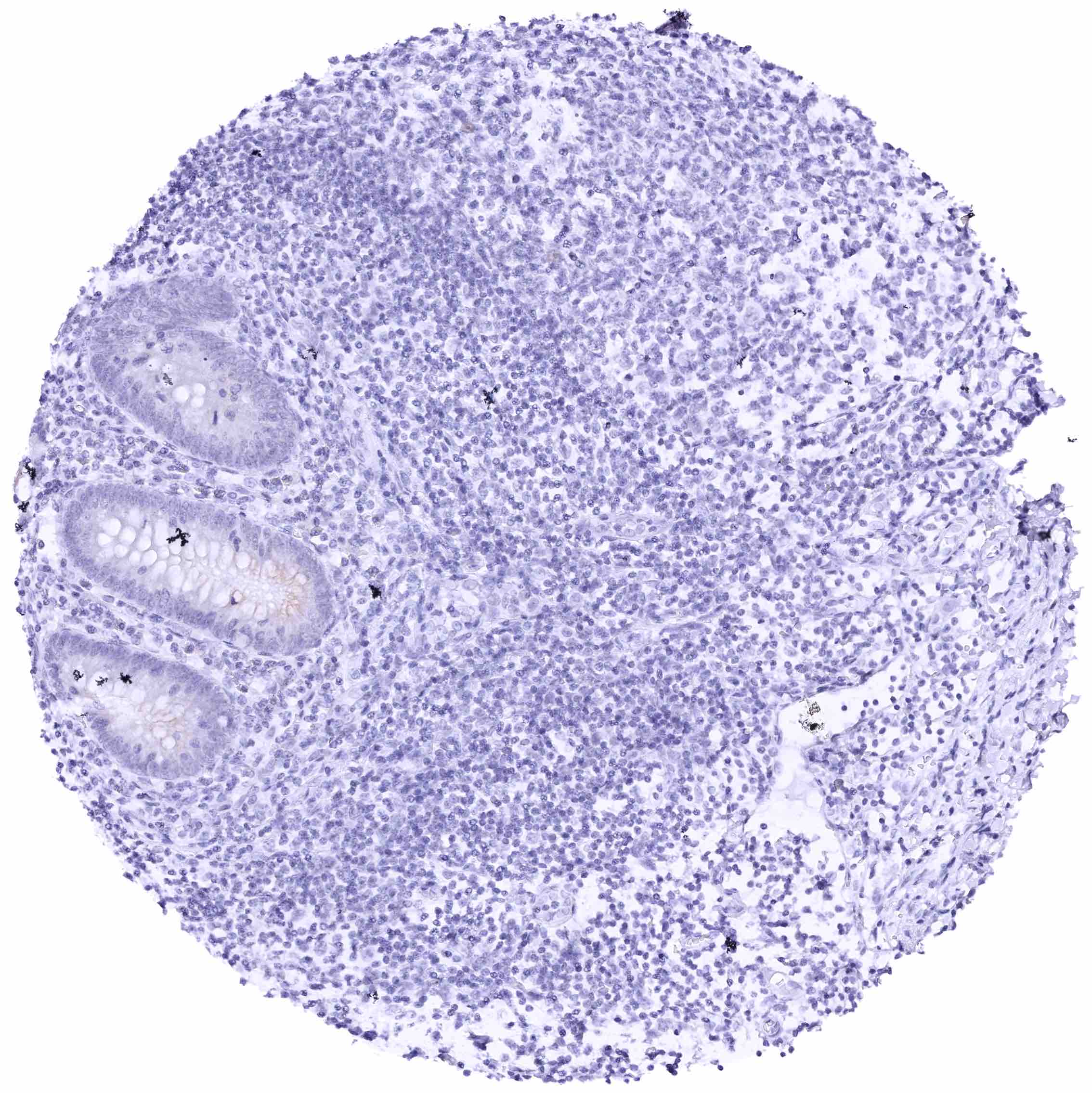
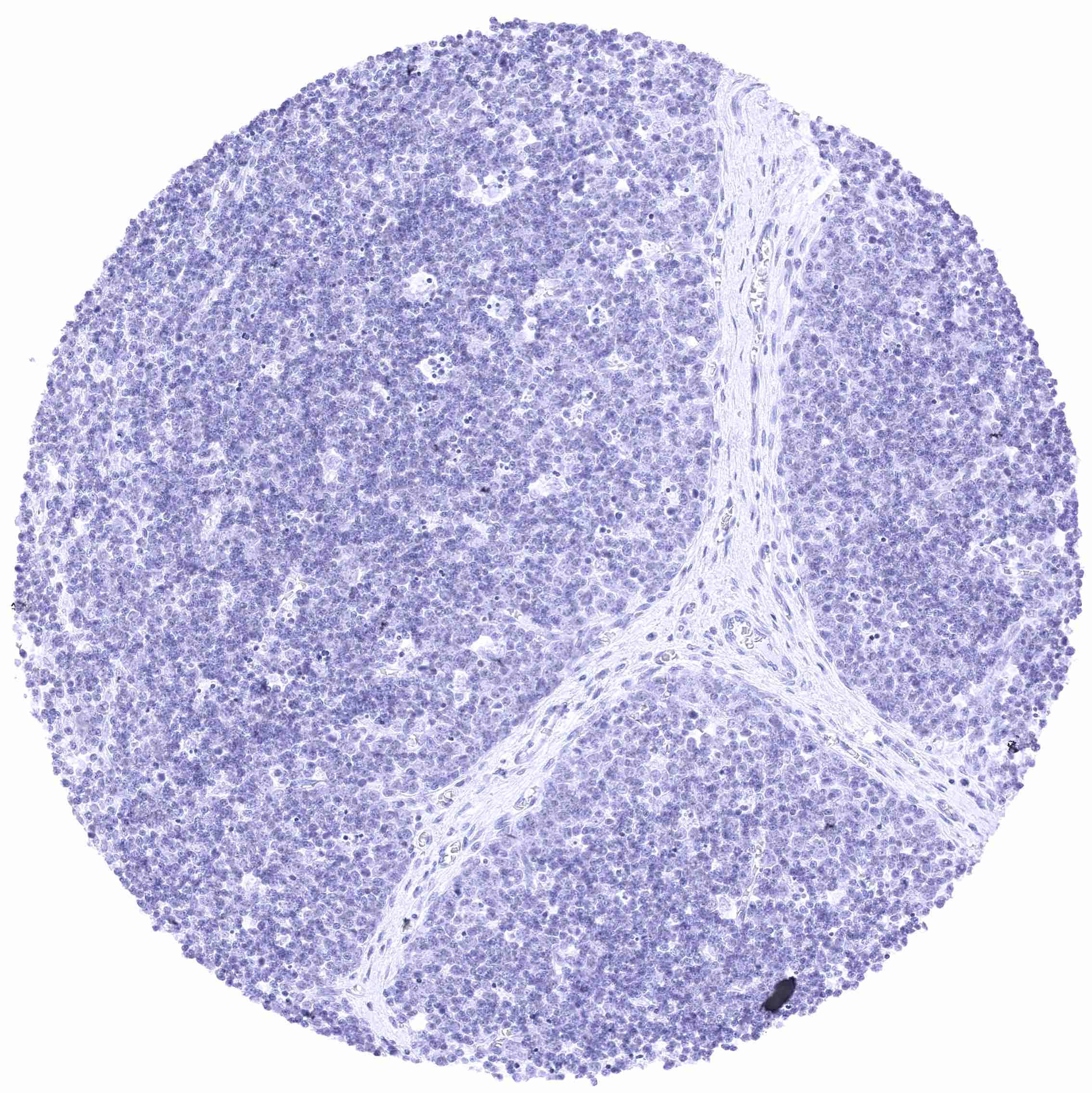
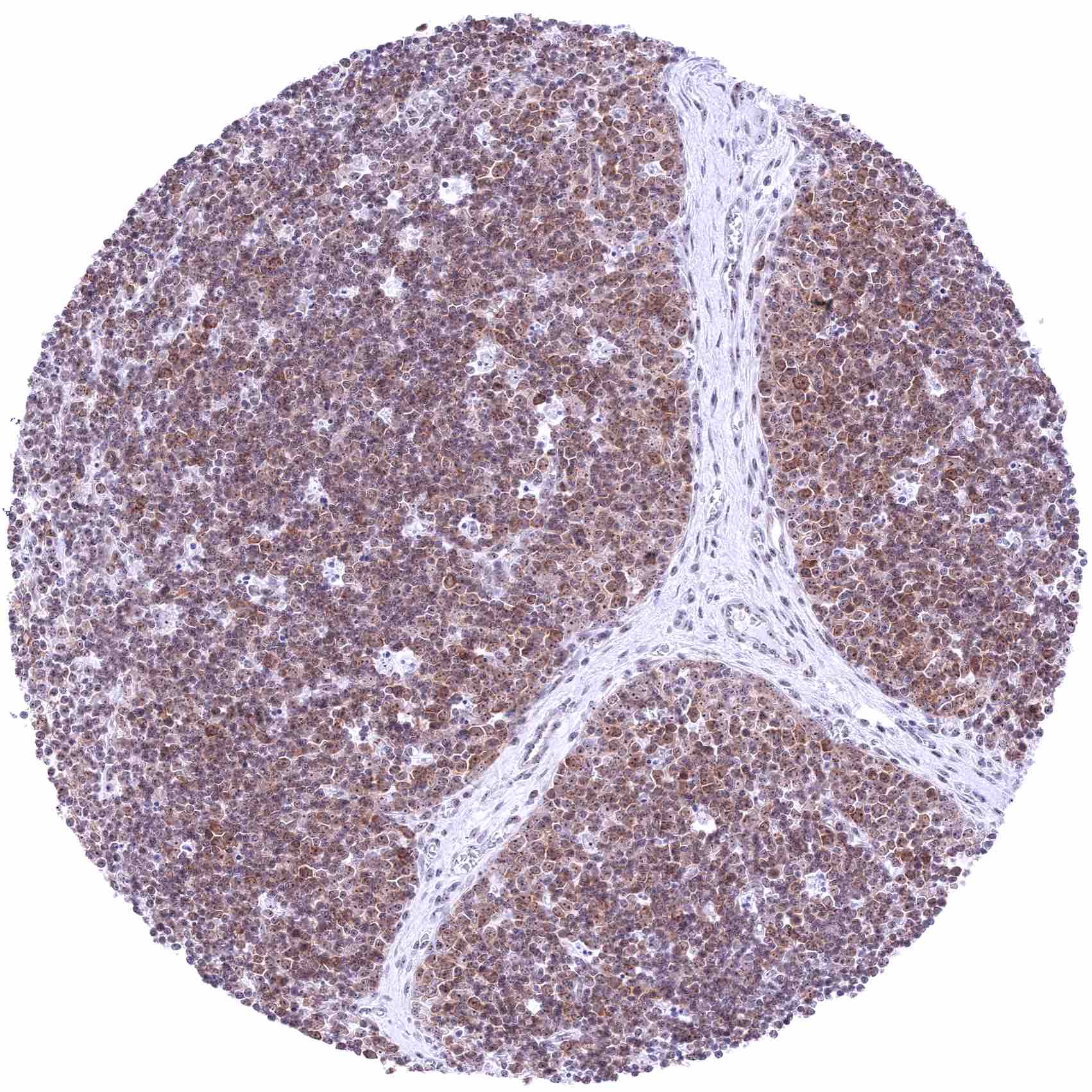
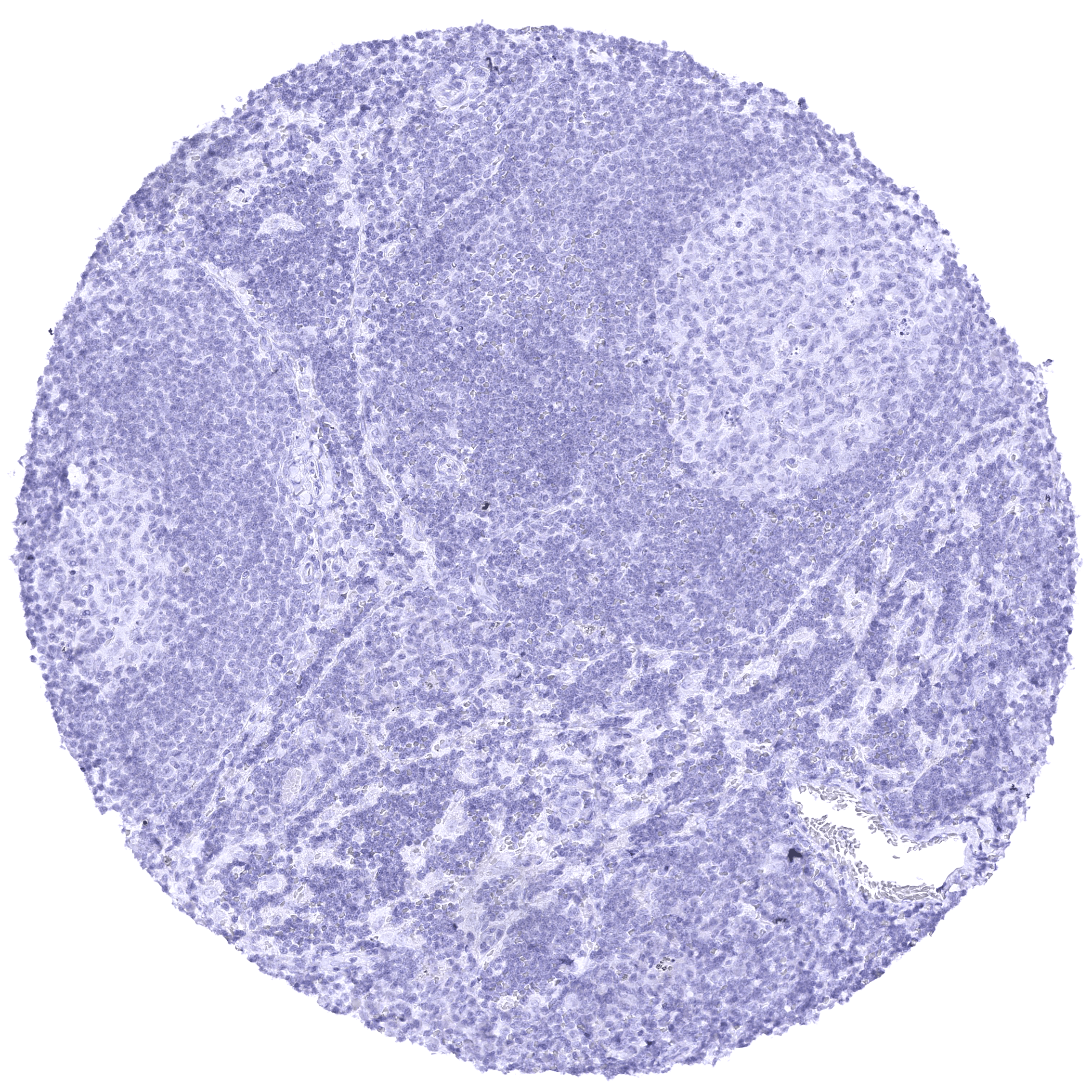
Negative control = Lymph node: All cell types must not show Nectin-4 staining.
Cellular localization = Membranous
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:75 – 1:150
Intended Use = Research Use Only
Relevance of Antibody
NFIX is a therapeutic target protein.
Biology Behind
Nectin-4, also known as Poliovirus receptor-related 4 (PVRL4), is a type I transmembrane protein belonging to the nectin family of immunoglobulin-like adhesion molecules. It is encoded by the PVRL4 gene, located on chromosome 1q23.3. Nectin-4 plays a crucial role in calcium-independent cell-cell adhesion and is involved in several signaling pathways including the PI3K/AKT and the JAK2–STAT5a pathways. Based on these interactions, Nectin-4 is involved in the regulation of migration, adhesion, and proliferation of tumor cells. In several cancer entities, unfavorable prognosis has been described for nectin-4 positive cancers. Nectin-4 also has a soluble form which is established by shedding of the entire nectin-4 extracellular domain. Nectin-4 shedding especially occurs in case of cellular hypoxia. Soluble nectin-4 interacts with integrin-β4 on endothelial cells and thereby promotes angiogenesis by activation of several signaling pathways including PI3K/AKT. Most of the current interest in nectin-4 is driven by its role as a drug target for enfortumab vedotin (EV) which has been FDA approved for advanced urothelial carcinoma. EV and several other anti-nectin-4 drugs are currently being further investigated in clinical trials on bladder cancer and several other tumor entities.
Staining Pattern in Normal Tissues
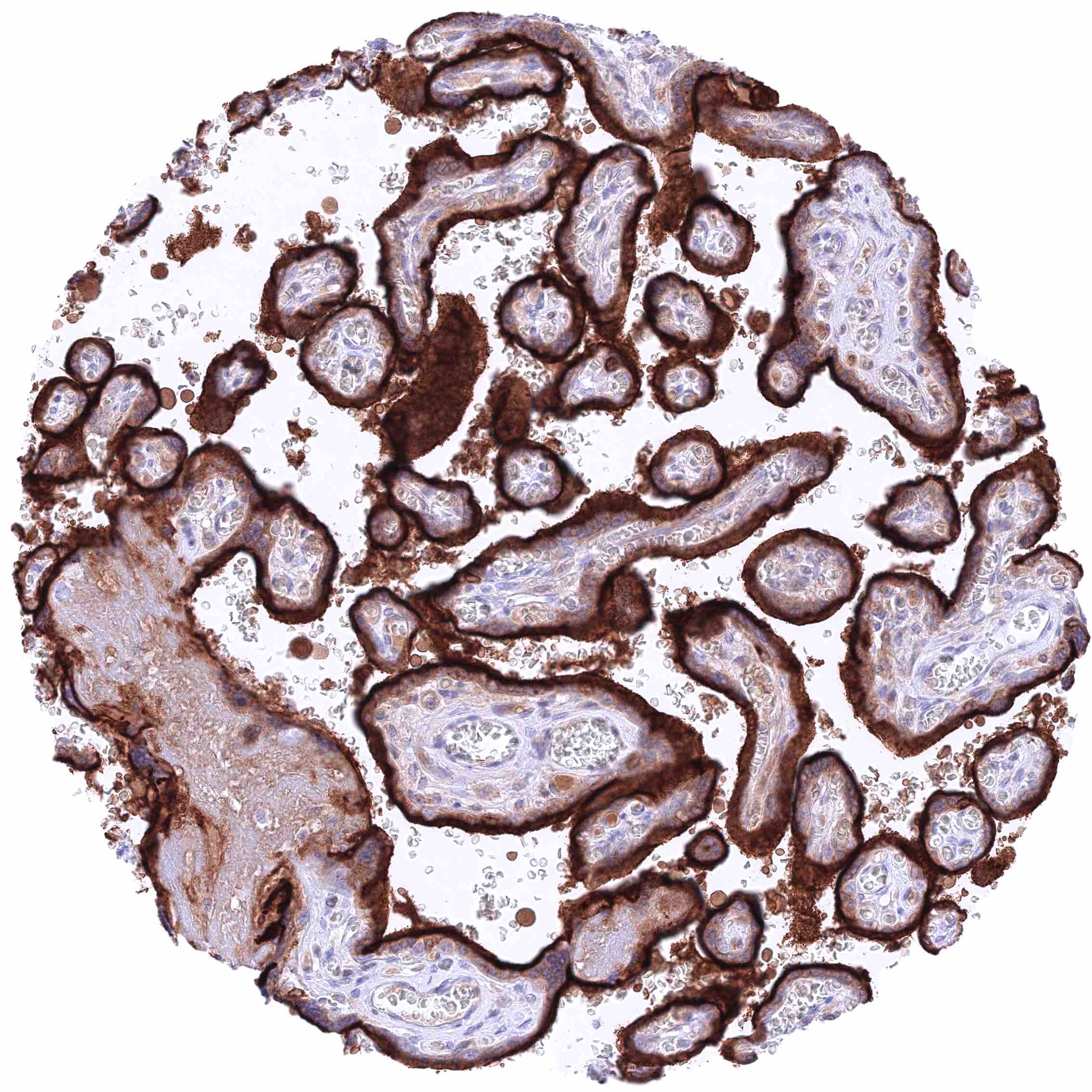
Nectin-4 expression most prominently occurs in squamous epithelium, urothelium, and in salivary glands but can also occur in other tissues and cell types. By IHC, nectin-4 staining is especially intense in luminal membranes of the syncytiotrophoblast of the placenta. Images describing the Nectin-4 staining pattern in normal tissues obtained by the antibody MSVA-304M are shown in our “Normal Tissue Gallery”.
| Brain | Cerebrum | Negative. |
| Cerebellum | Negative. | |
| Endocrine Tissues | Thyroid | Negative. |
| Parathyroid | Negative. | |
| Adrenal gland | Negative. | |
| Pituitary gland | Negative. | |
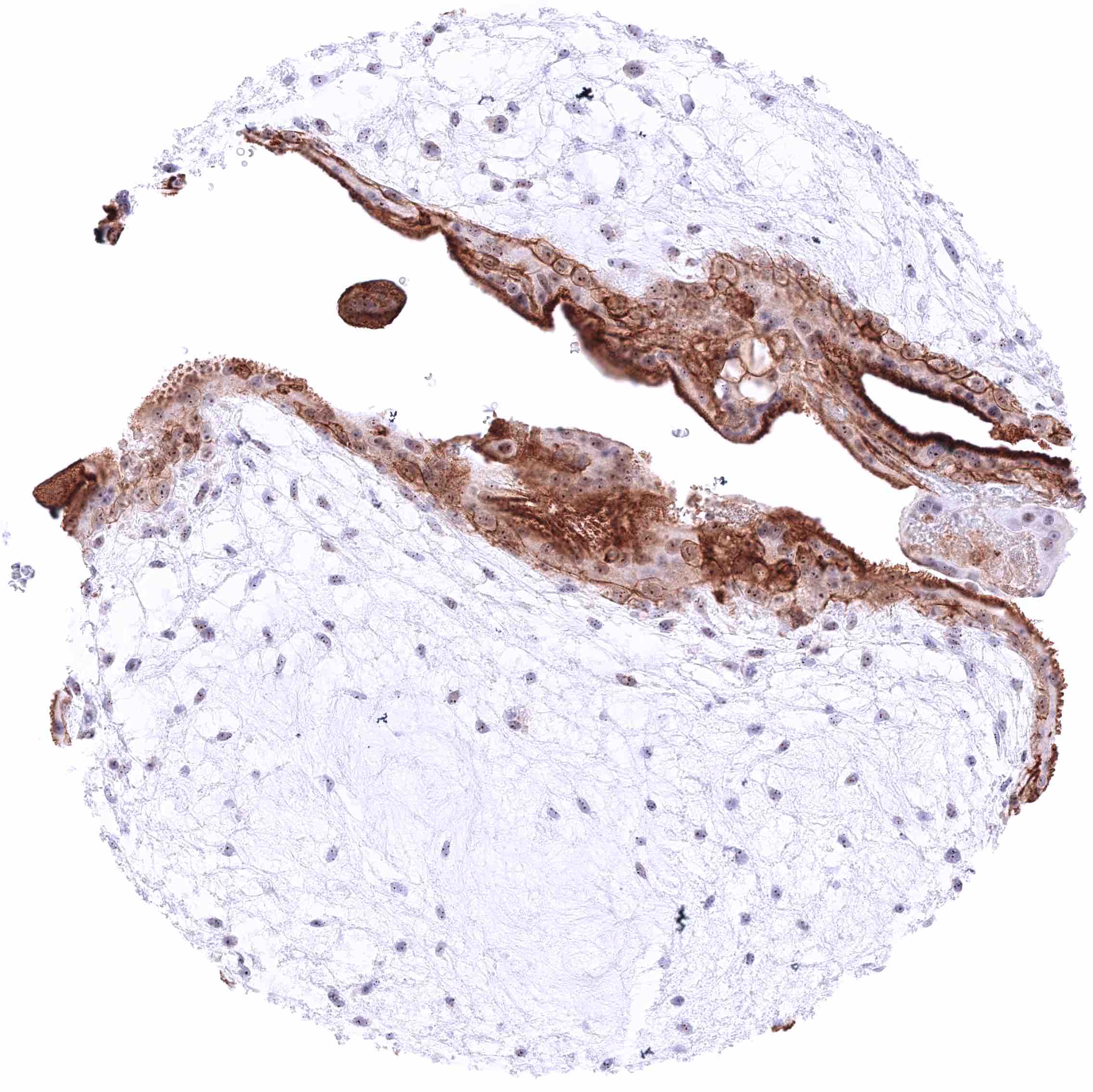
| Respiratory system | Bronchus, Respiratory epithelium | Weak to moderate membranous nectin-4 staining of ciliated cells (most prominent at the lateral membranes). |
| Lung | Moderate to strong membranous nectin-4 staining of at least a fraction of bronchiolar epithelial cells. Pneumocytes are nectin-4 negative. | |
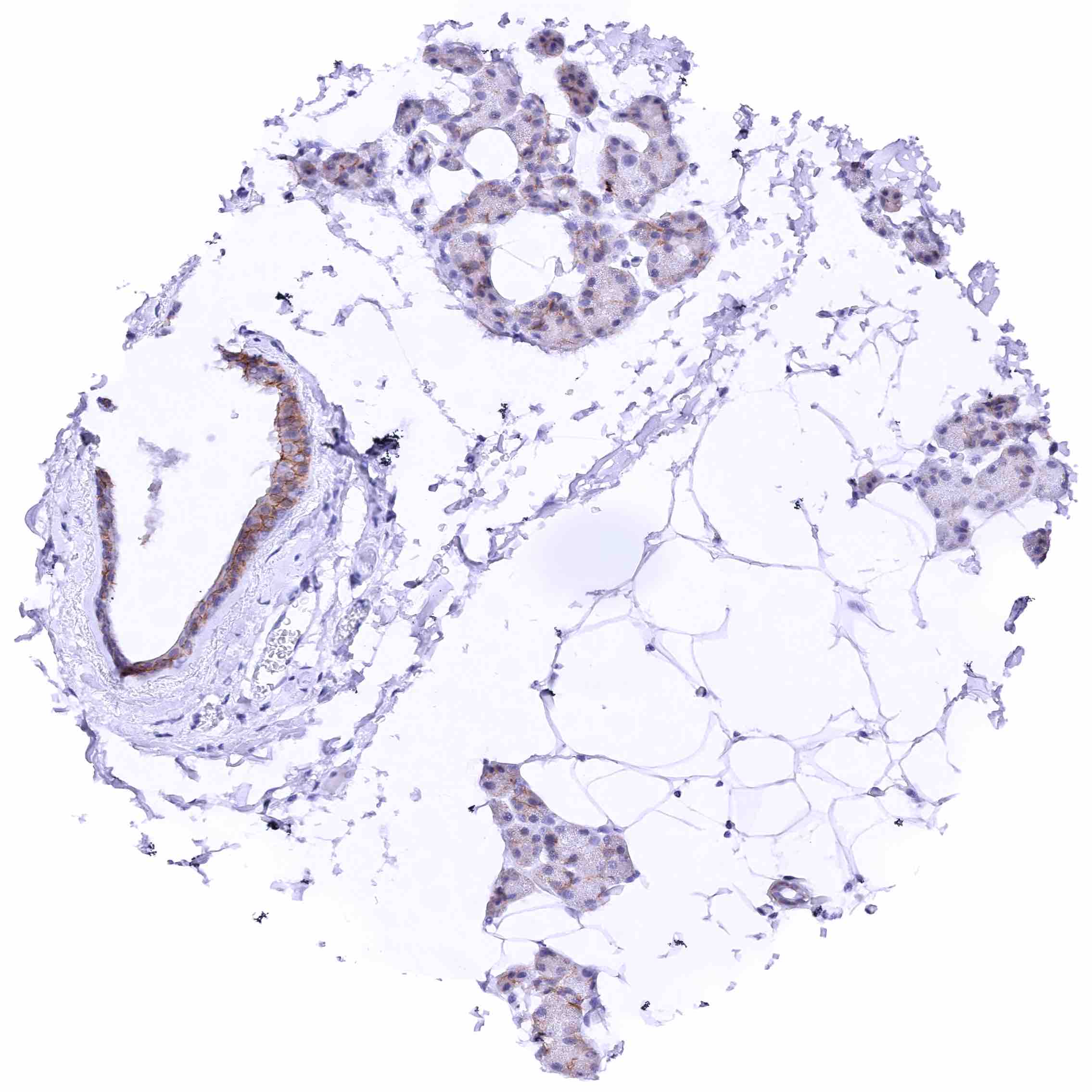
| Gastrointestinal Tract | Salivary glands | Membranous nectin-4 staining of variable intensity of excretory duct cells (negative to strong) and glandular cells. At least in some samples, a strong nectin-4 of at least a subset of myoepithelial cells along glands and excretory ducts is also seen. Staining of excretory ducts is often more intense than of glands. |
| Esophagus | Nectin-4 staining of squamous epithelium is strong in the suprabasal cell layers while the staining intensity decreases markedly towards the superficial cell layers where cells are often negative. Basal cells are nectin-4 negative. | |
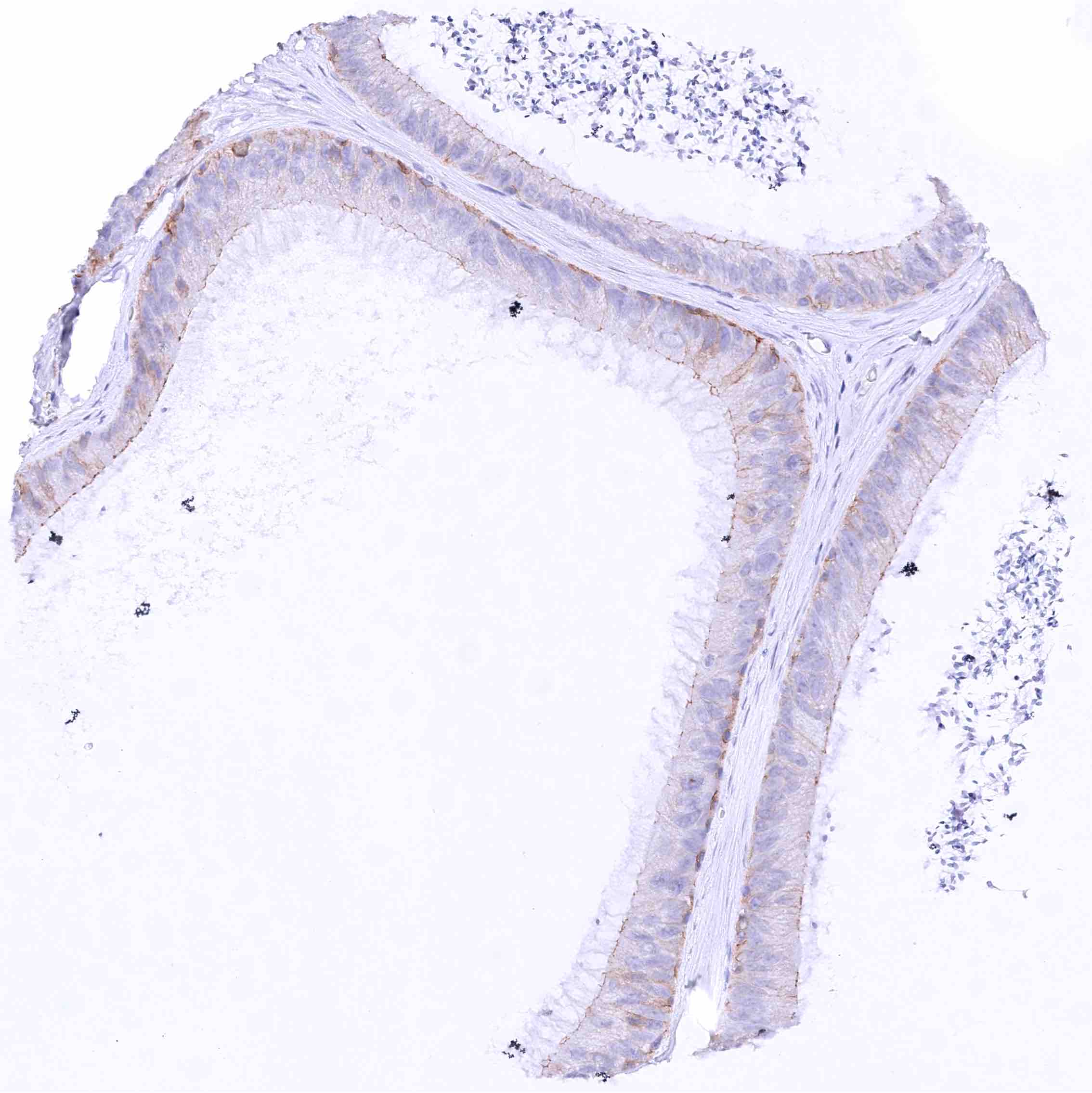
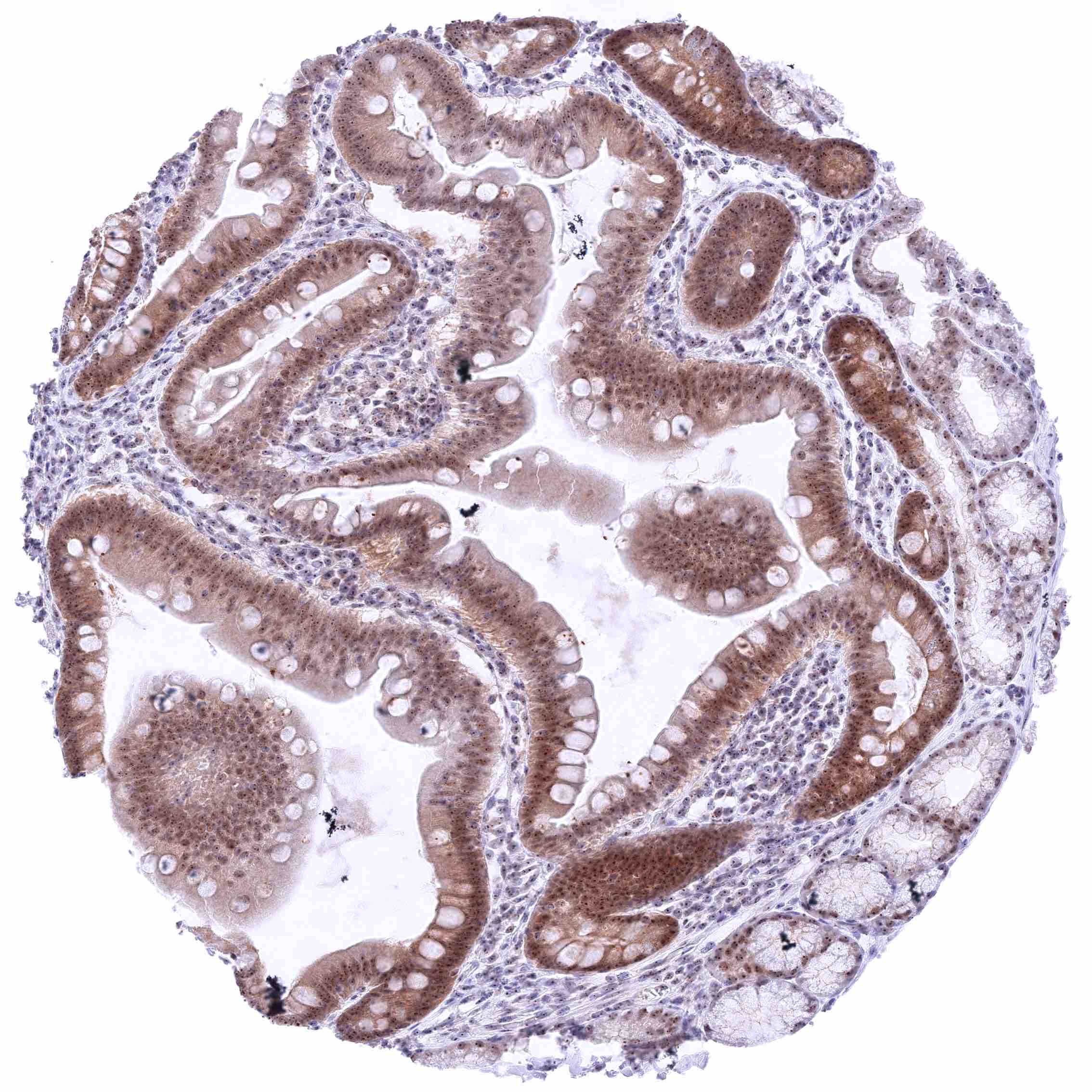
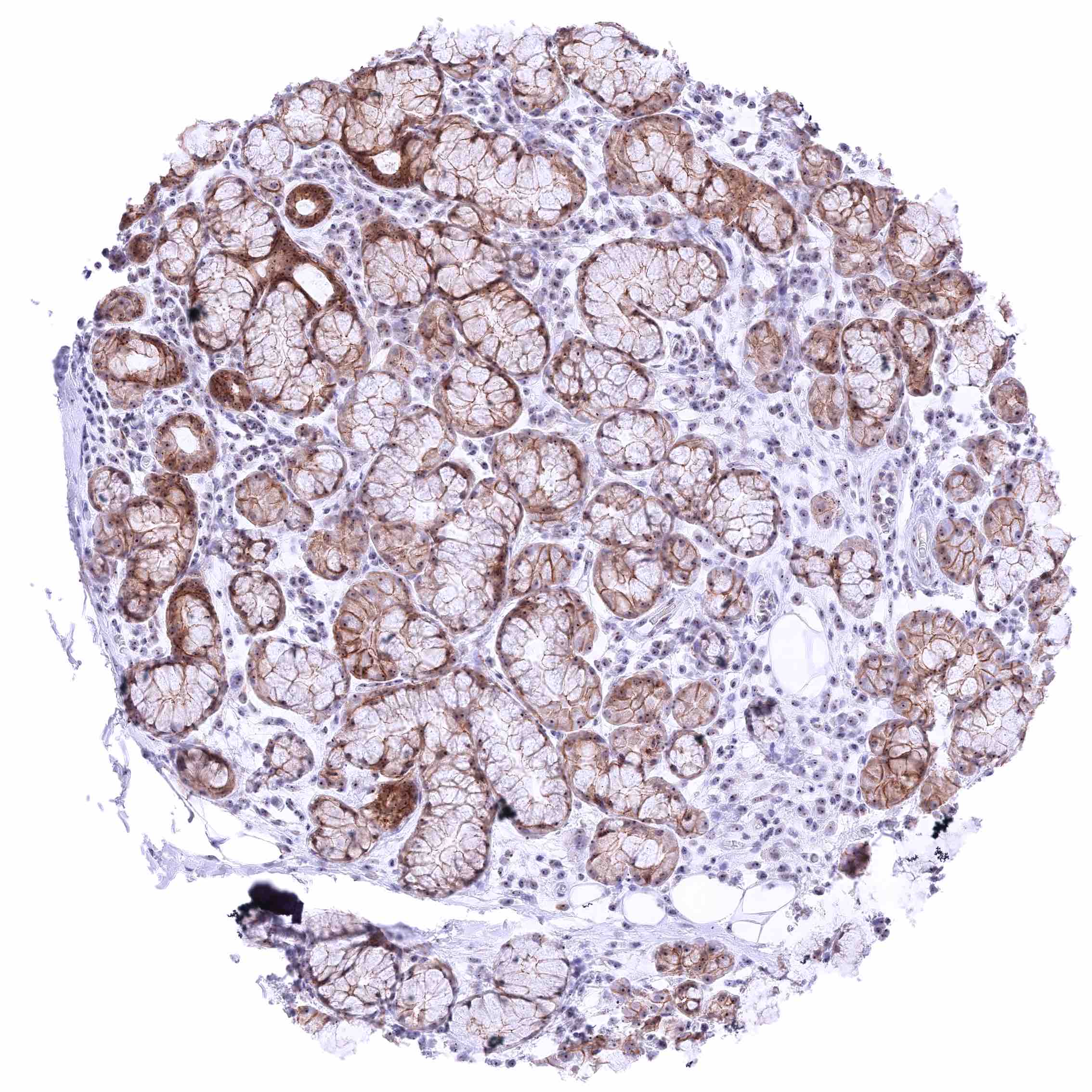
| Stomach | Moderate membranous nectin-4 staining of surface epithelial cells (most prominent at the lateral membranes). Gastric glands are mostly negative or show minimal staining. | |
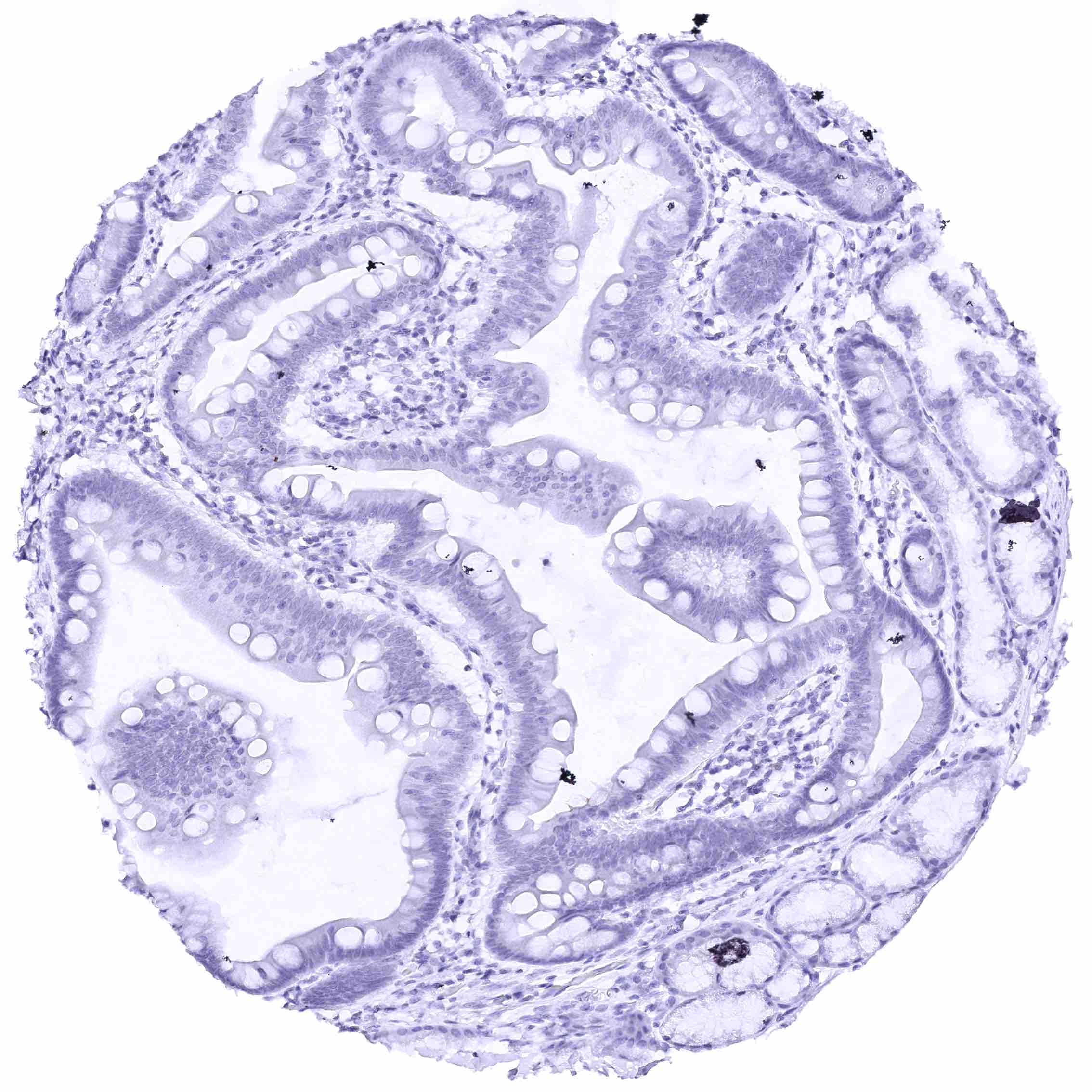
| Duodenum | Negative. | |
| Small intestine | Negative. | |
| Appendix | Negative. | |
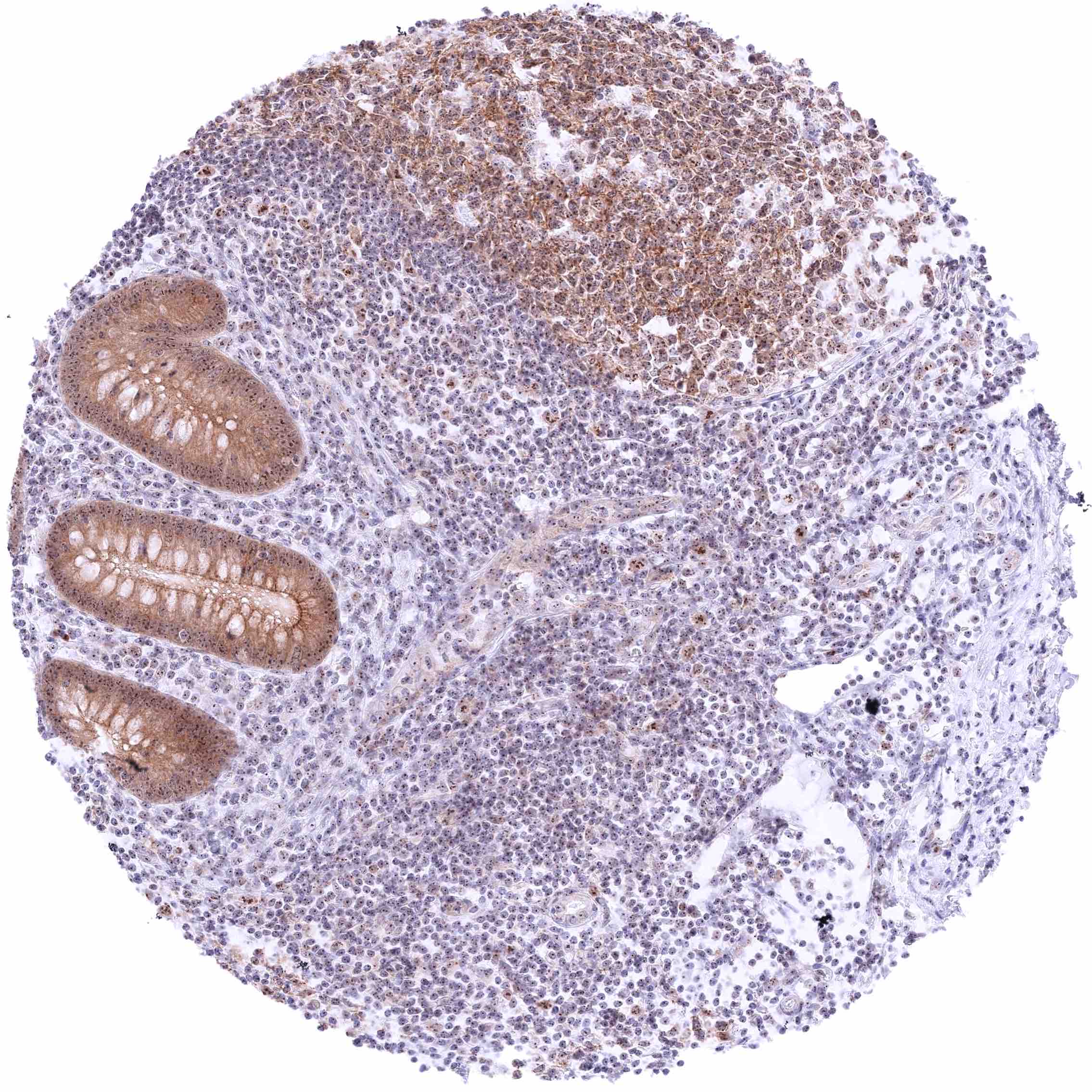
| Colon | Negative. | |
| Rectum | Negative. | |
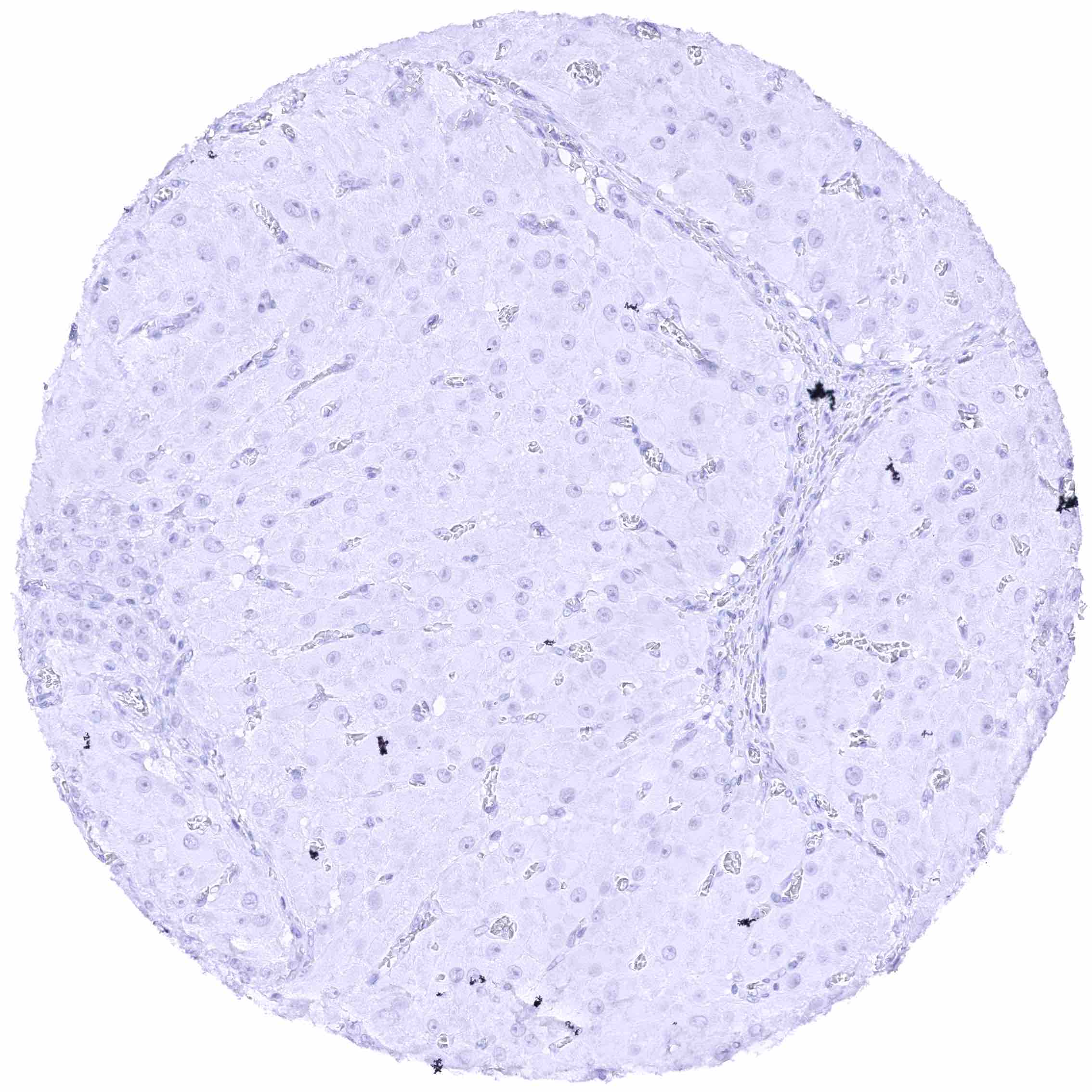
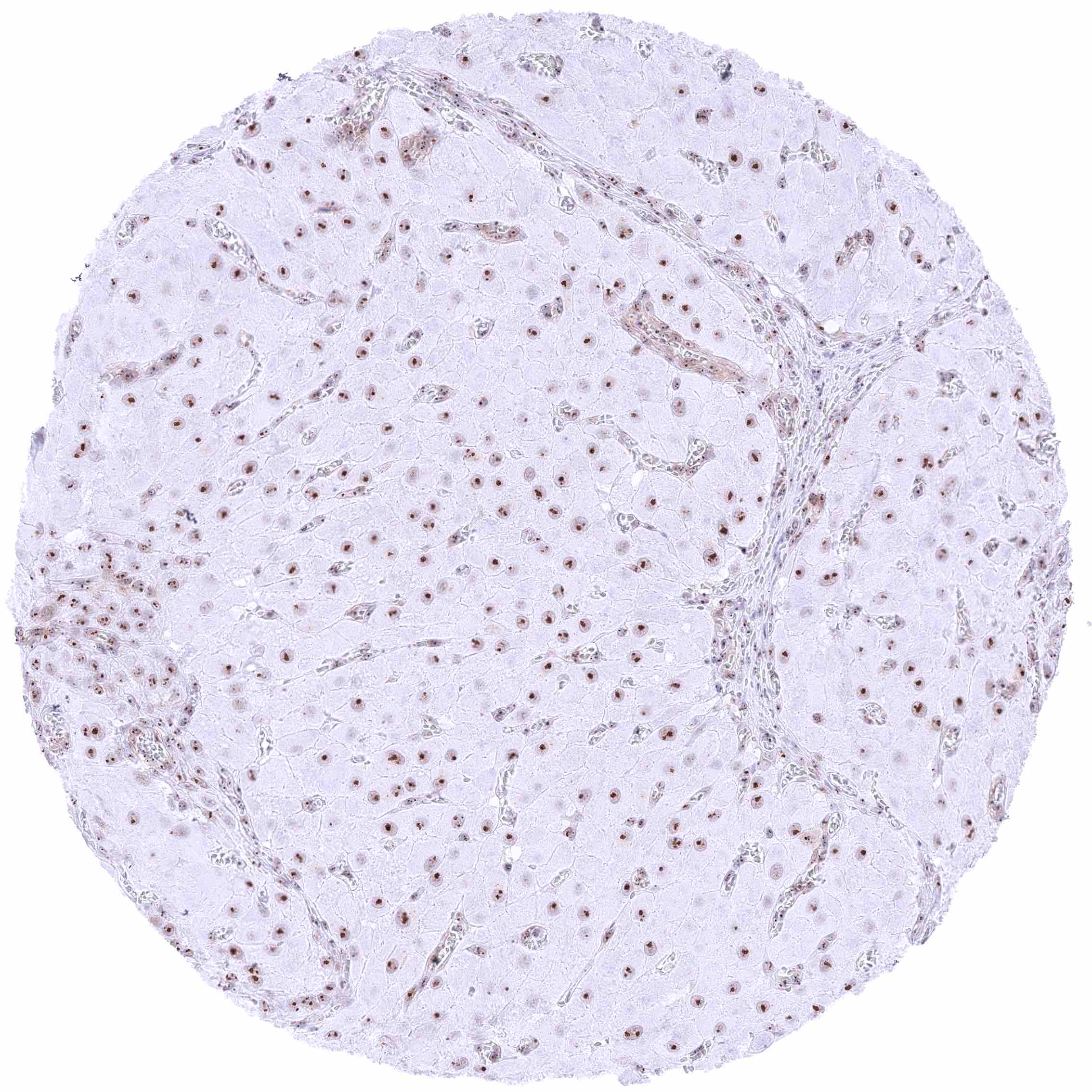
| Liver | Negative. | |
| Gallbladder | Weak to moderate membranous nectin-4 staining of epithelial cells (most prominent at the lateral membranes). | |
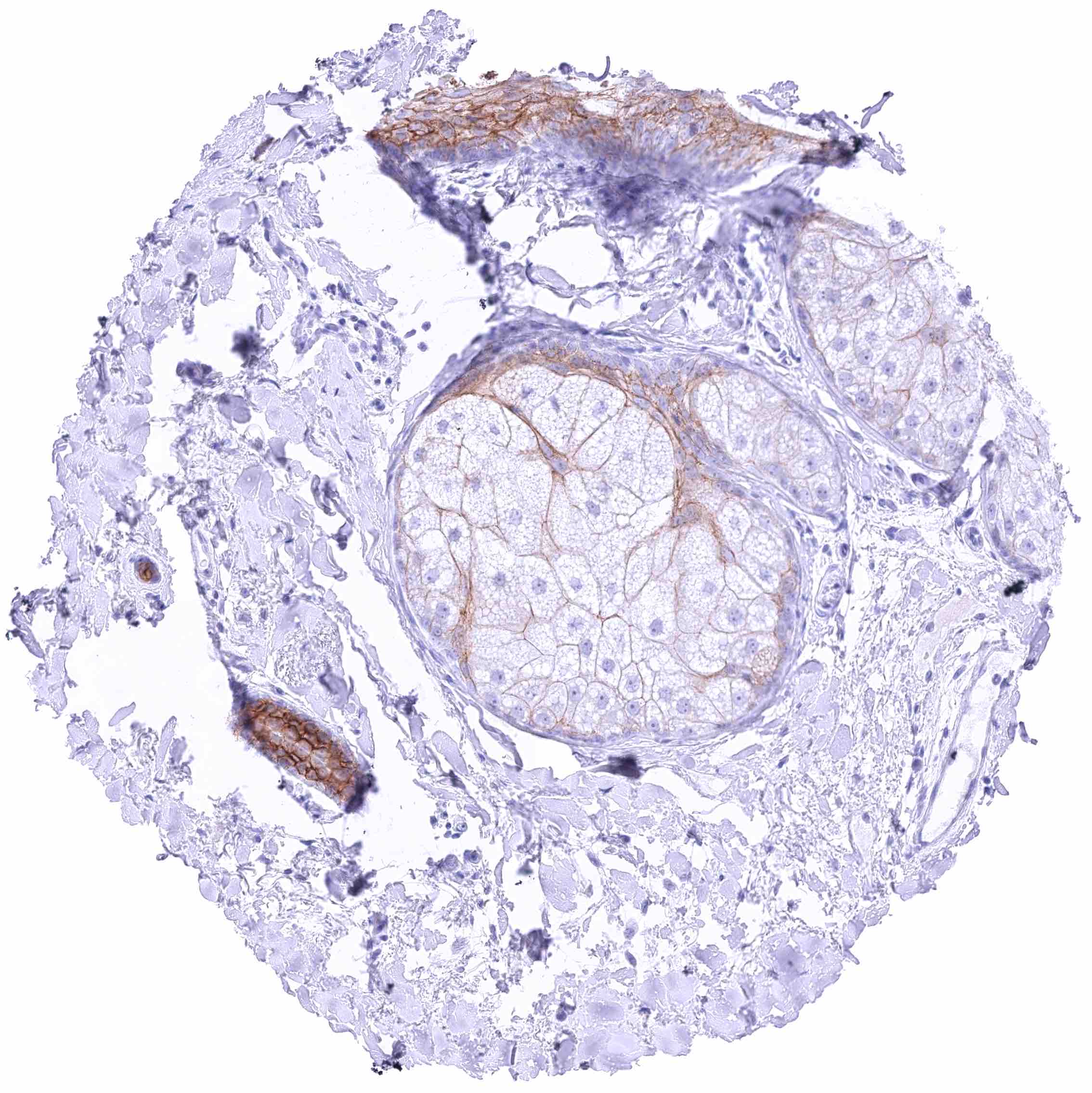
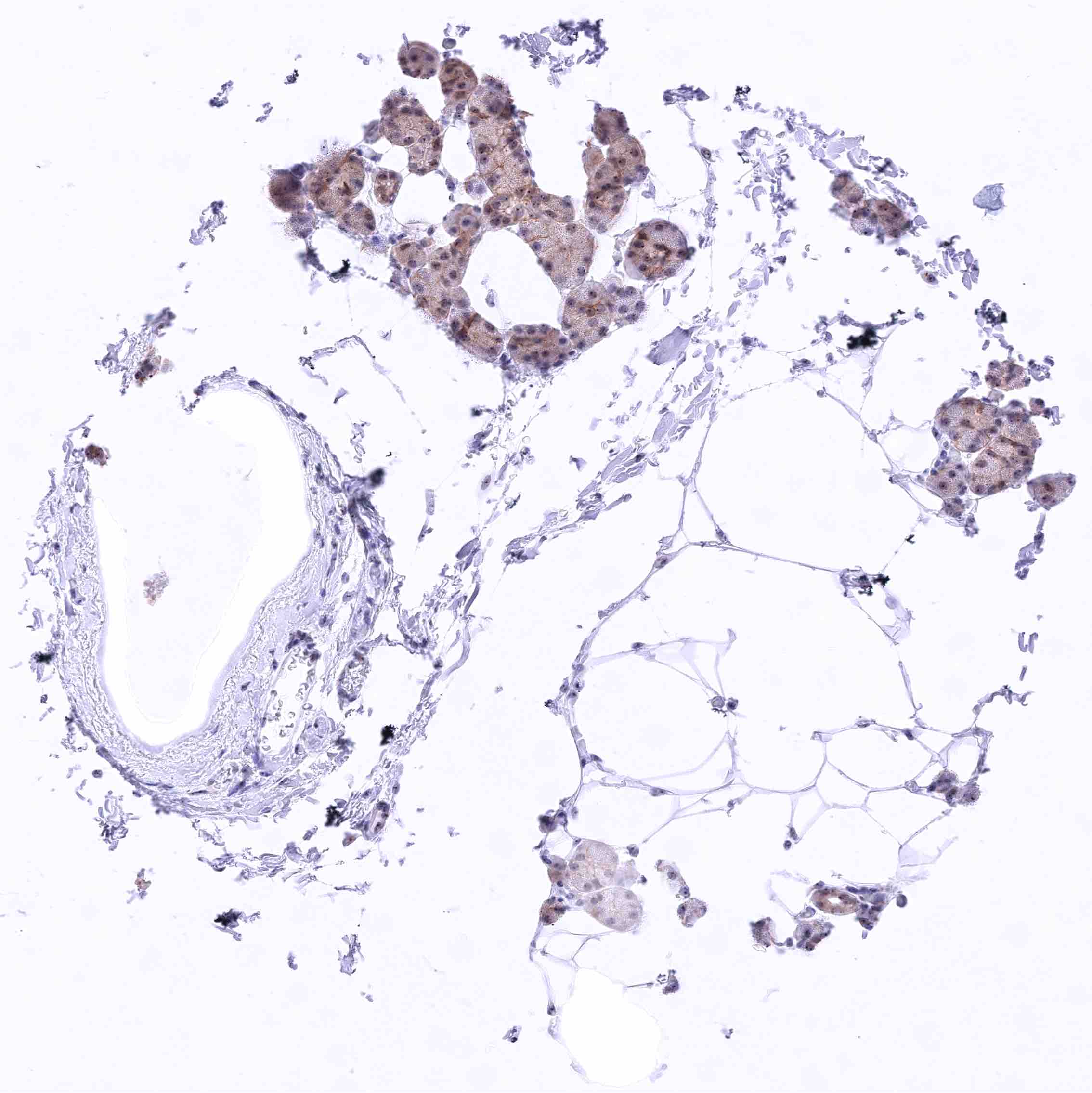
| Pancreas | Faint nectin-4 staining of luminal membranes of some acinar cells and/or intercalated ducts. Islet cells are nectin-4 negative. | |
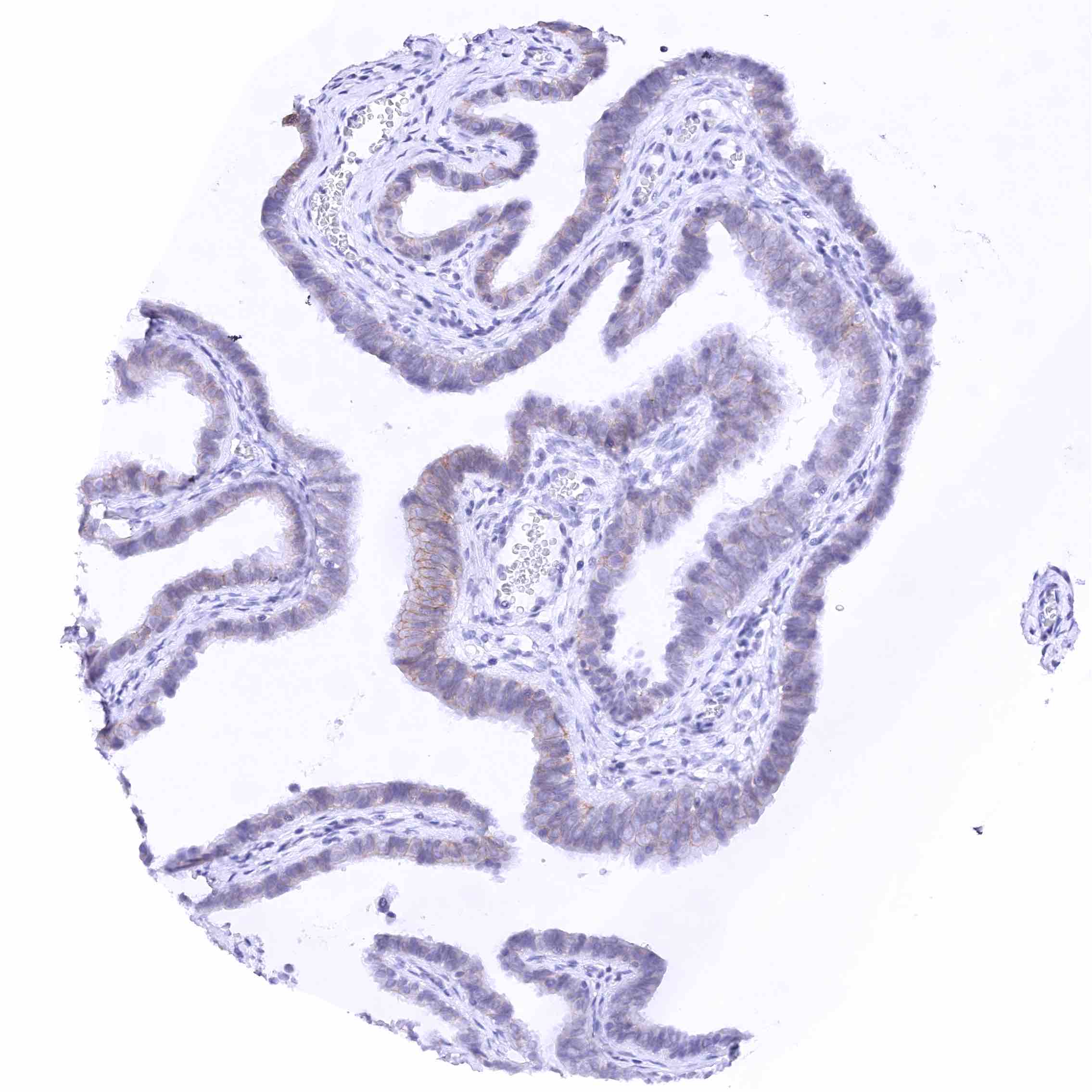
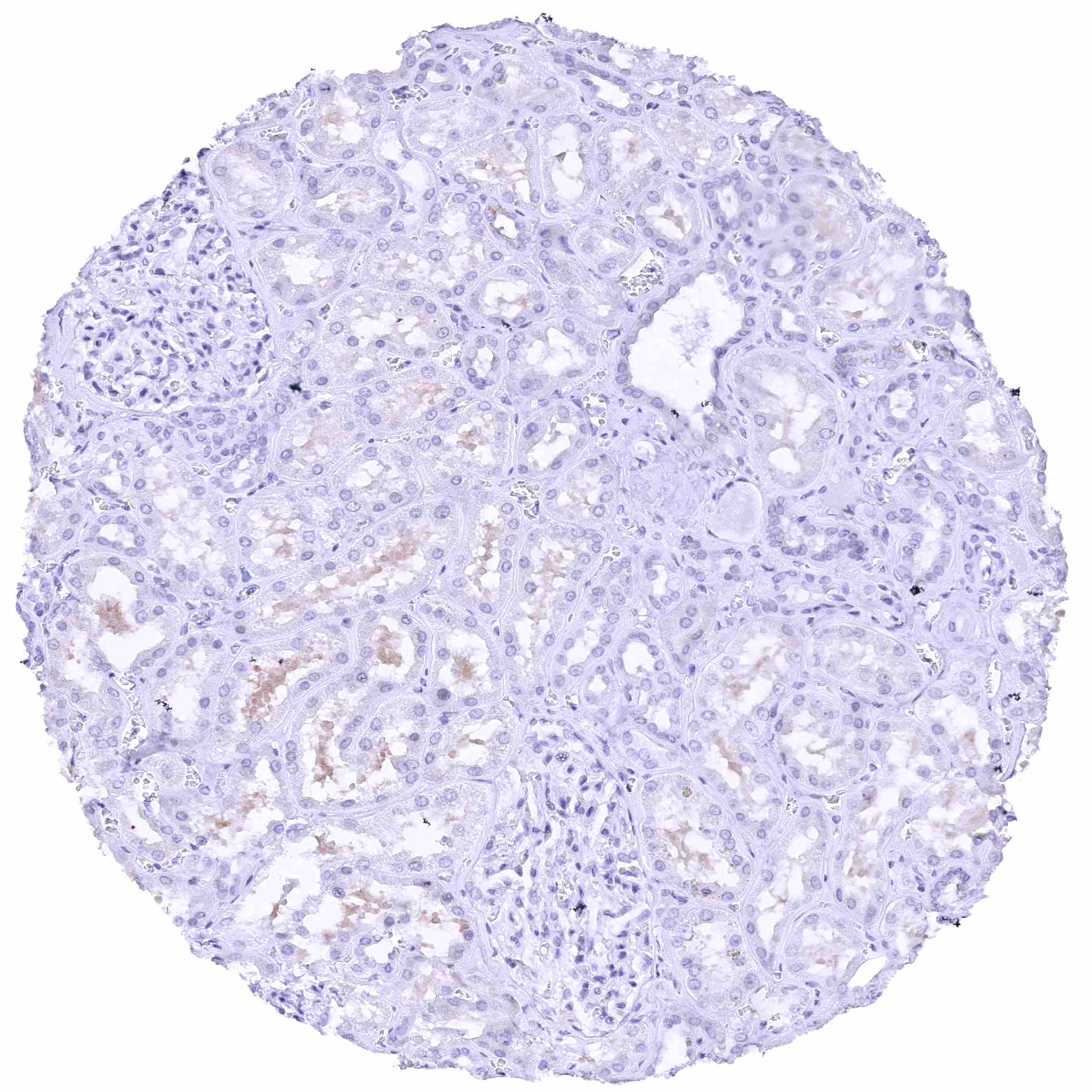
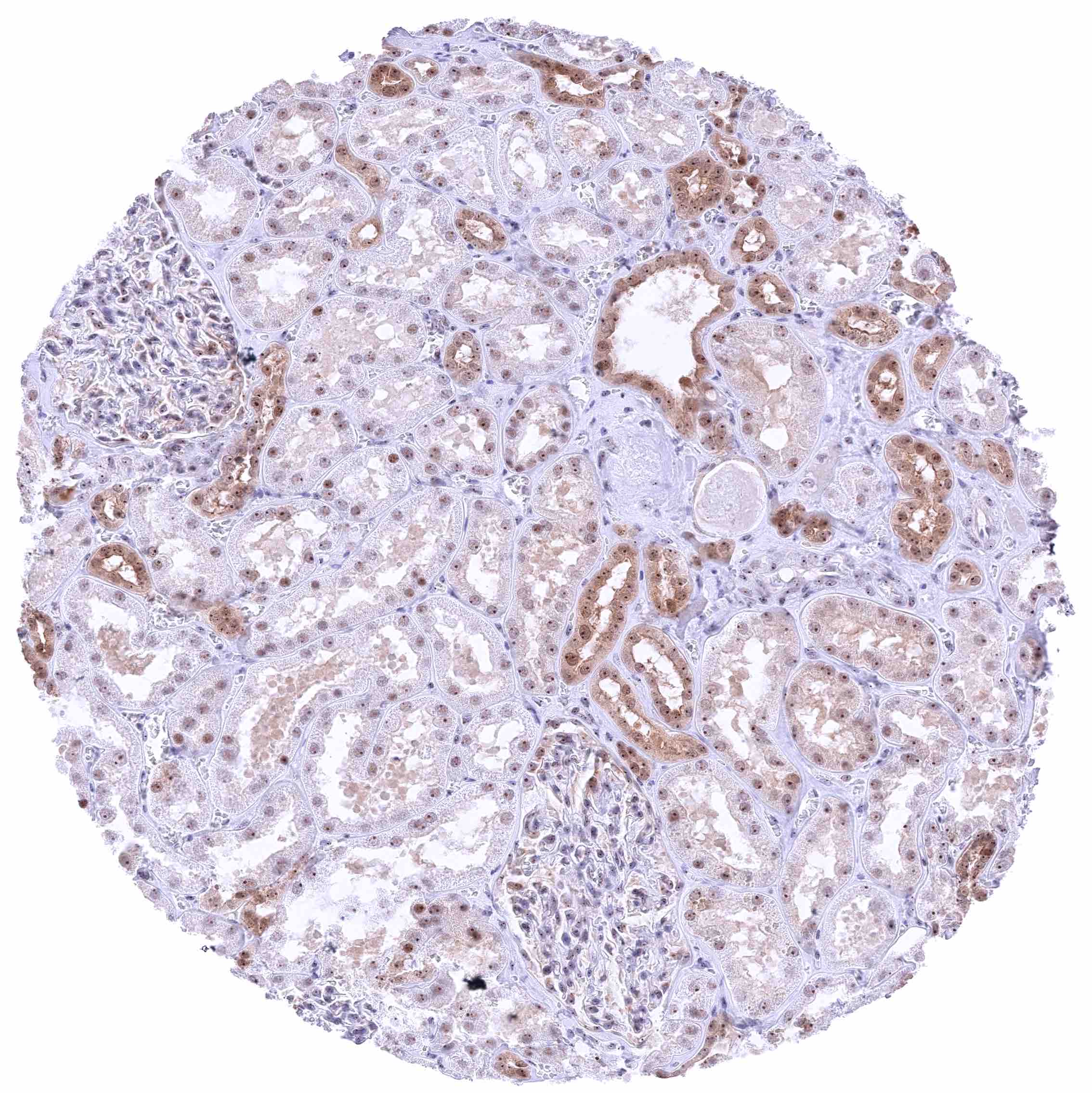
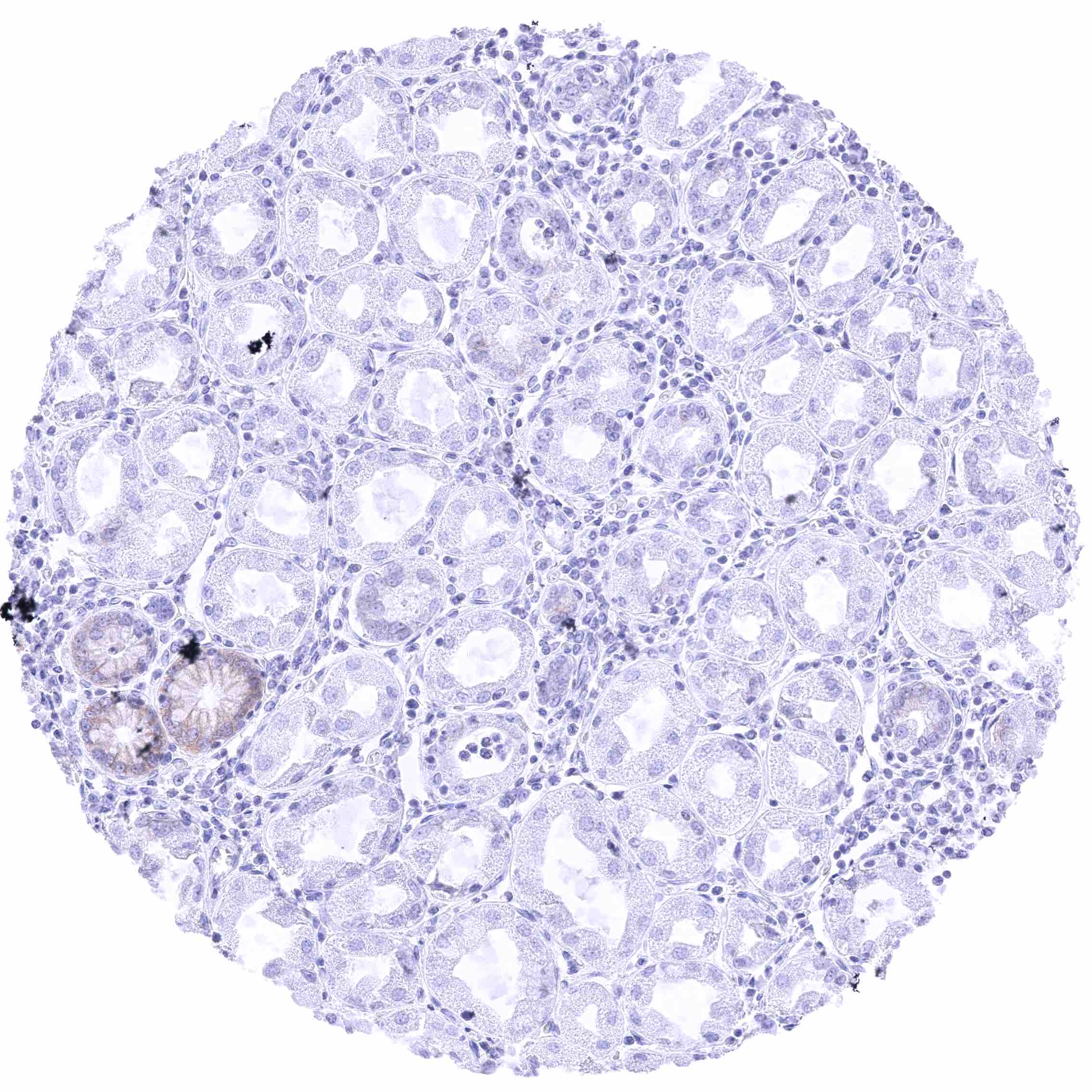
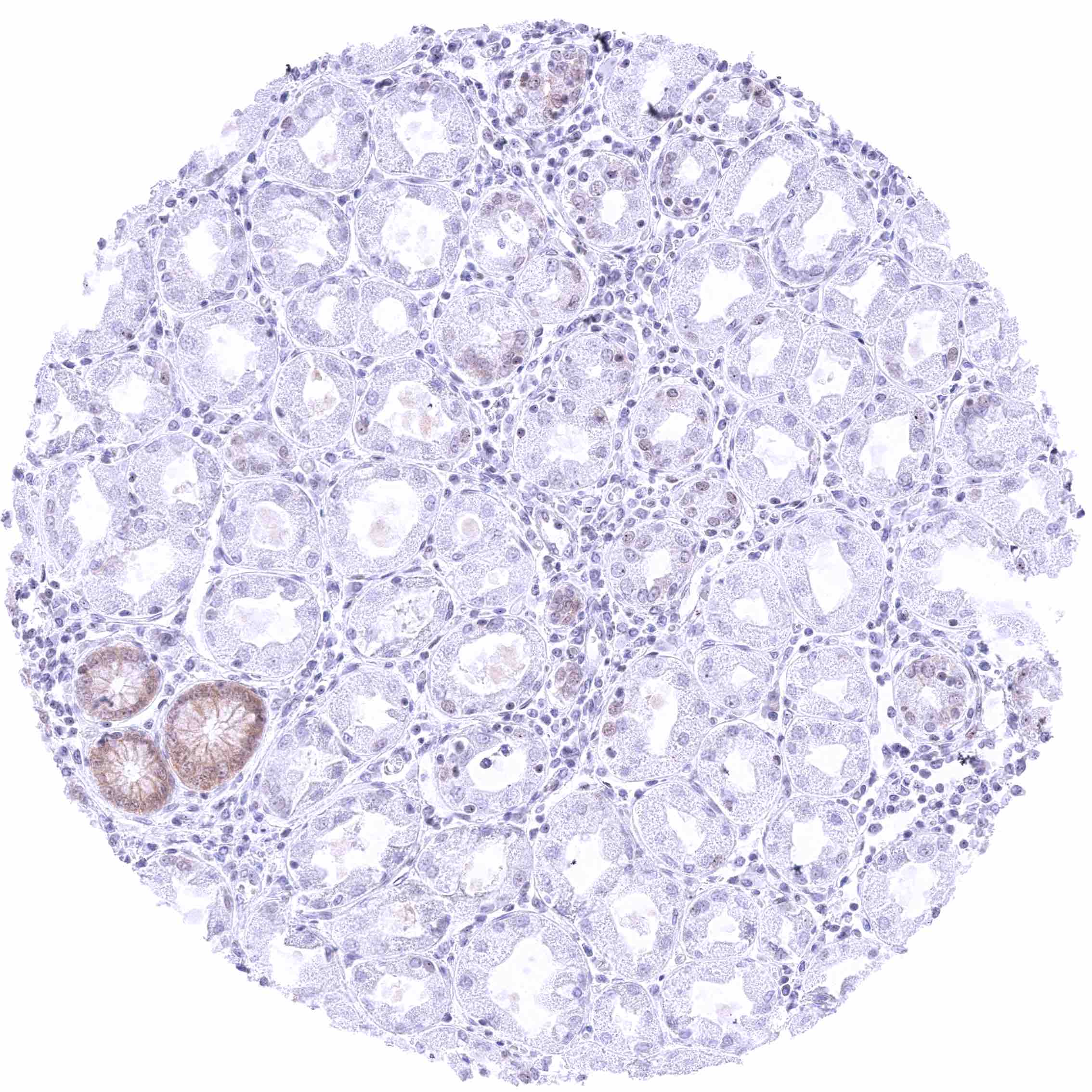
| Genitourinary | Kidney | Weak to moderate membranous nectin-4 staining of some flat tubular structures in the renal cortex (distal tubuli vs. atrophic tubuli vs. collecting ducts). |
| Urothelium | Strong membranous nectin-4 staining of urothelial cells. Staining is sometimes inhomogeneous with strongest positivity in suprabasal cell layers. Basal cells are always nectin-4 negative. | |
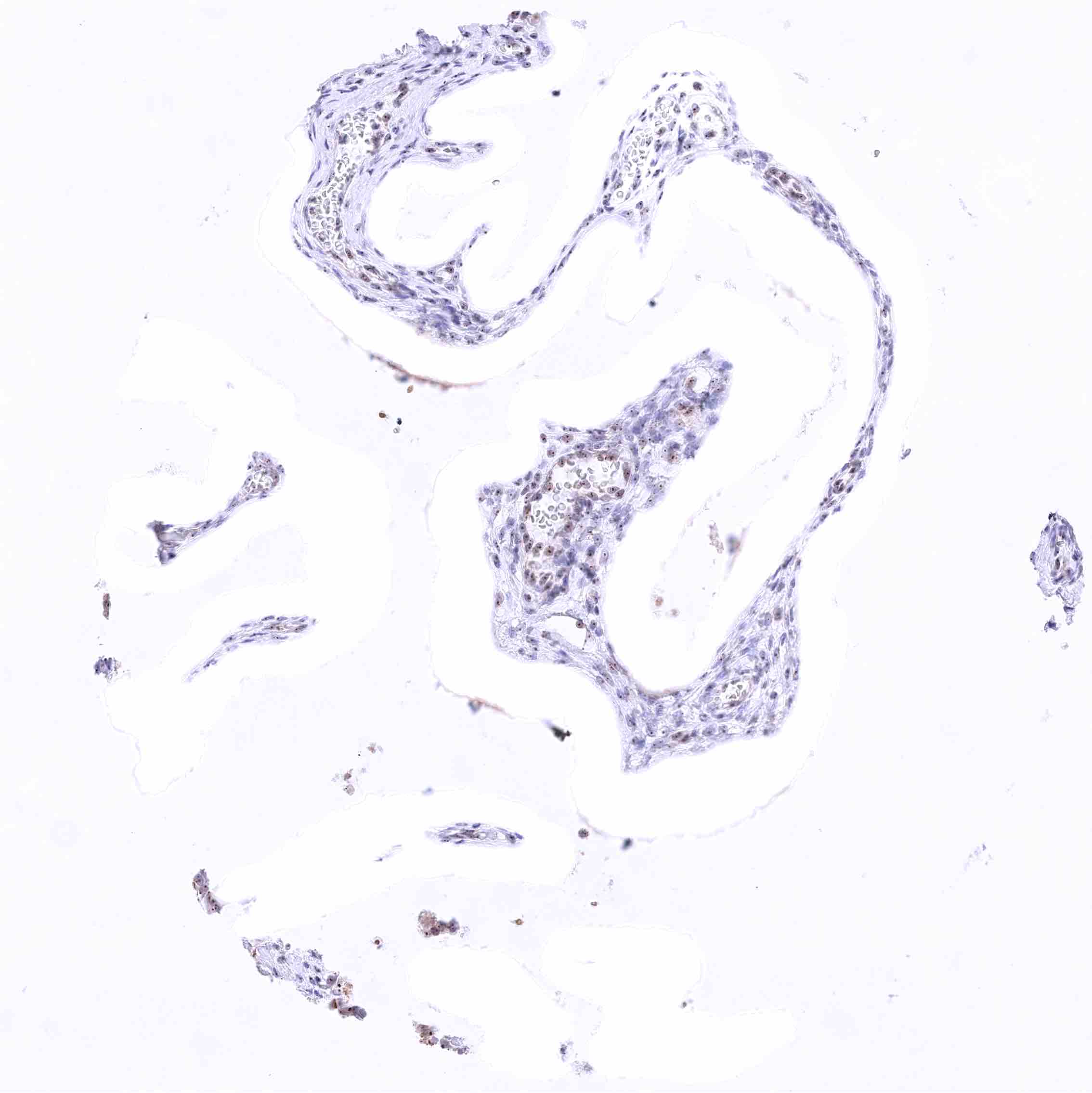
| Male genital | Prostate | A focal weak to moderate membranous nectin-4 staining of acinar cells can occur, especially in areas with atrophic glands. |
| Seminal vesicles | Moderate membranous nectin-4 staining of a subset of epithelial cells. | |
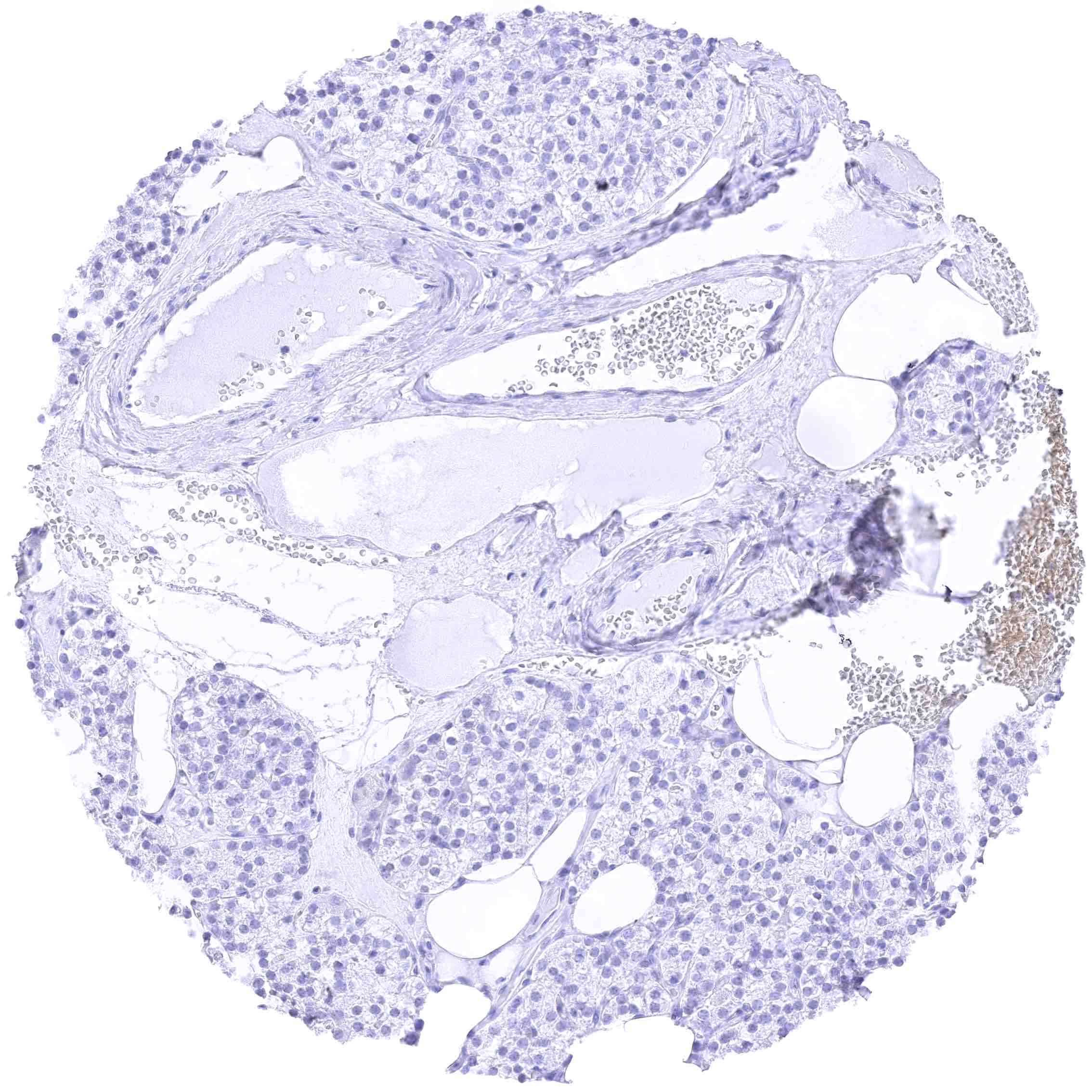
| Testis | Negative. | |
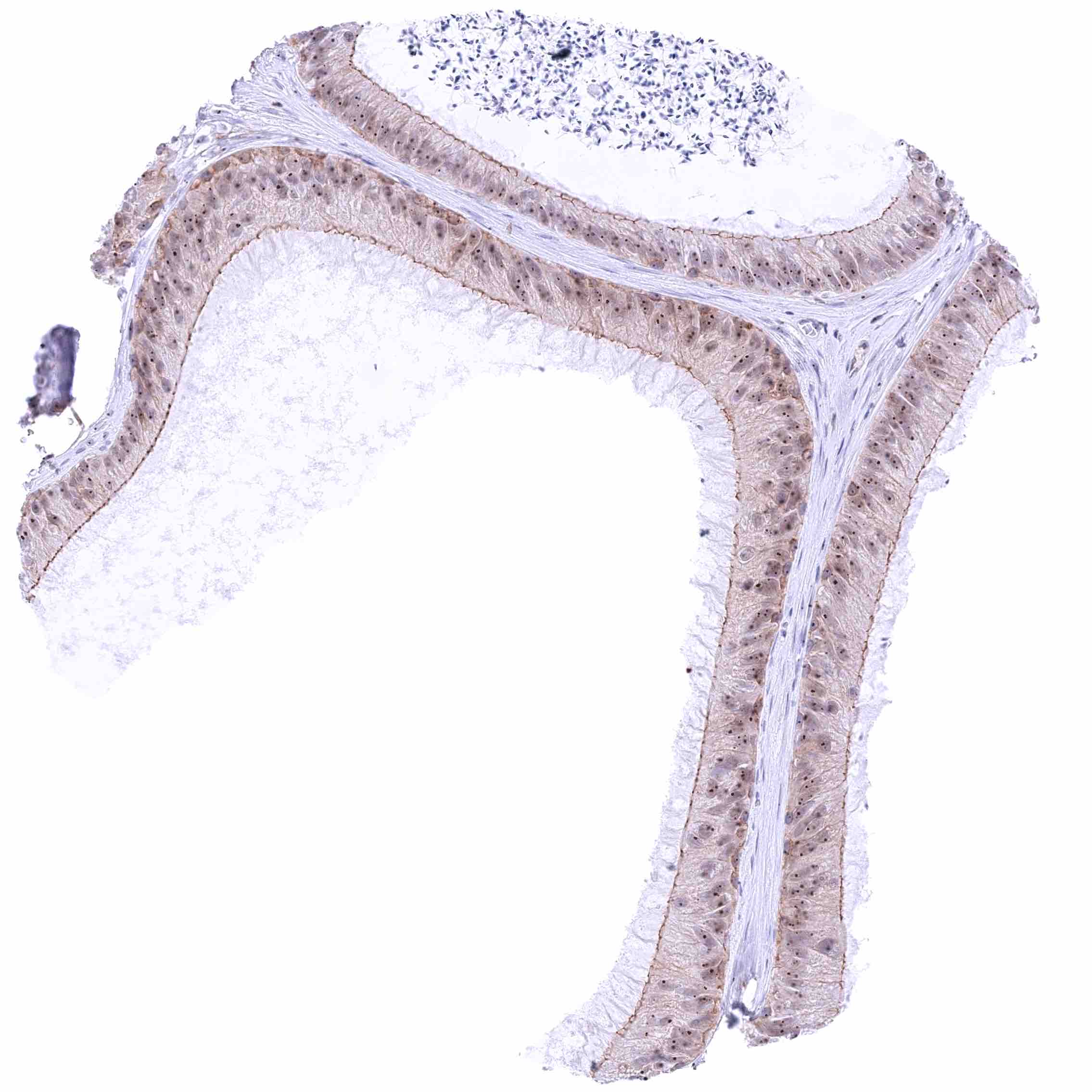
| Epididymis | Weak to moderate membranous nectin-4 staining of apical and sometimes also lateral membranes of tall columnar cells and of membranes of basal cells. | |
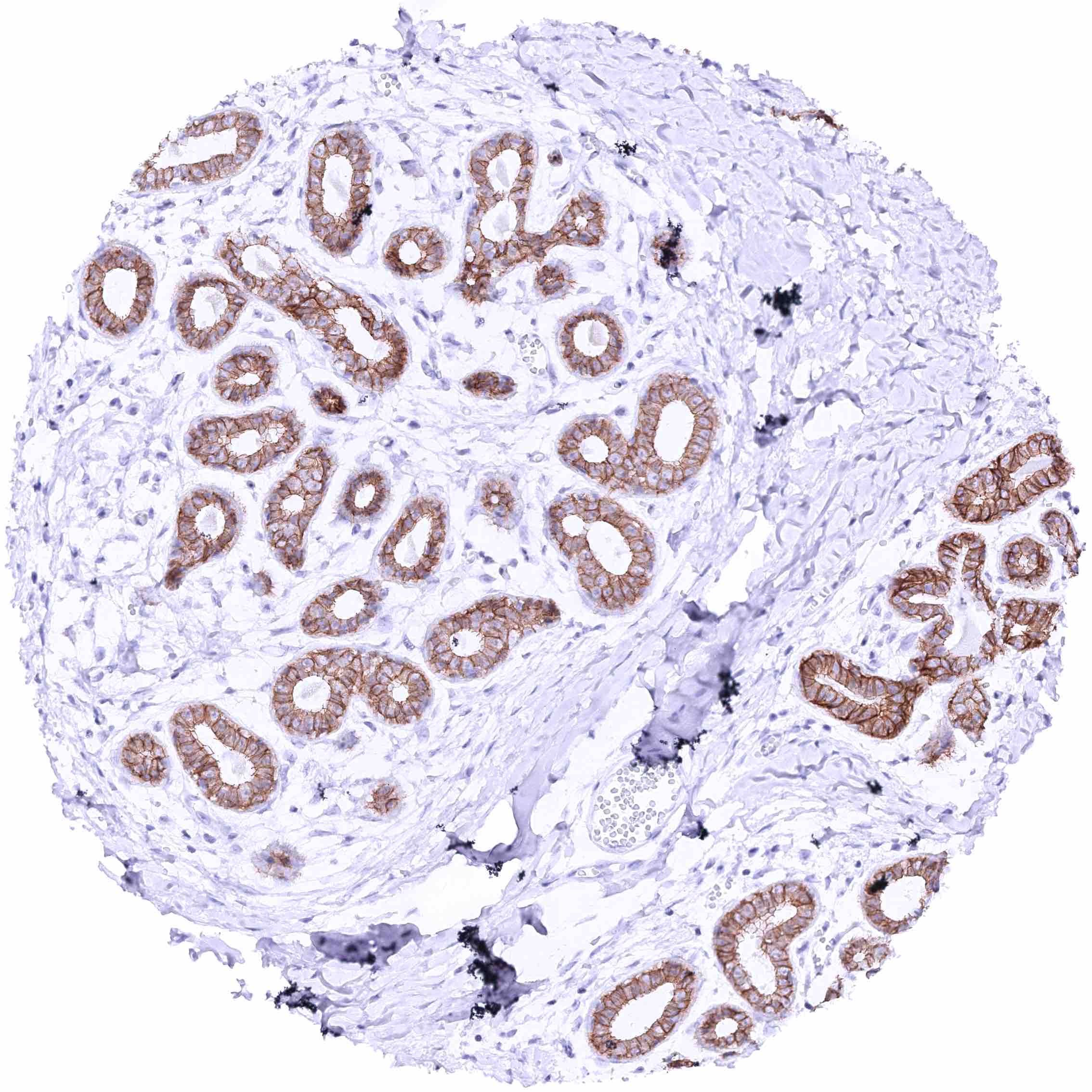
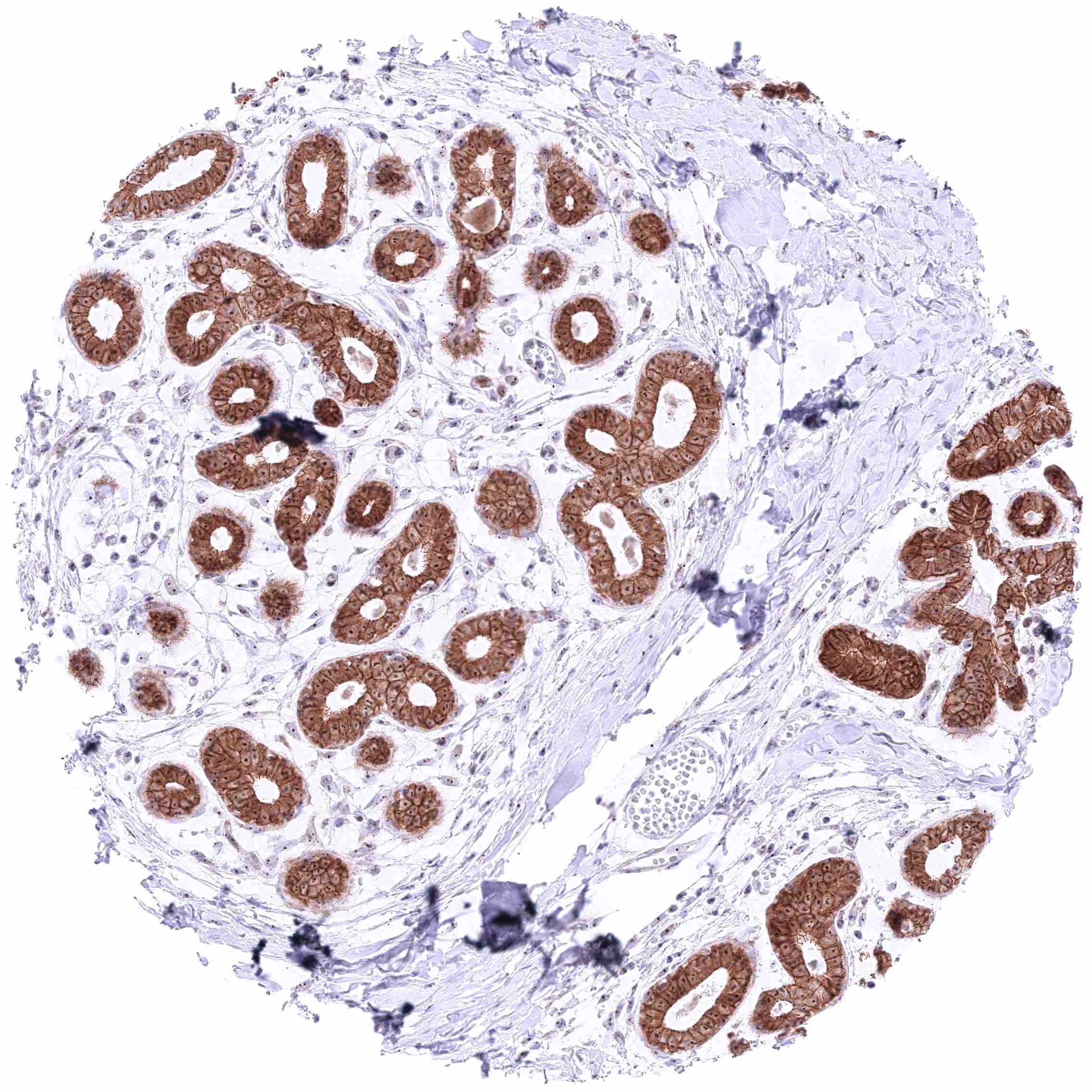
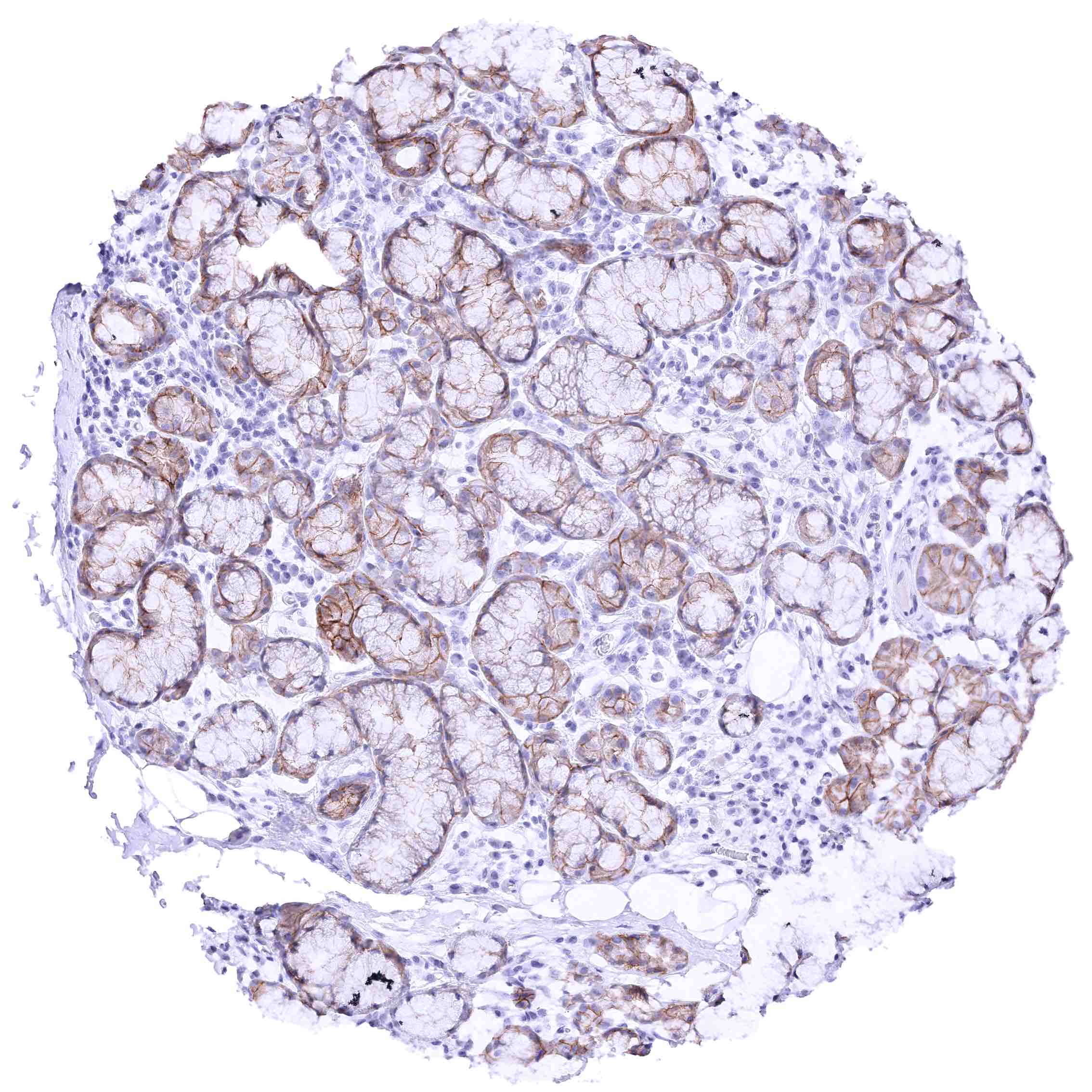
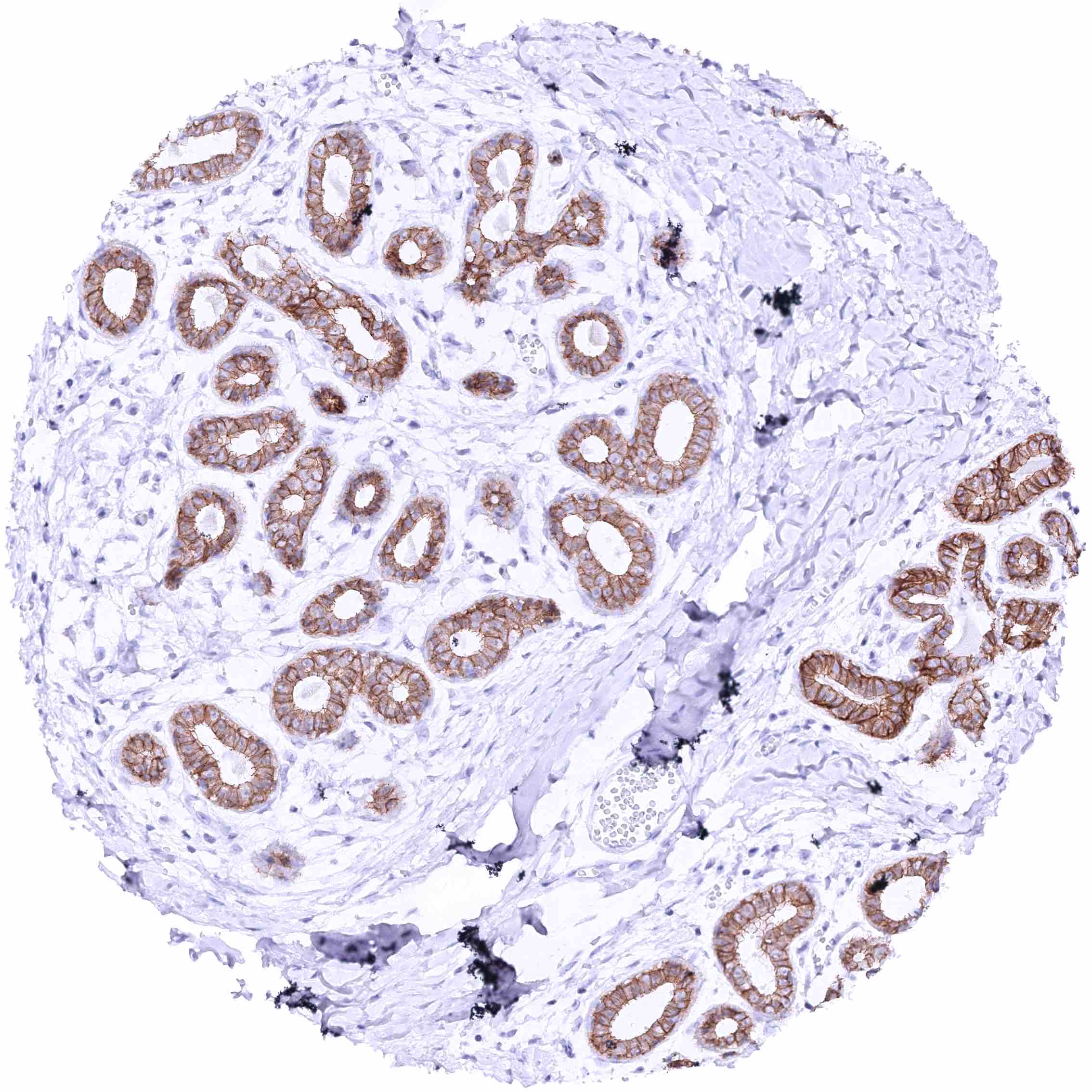
| Female genital | Breast | Strong membranous nectin-4 staining of luminal epithelial cells while staining is markedly less intense or absent in basal cells. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Nectin-4 staining of squamous epithelium is most intense in the suprabasal cell layers while the staining intensity decreases gradually towards the superficial cell layers. Basal cells are nectin-4 negative. | |
| Uterus endocervix | Distinct membranous, baso-lateral nectin-4 staining of endocervical glands. | |
| Uterus, endometrium | Weak to moderate nectin-4 staining of apical membranes of at least a fraction of endometrial glands. Decidua cells are negative in pregnancy. | |
| Fallopian Tube | Weak to moderate membranous nectin-4 staining of a subset of epithelial cells (most prominent at the lateral membranes). | |
| Ovary | Negative. | |
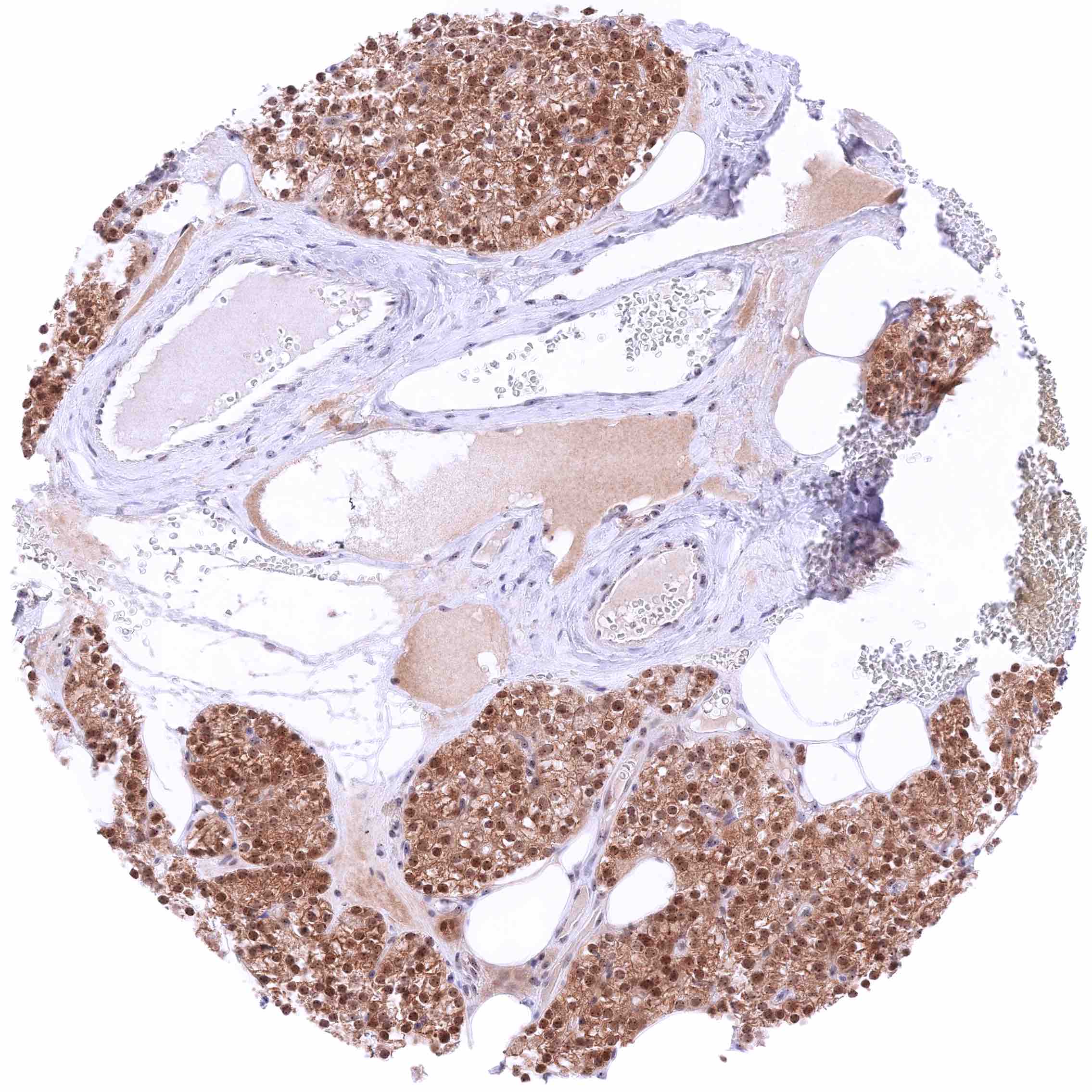
| Placenta early | Very intense nectin-4 staining of the apical surface membrane of the syncytiotrophoblast. Moderate membranous nectin-4 staining of cytotrophoblast cells. | |
| Placenta mature | Very intense nectin-4 staining of the apical surface membrane of the syncytiotrophoblast. | |
| Amnion | Moderate membranous nectin-4 staining of a subset of amnion cells, especially at the apical membranes. | |
| Chorion | Strong membranous nectin-4 staining of most chorion cells. | |
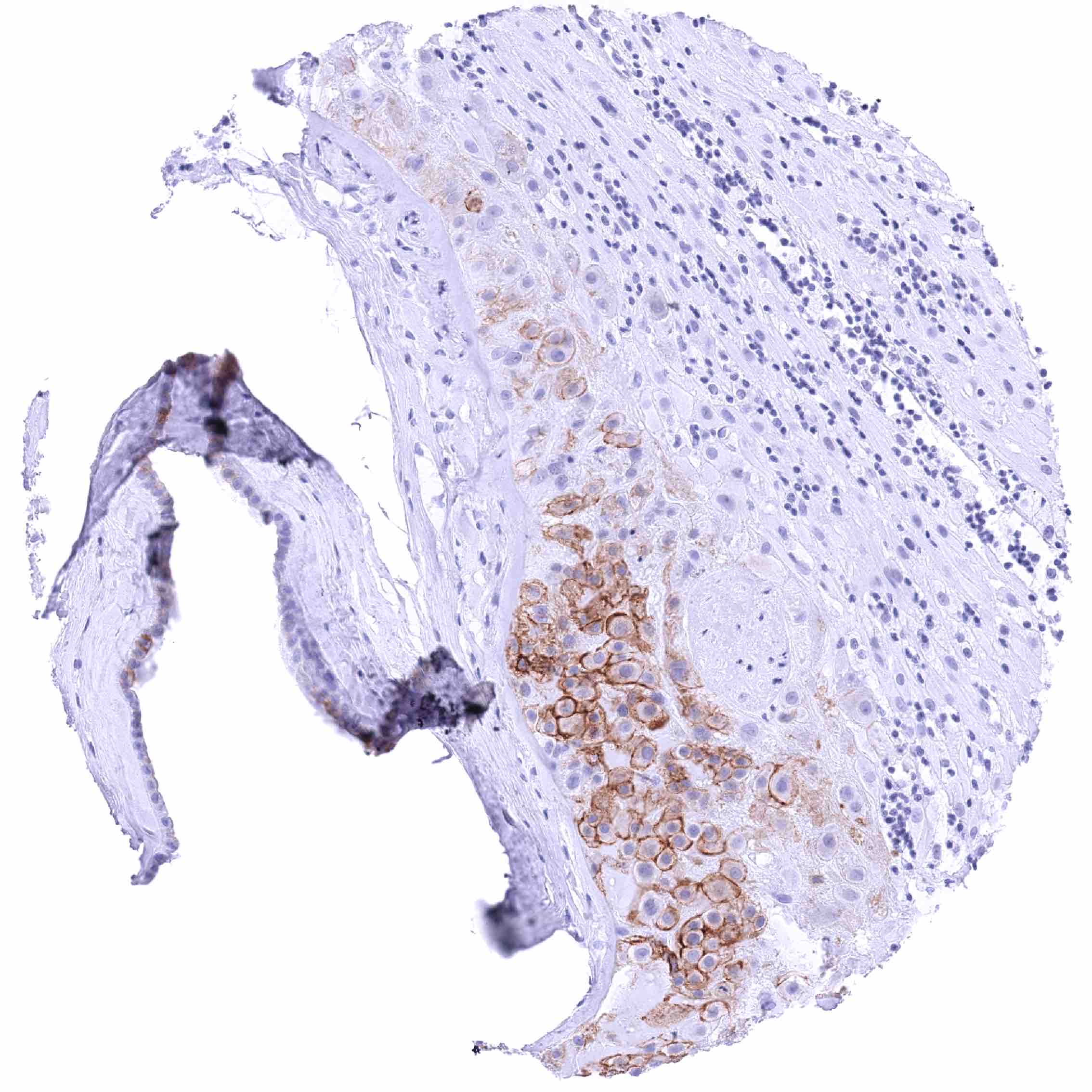
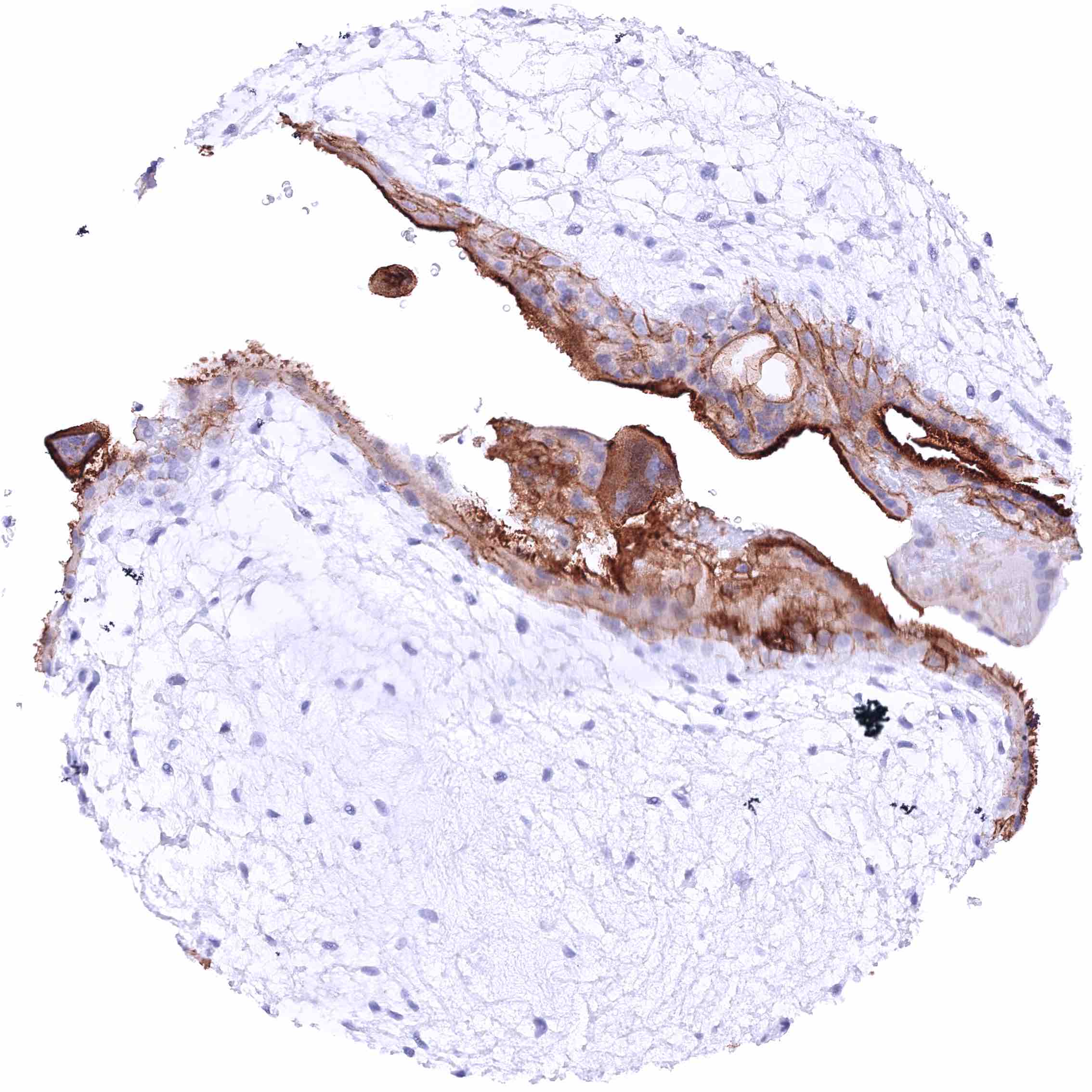
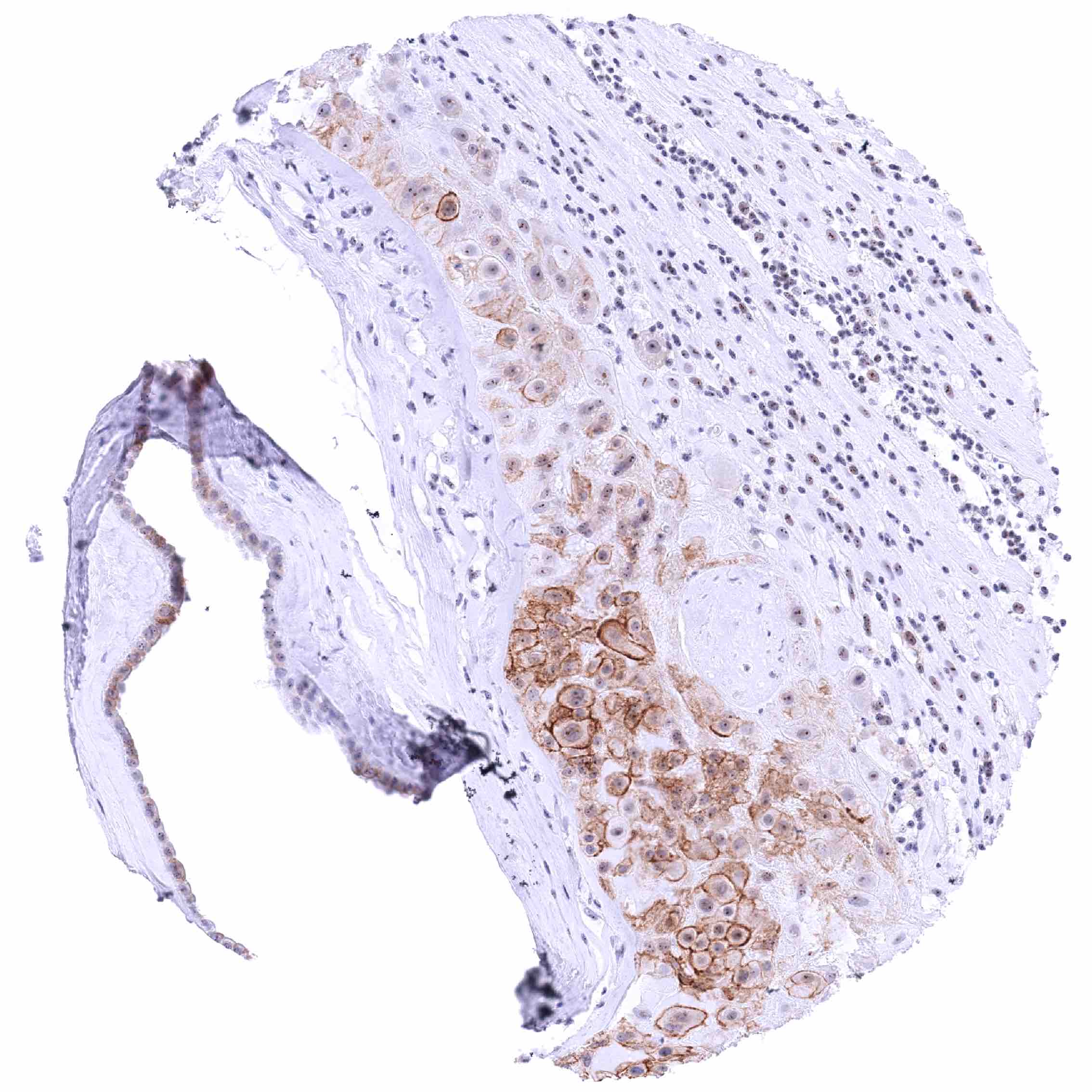
| Skin | Epidermis | In the squamous epithelium, there is a moderate to strong membranous nectin-4 staining of suprabasal and intermediate cell layers. The nectin-4 staining intensity decreases markedly towards the superficial cell layers which are often nectin-4 negative. Basal cells are nectin-4 negative. |
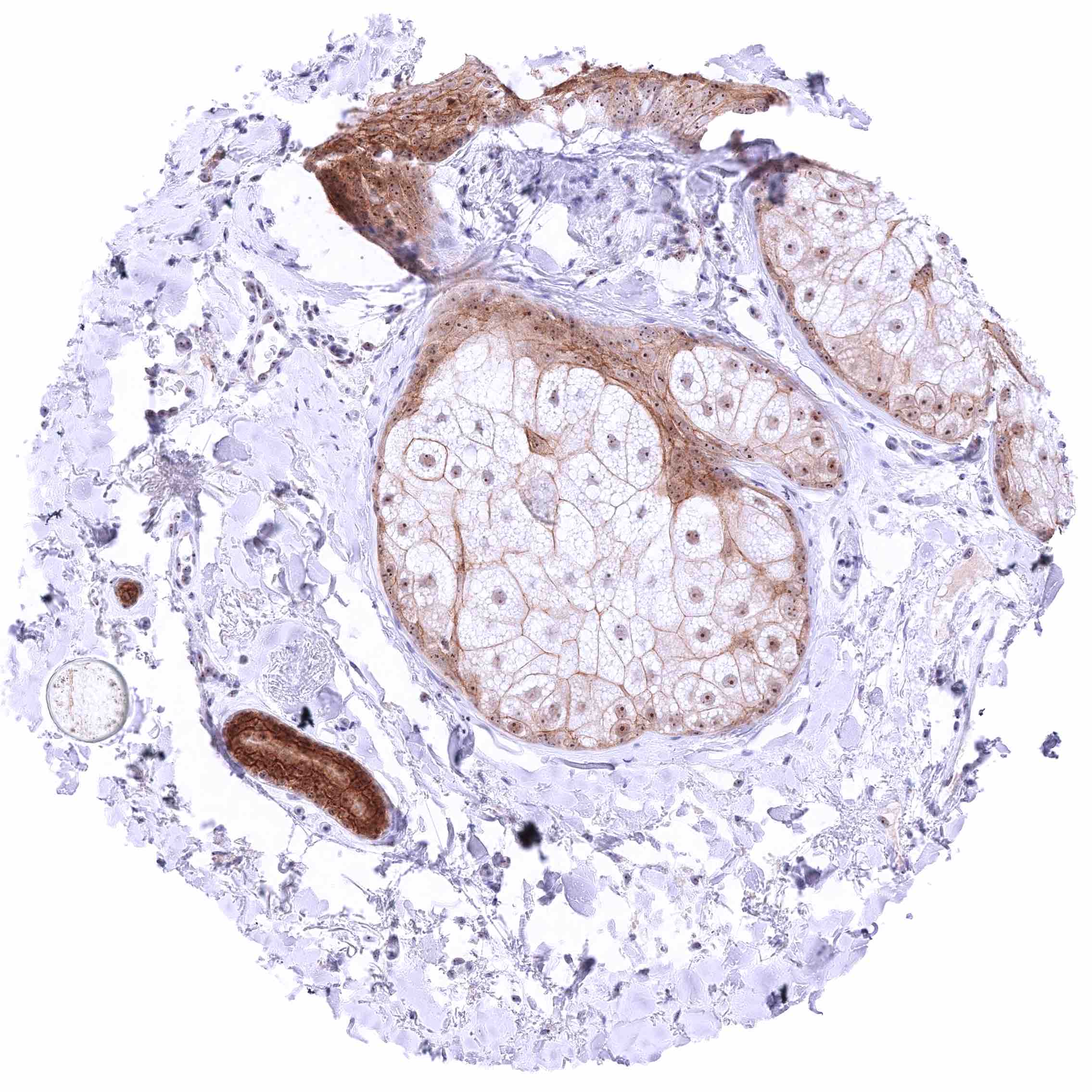
| Sebaceous glands | Weak to moderate membranous nectin-4 staining of sebaceous cells. Moderate membranous nectin-4 staining of peripheral germinative cells. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/ lymphoid tissue | Bone marrow | Negative. |
| Lymph node | Negative. | |
| Spleen | Negative. | |
| Thymus | Lymphocytes are nectin-4 negative. Most likely, a subset of cells of corpuscles of Hassall’s are nectin-4 positive (not analyzed by MSVA). | |
| Tonsil | Squamous epithelium: Strong membranous nectin-4 staining of is most intense in the suprabasal cell layers while the staining intensity decreases gradually towards the surface. Basal cells (are nectin-4 negative.
Lymphocytes: Negative. |
|
| Remarks |
These findings are largely comparable to the RNA and protein data described in the Human Protein Atlas (Tissue expression Nectin-4).
Positive control = Tonsil: A strong membranous Nectin-4 staining must be seen in squamous epithelial cells while inflammatory cells must remain nectin-4 negative.
Negative control = Lymph node: All cell types must not show Nectin-4 staining.
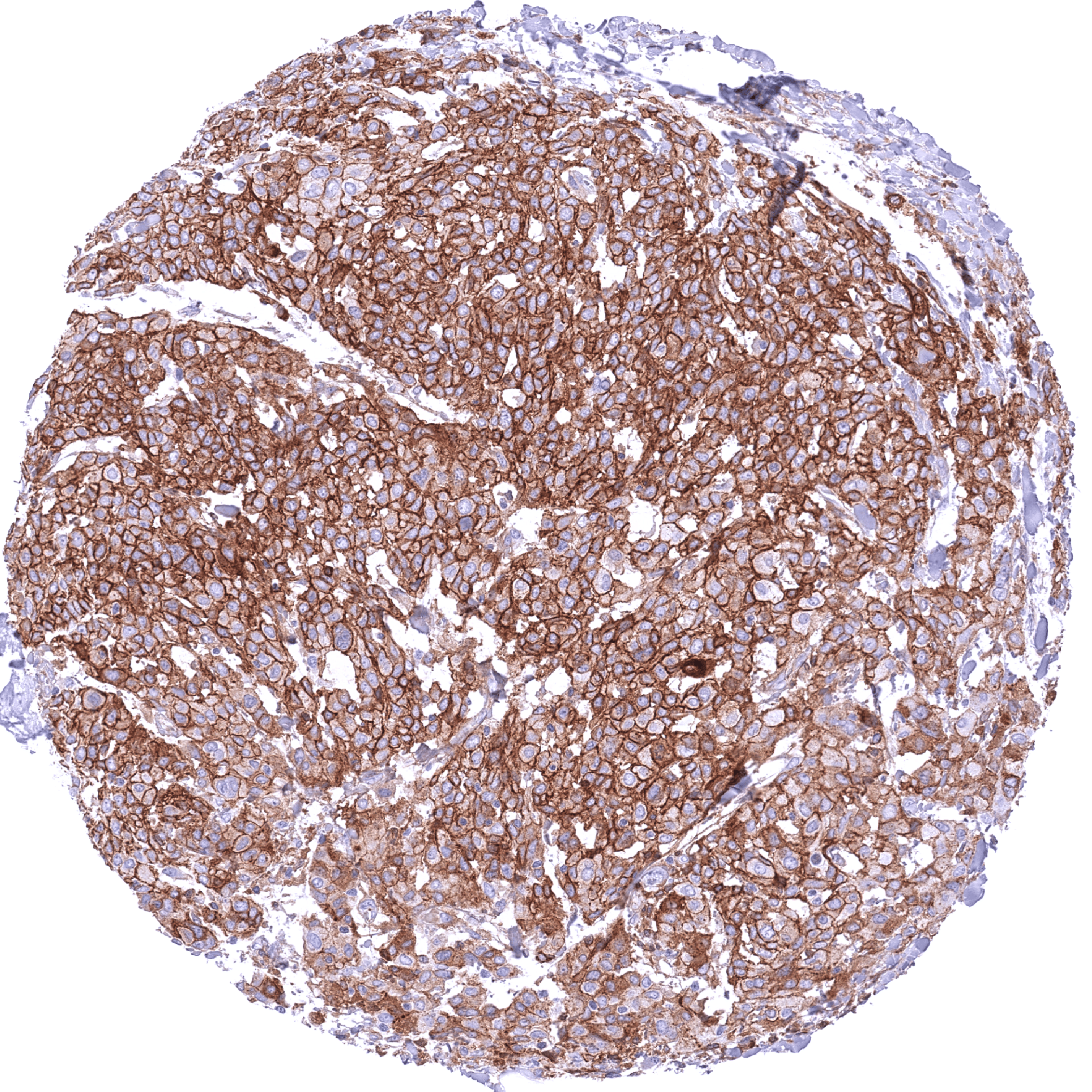
Staining Pattern in Relevant Tumor Types
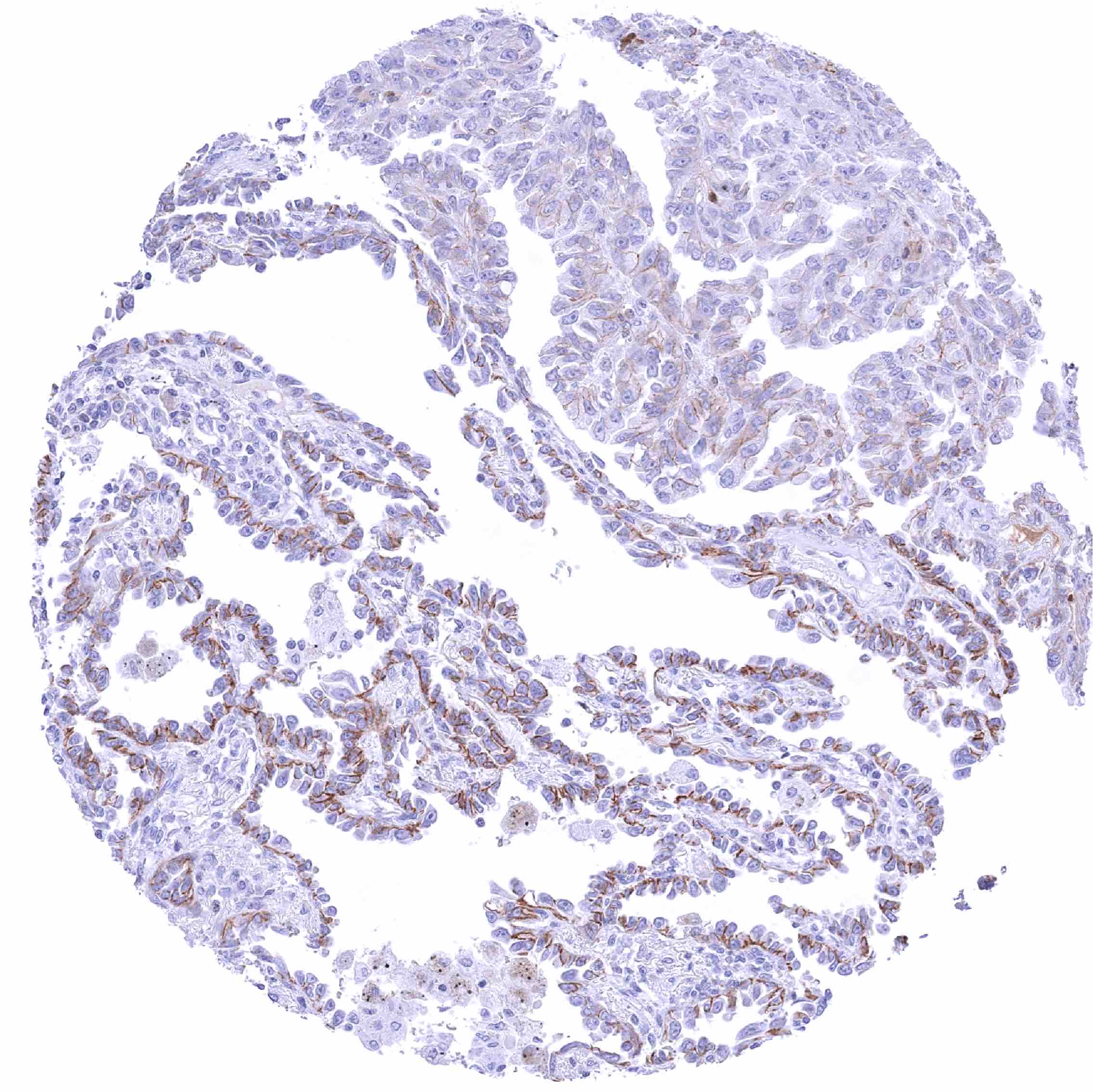
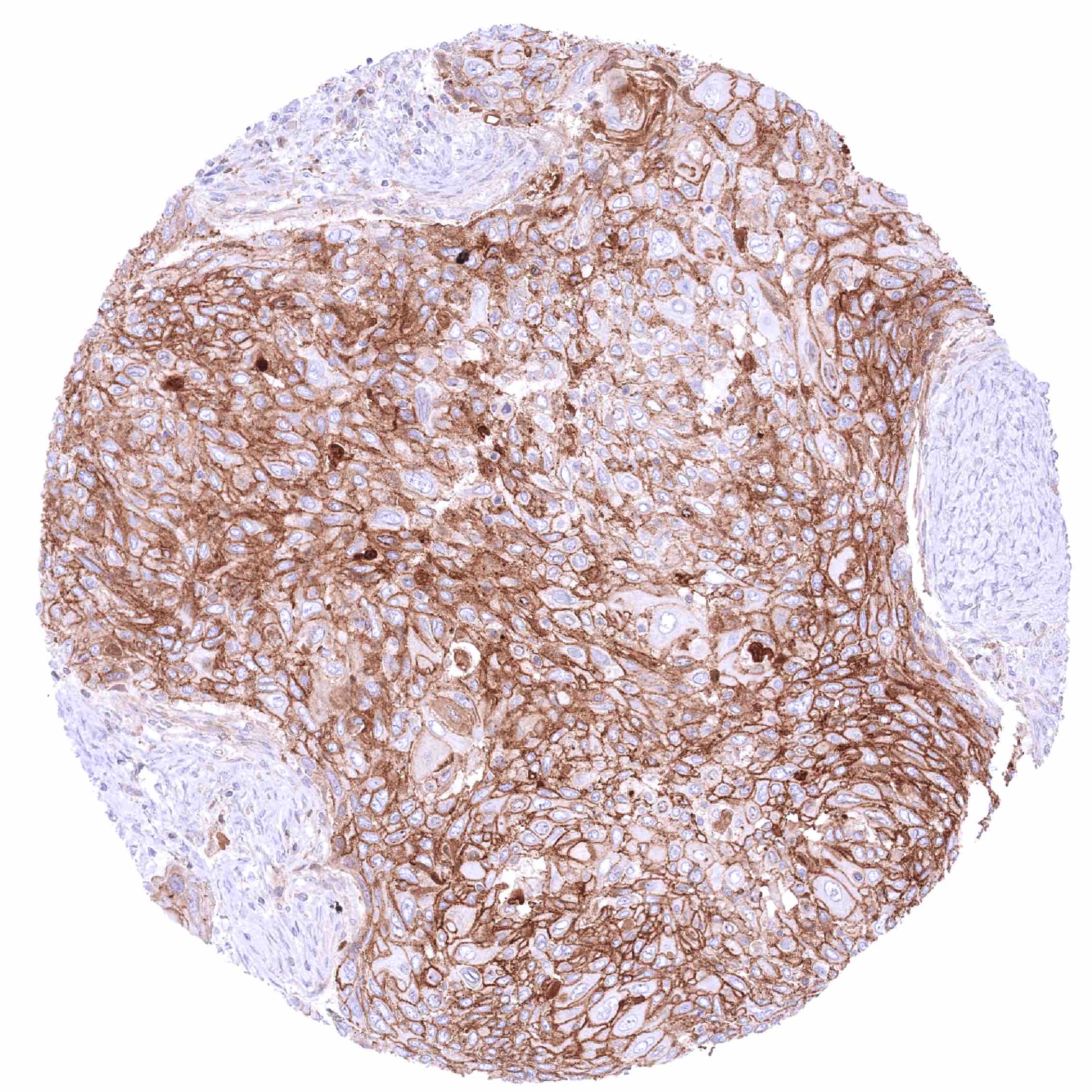
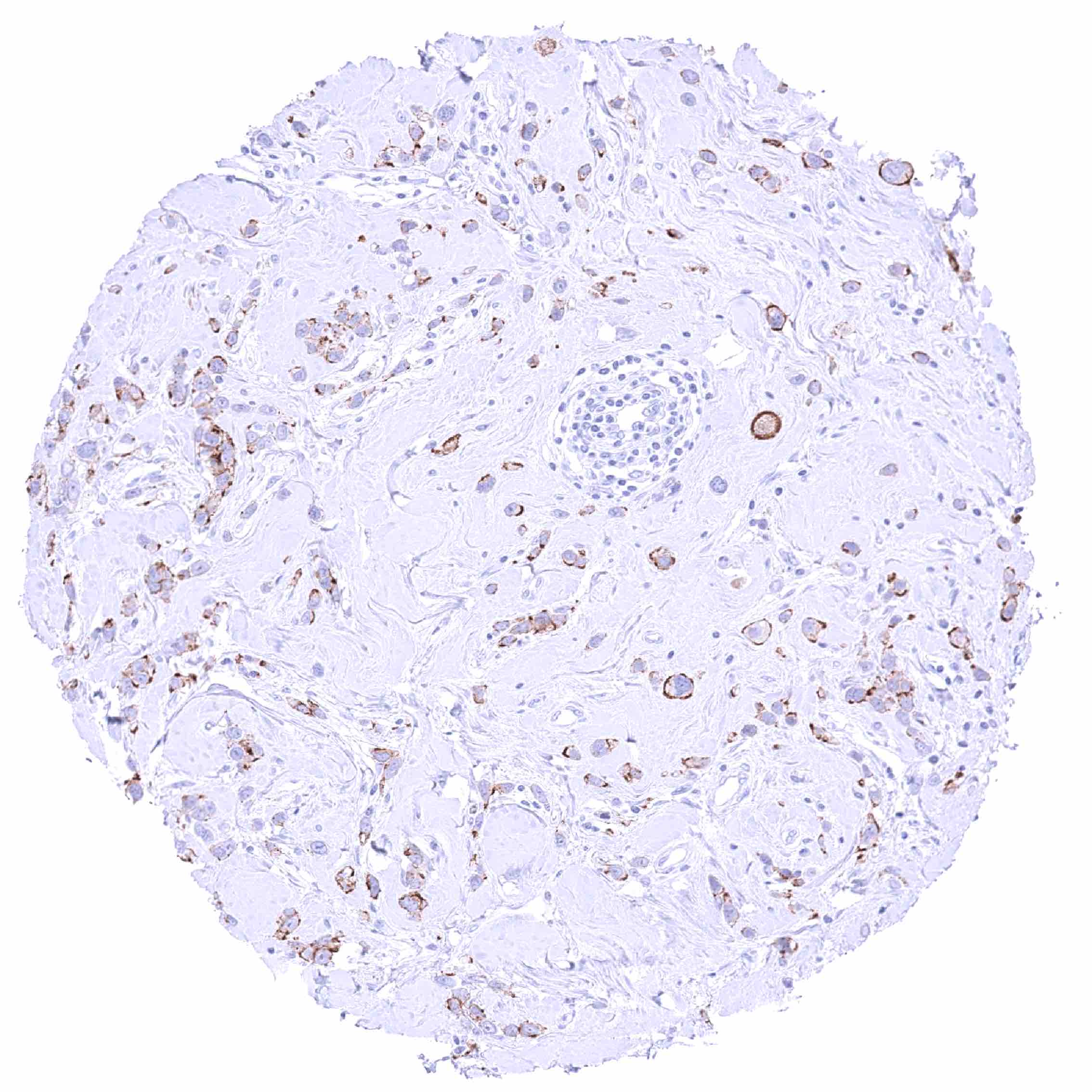
Nectin-4 expression is particularly frequent in squamous cell carcinomas from different sites of origin, urothelial tumors, pancreatic adenocarcinoma, pulmonary adenocarcinoma, and in breast cancer. However, Nectin-4 expression can also occur in various other tumor entities.
The TCGA findings on Nectin-4 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-304M at a dilution of 1:100 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- How can Nectin-4 immunohistochemistry be optimally used to predict response to anti-nectin-4 drugs?
- How common is nectin-4 expression in different tumor types?
- Are nectin-4 expression levels in cancers related to patient prognosis?
- What are the precise cancer-promoting molecular mechanisms resulting from Nectin4 expression?
- What are the mechanisms regulating Nectin4 expression and activity in tumors, and how do tumor microenvironment factors influence its function?
- Understanding mechanisms of resistance towards anti-nectin-4 drugs?
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody MSVA-304M a high specificity is supported by the strong concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression Nectin-4). Nectin-4 immunostaining by using MSVA-304M was only detected in organs that also showed detectable RNA expression (placenta, tissues covered by squamous epithelium, urinary bladder, breast gland, stomach, gallbladder, pancreas, salivary glands, kidney, prostate, seminal vesicle, epididymis, respiratory epithelium, cervix uteri, endometrium, fallopian tube) while staining was never seen in these tissues for which nectin-4 RNA had not been found (brain, thyroid, parathyroid, hypophysis, adrenal gland, ovary, testis, liver, small intestine, colorectum, connective tissue, fat, muscle, bone marrow, spleen, lymph node).
Comparison of antibodies: True expression of nectin-4 in all cell types found to be positive by using the antibody MSVA-304M was confirmed by identical IHC staining patterns obtained by a second, independent nectin-4 antibody, termed “validation antibody”. Additional nucleolar, cytoplasmic and membranous stainings in lymphocytes, epithelial cells of the small intestine and the colorectum, collecting ducts of the kidney, testis, respiratory epithelium, endometrium, fallopian tube, adrenal gland, corpus luteum of the ovary, and the parathyroid gland were seen by the validation antibody but not by MSVA-304M. These stainings of the validation antibody were considered to represent antibody specific cross-reactivities of the validation antibody.