295,00 € – 895,00 €
Product details
Synonyms = cell proliferation-inducing protein 59; GLUL; Glutamate ammonia ligase; GS; PIG43; PIG59; Glutamate decarboxylase; glutamine synthase; Glutamine synthetase; glutamine synthetase I; Proliferation inducing protein 43; GLNA; GLNS
Antibody type = Mouse monoclonal / IgG
Clone = MSVA-750M
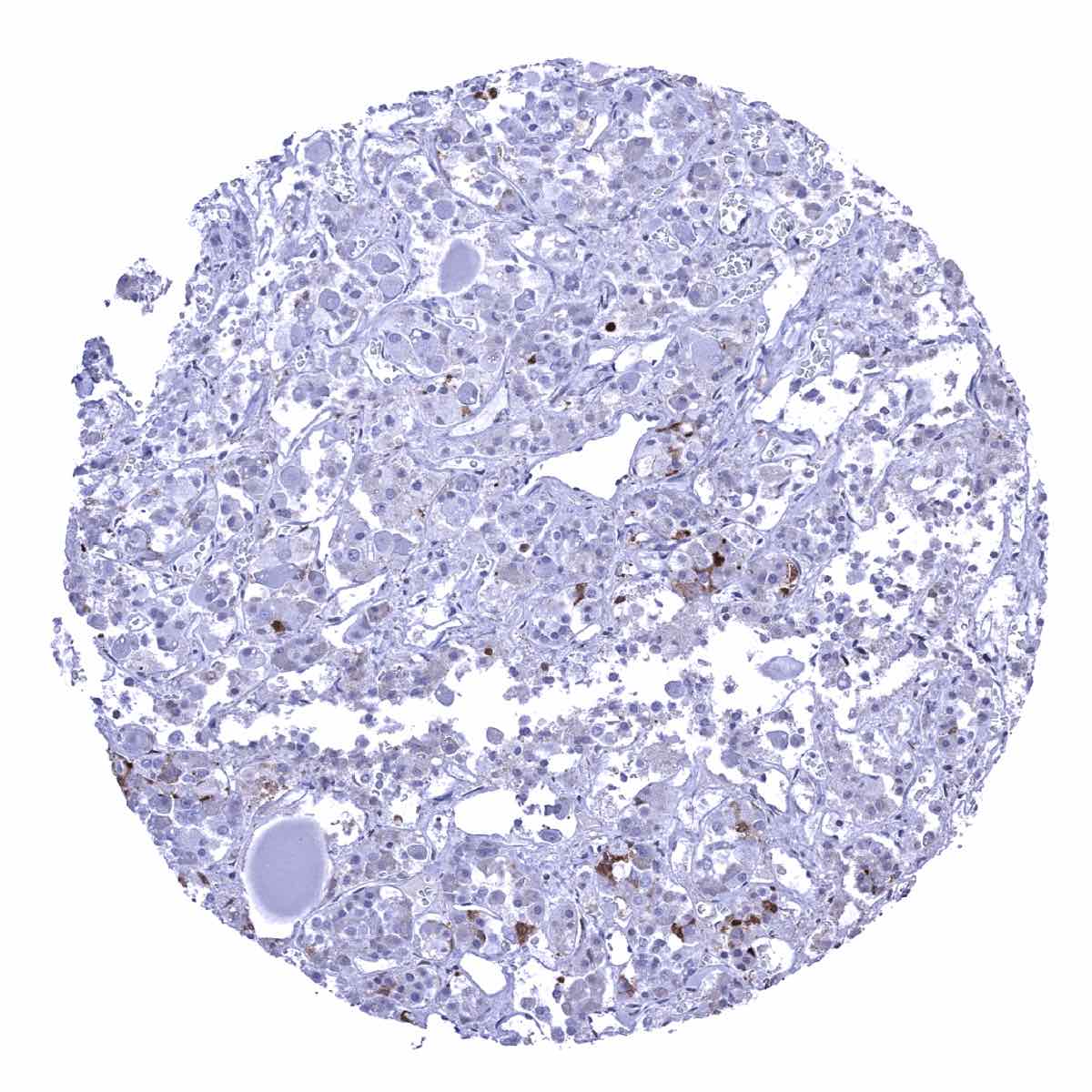
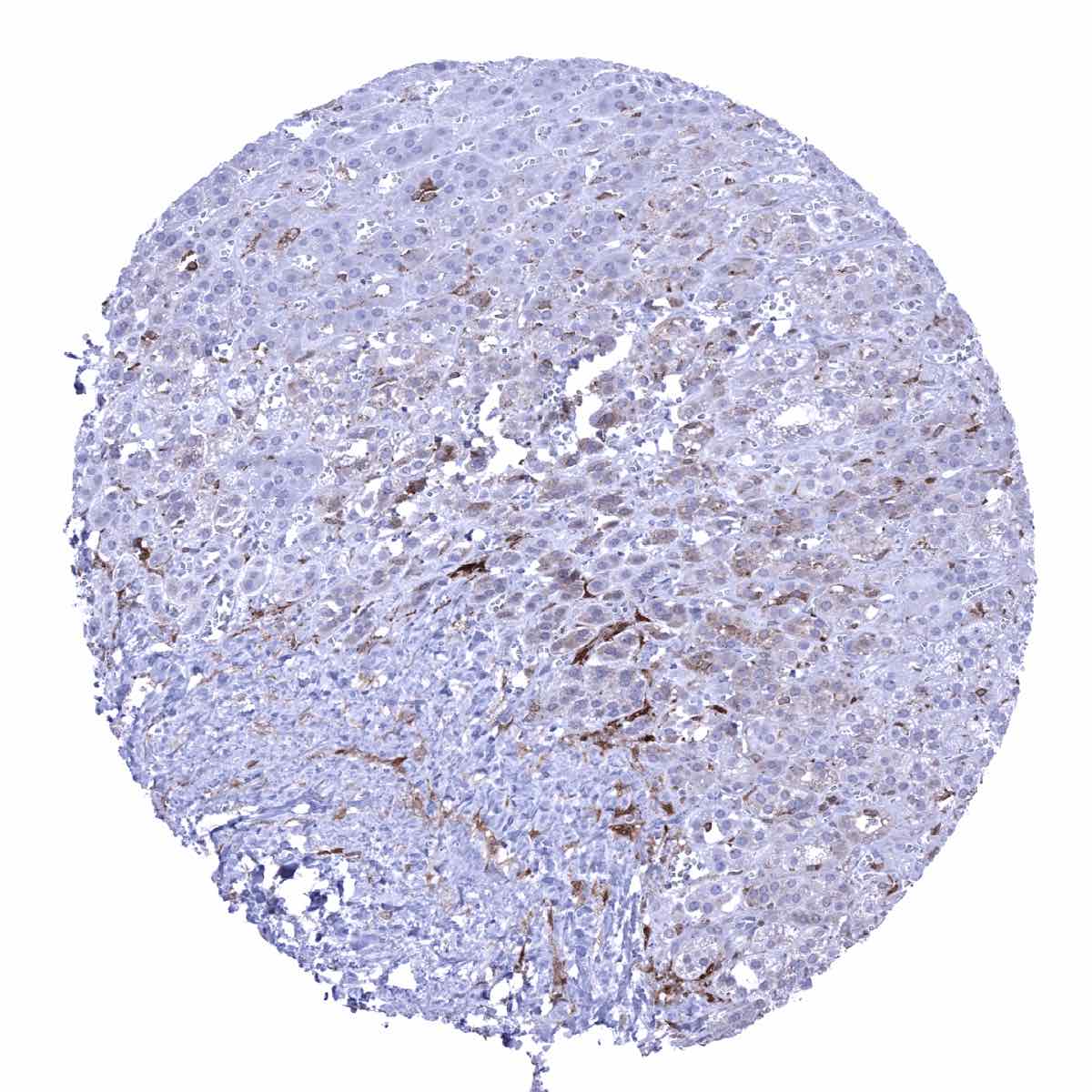
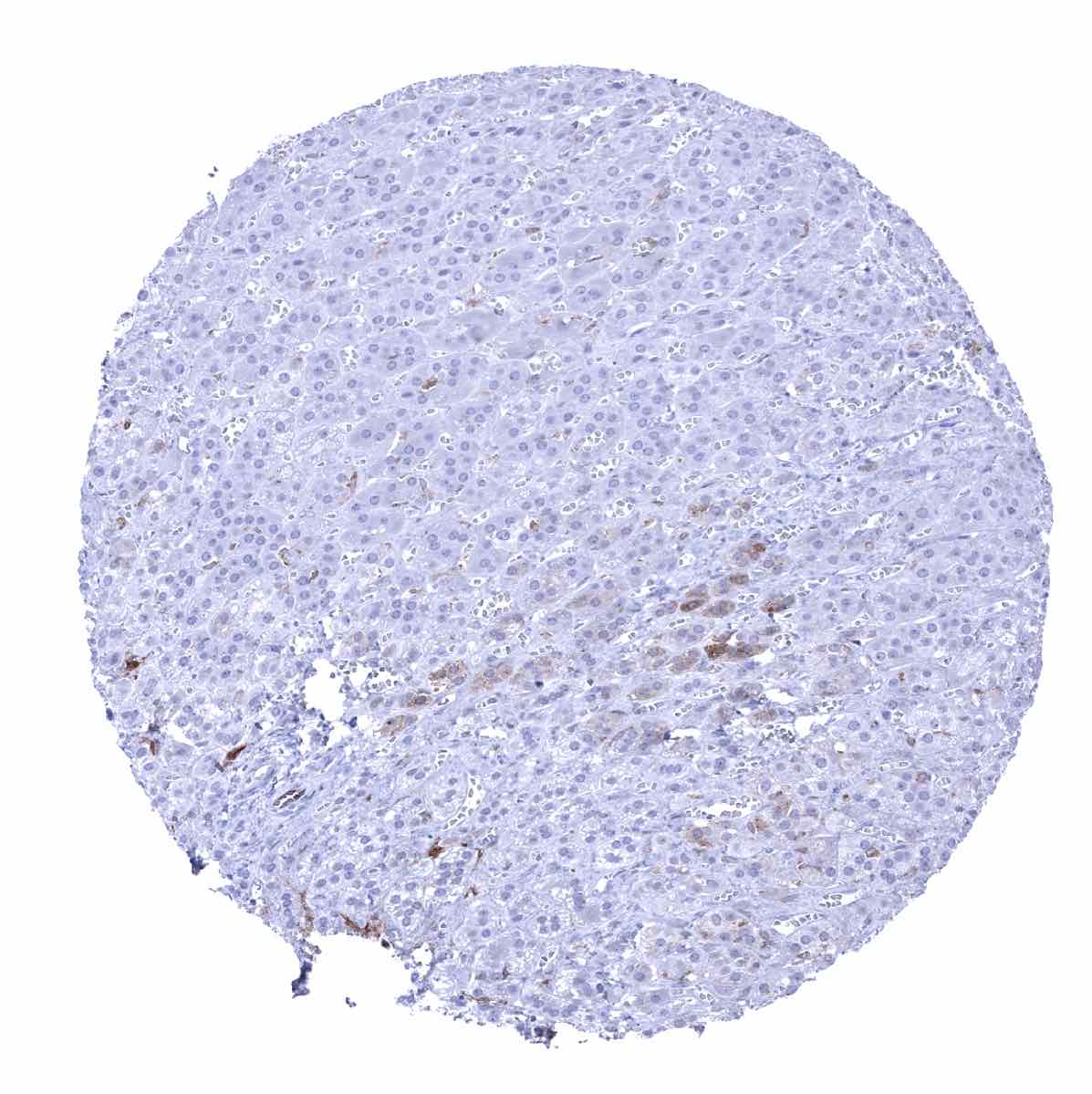
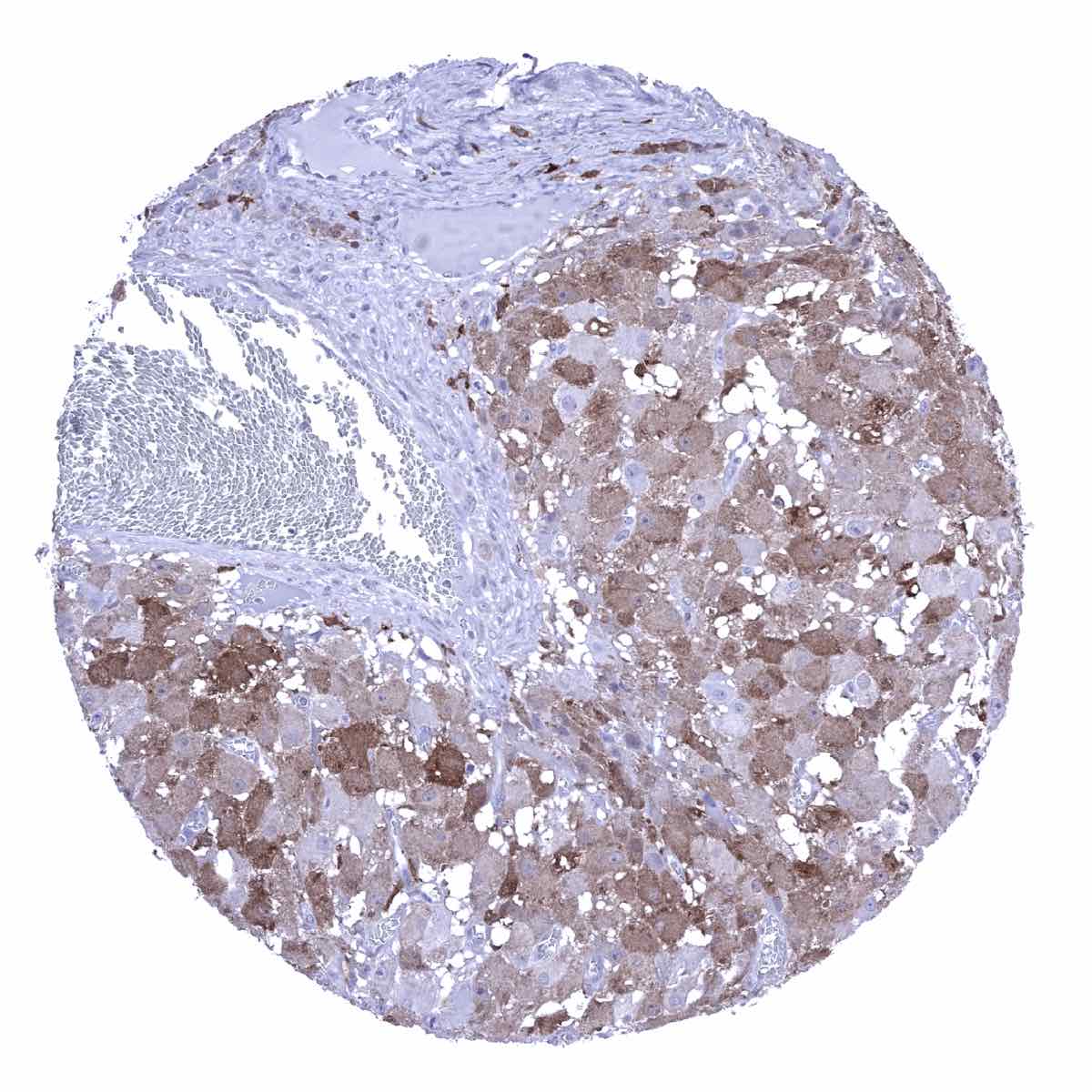
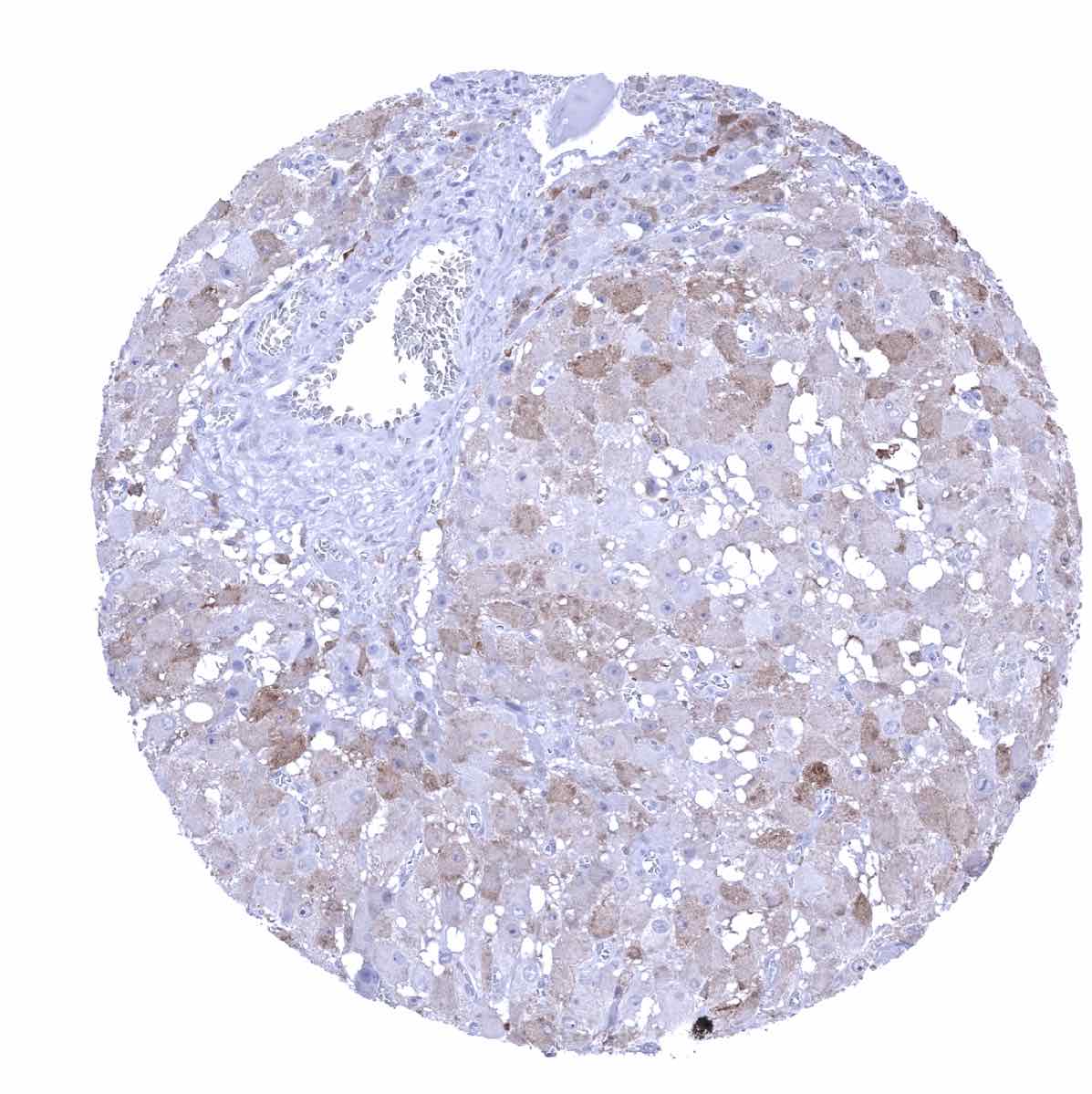
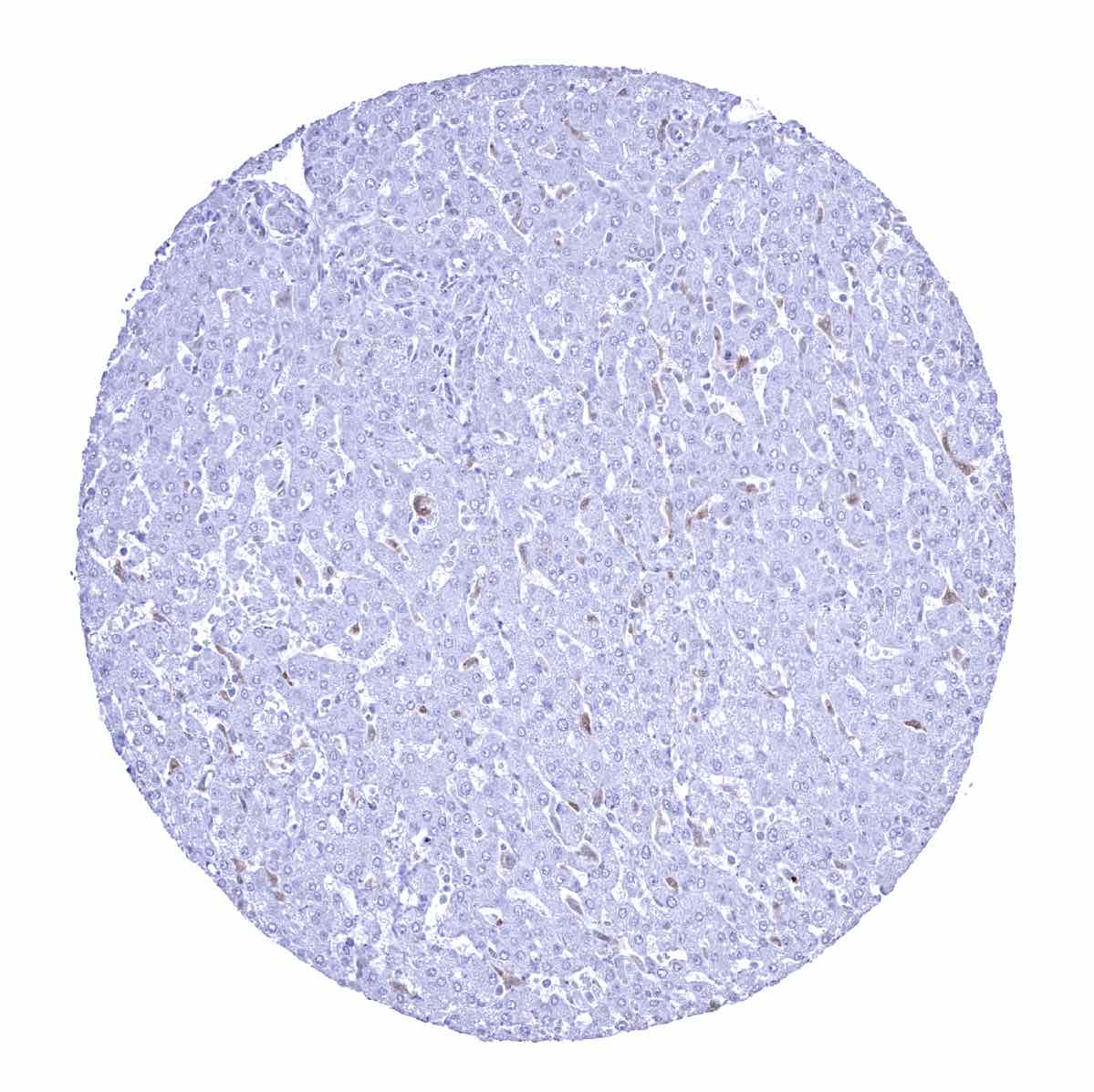
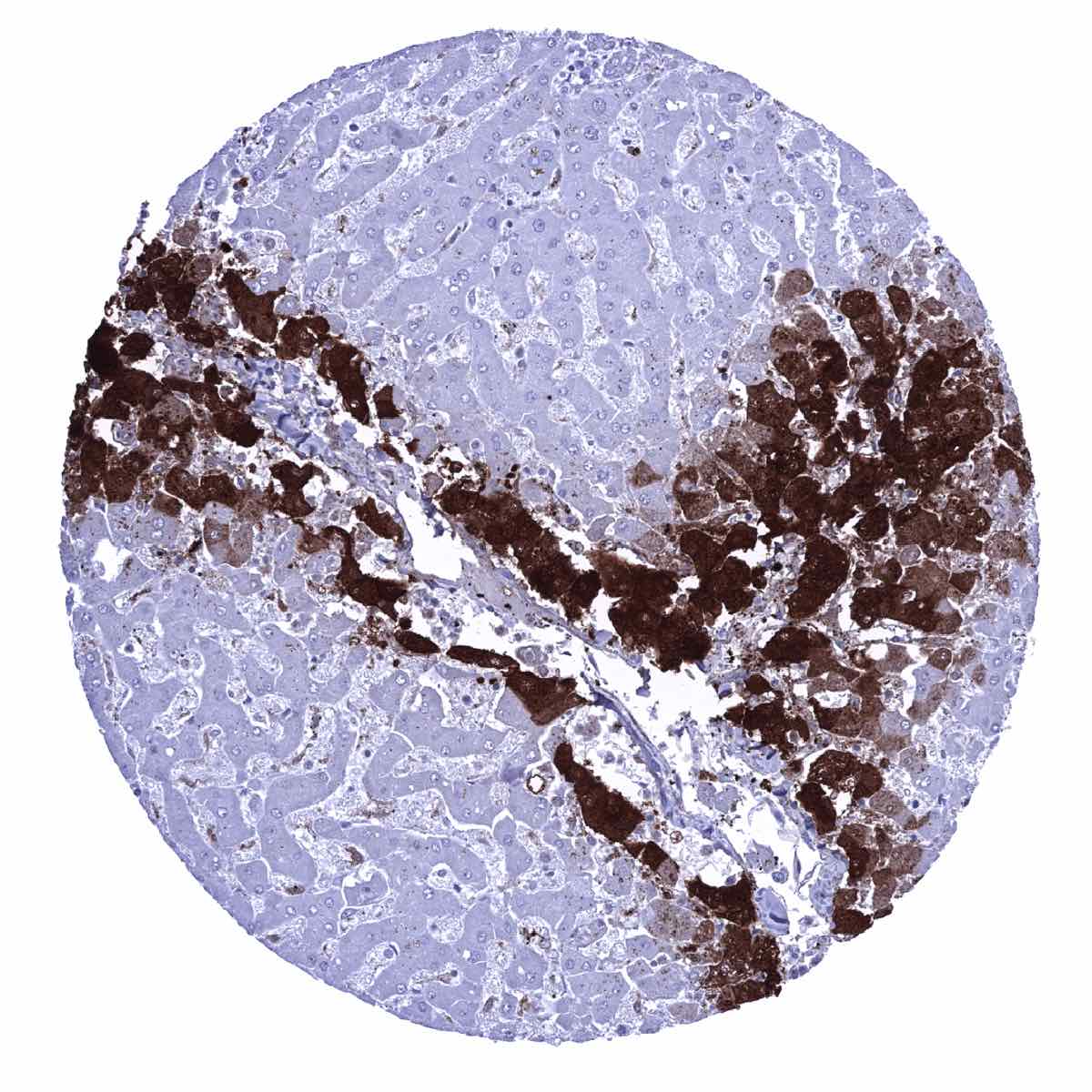
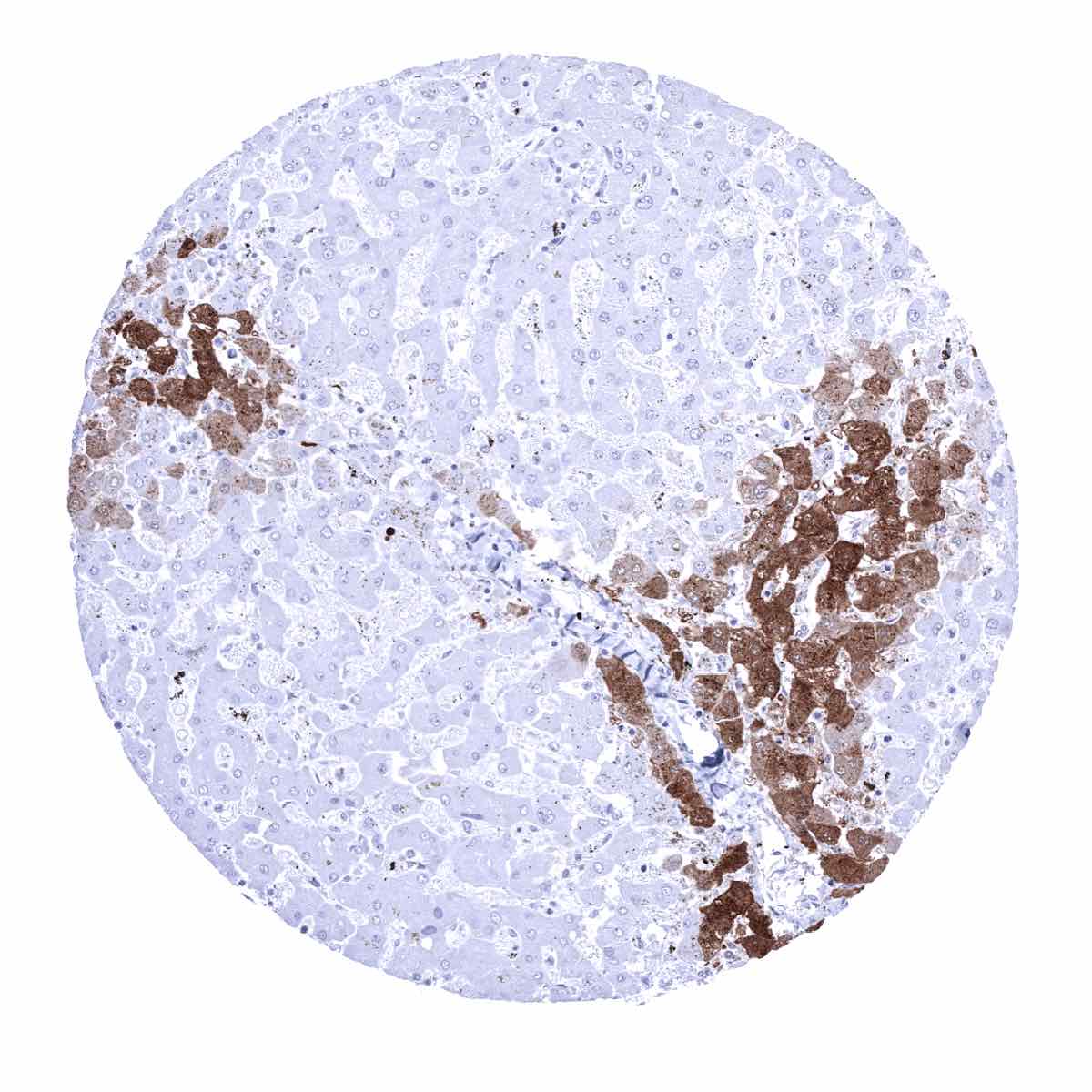
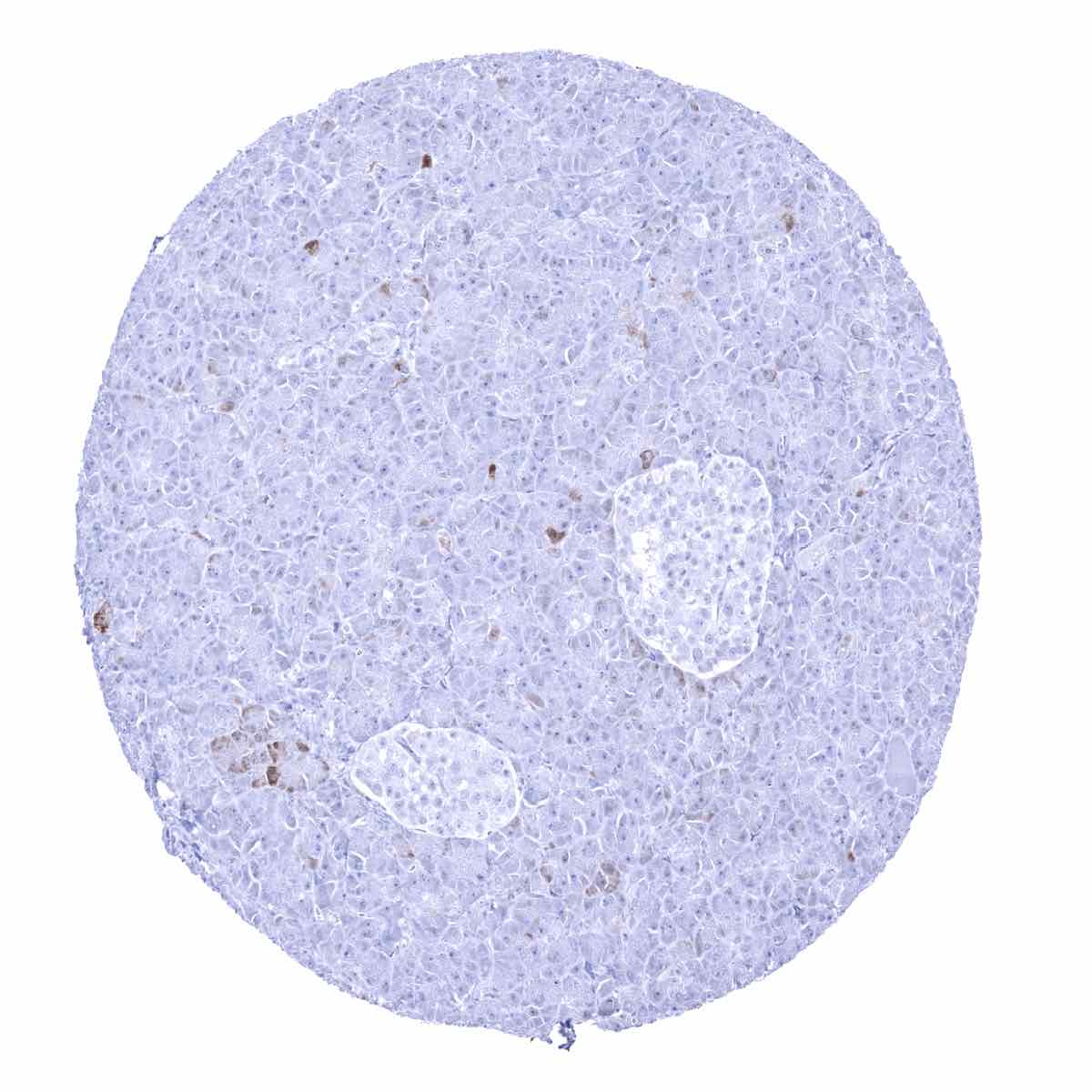
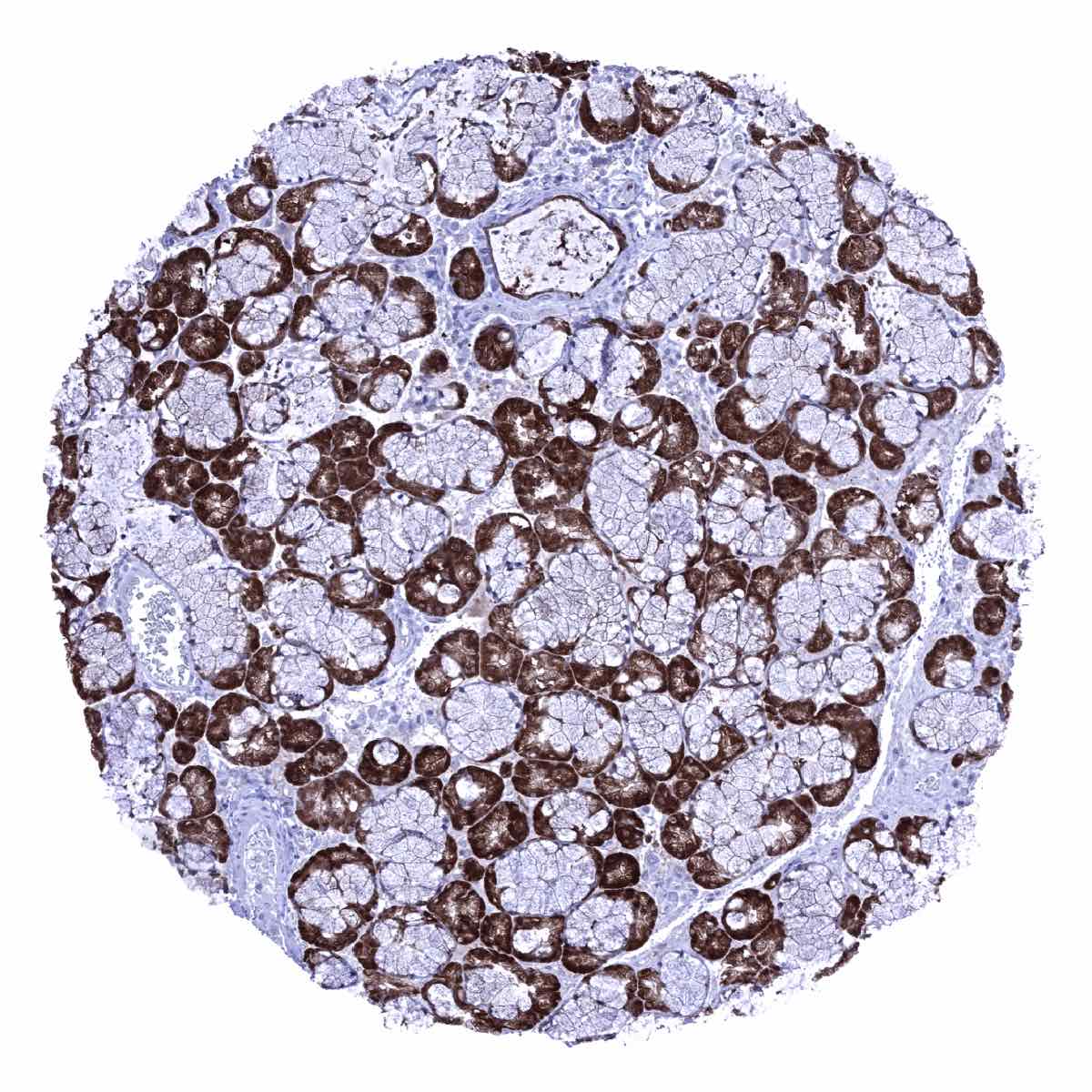
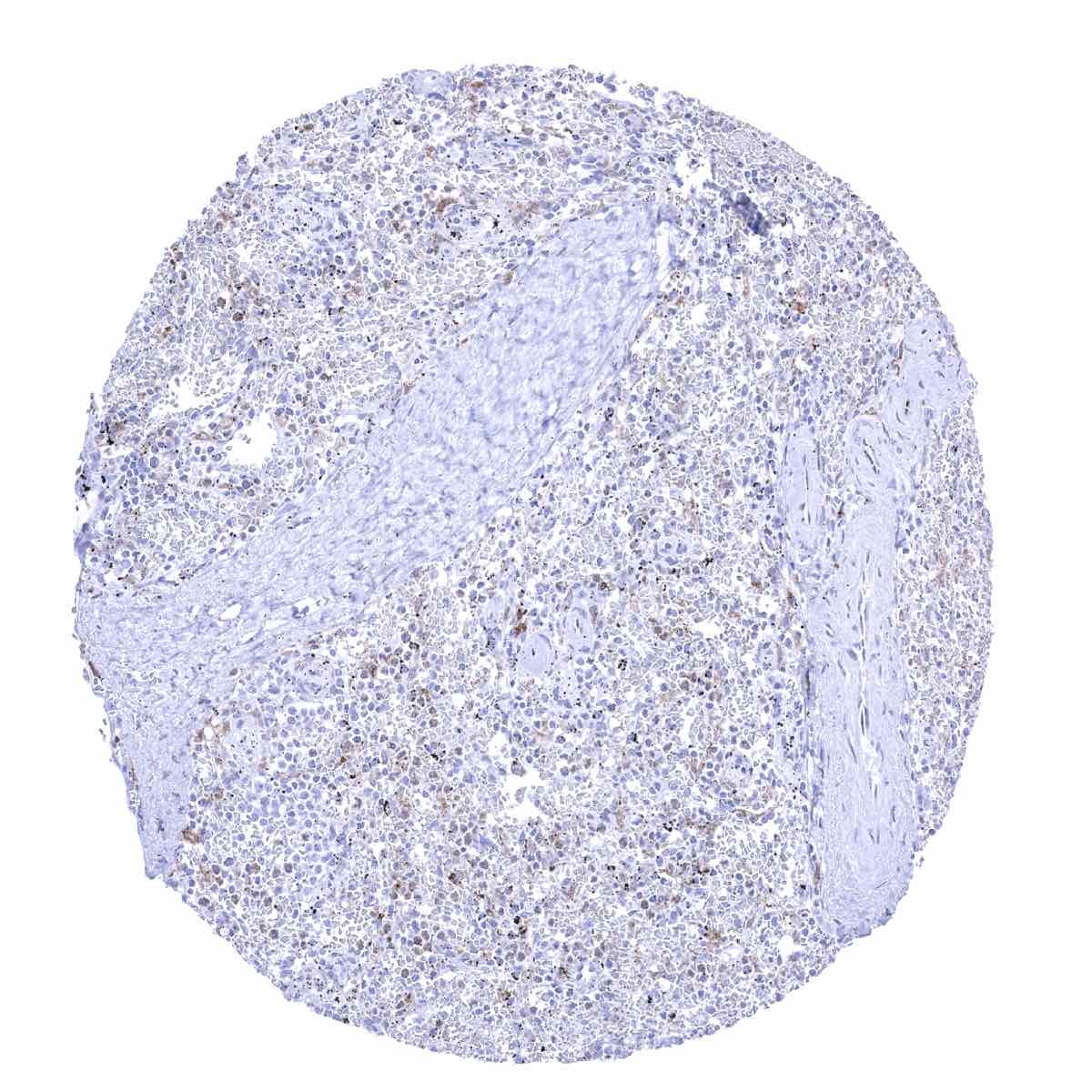
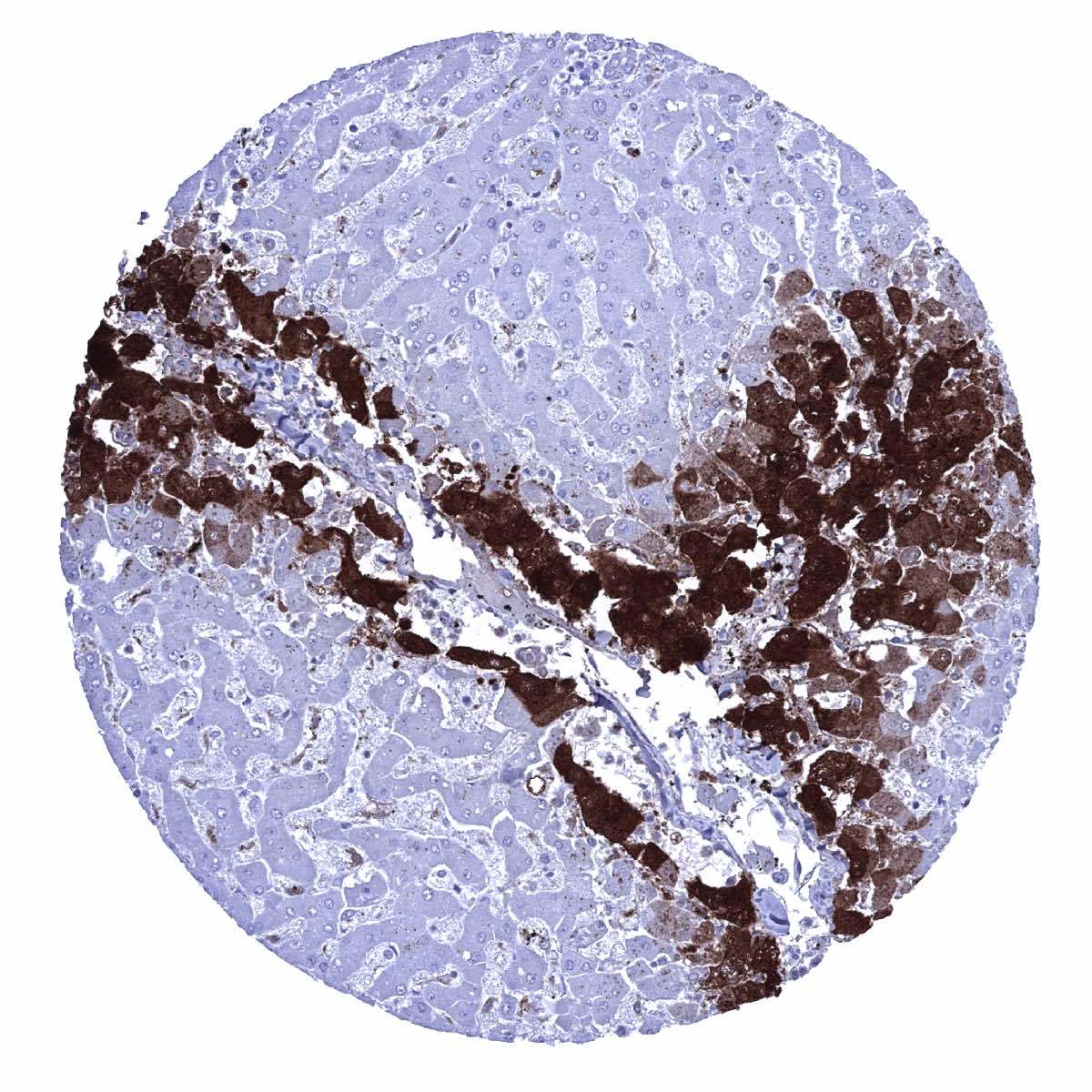
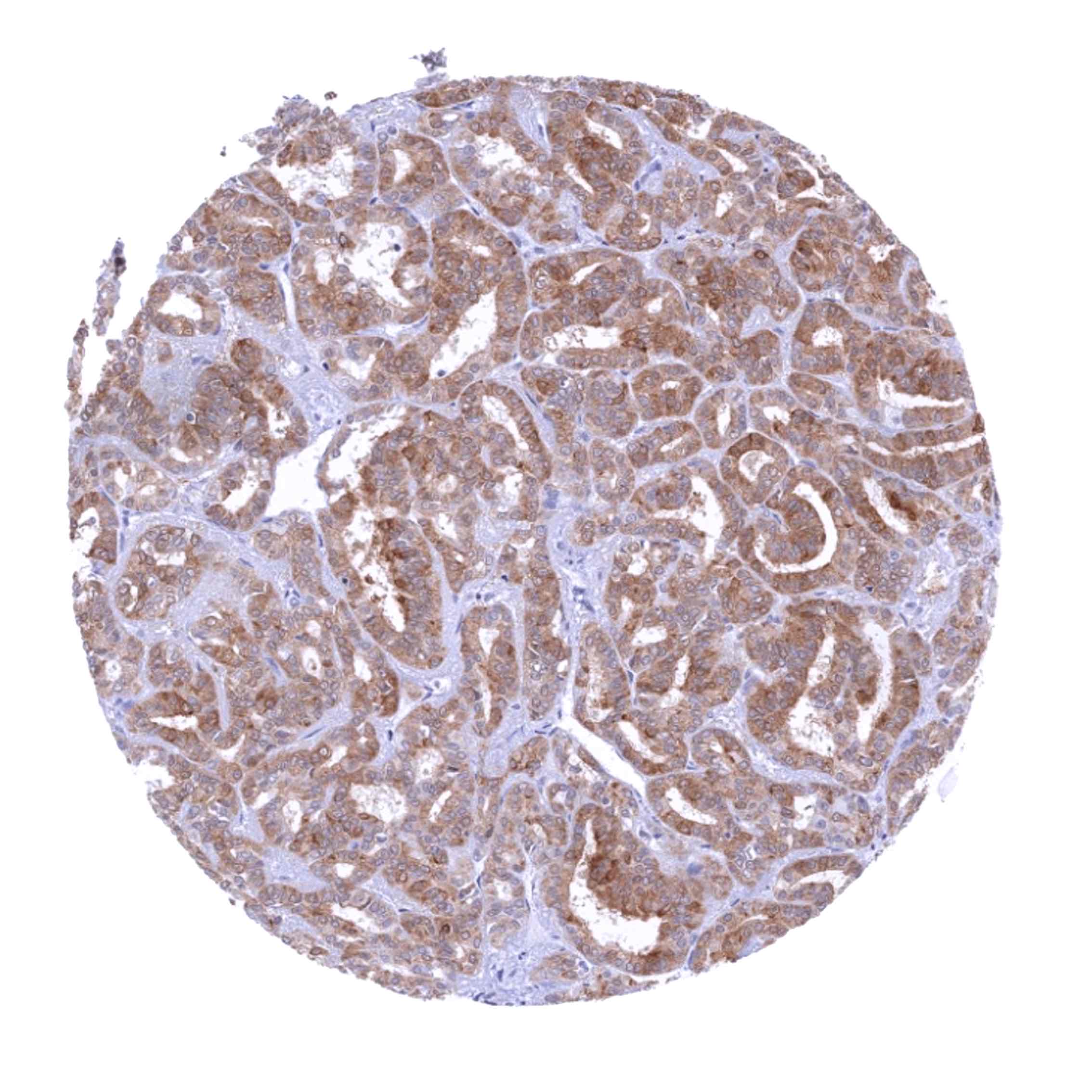
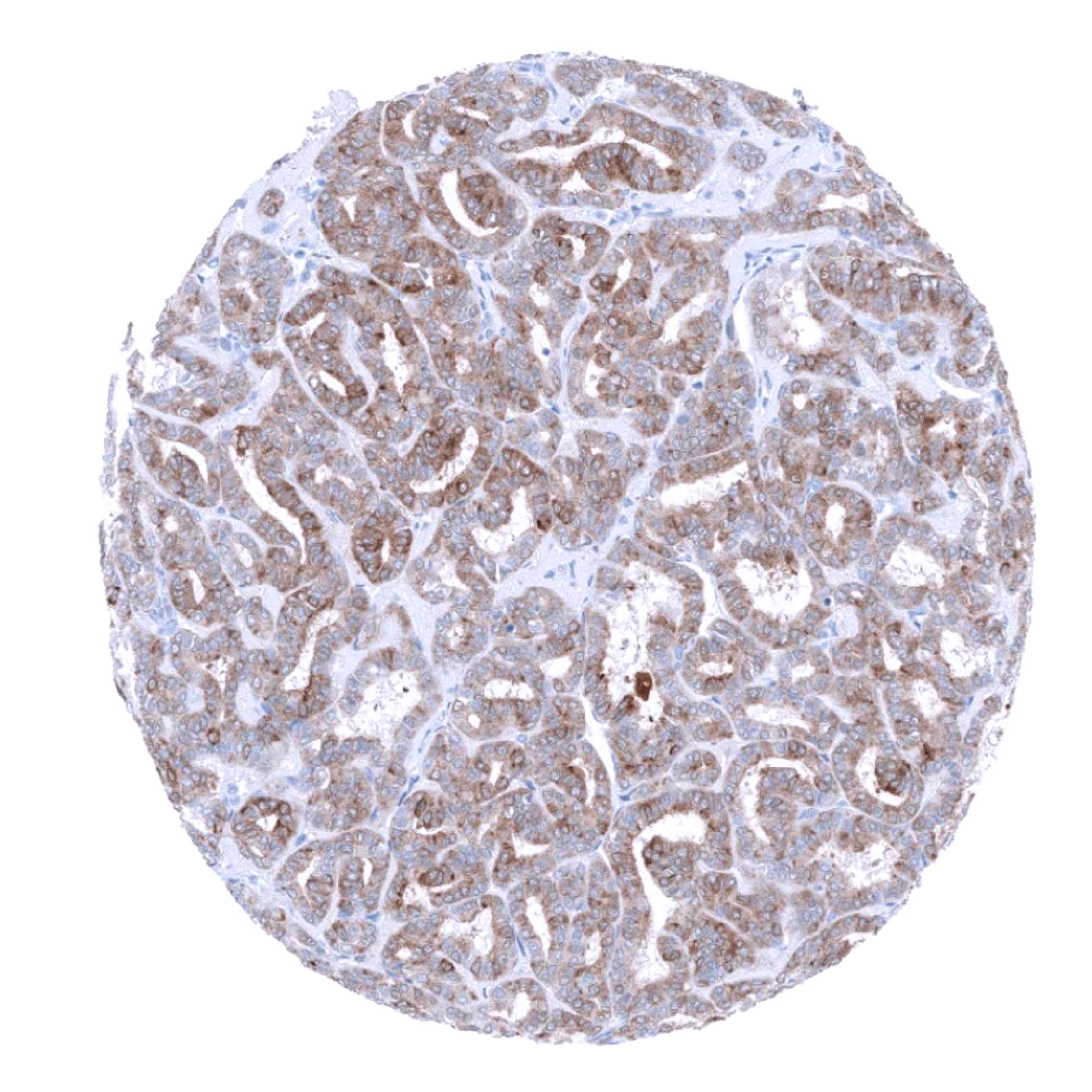
Positive control = Liver: A strong GS staining should be seen of centrilobular hepatocytes while staining is weak to moderate in Kupffer cells.
Negative control = Liver: Periportal hepatocytes must be GS negative in the normal liver.
Cellular localization = Cytoplasm. Mitochondrion.
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
Glutamine Synthetase is a key enzyme of cell metabolism.
Biology Behind
Glutamine synthetase (GS) is a 42 kDa protein, coded by the GLUL gene at 1q25.3. GS converts glutamate and ammonia into glutamine using adenosine triphosphate (ATP). As GS is the only enzyme capable of producing glutamine, GS plays a pivotal role. Glutamine is the most abundant amino acid in mammalian blood, making up as much as 20% of the total amino acid content. Glutamine is essential for protein and amino acid synthesis via transamination and purine, pyrimidine, glucosamine and carbamoyl phosphate synthesis. As the glutamine coming from diet is metabolized in the intestine, most of the body’s glutamine is synthesized de novo. GS exerts critical biological functions in liver, kidney, skeletal muscle, and brain. In the liver GS detoxifies ammonium. In the kidney, it contributes to the acid–base balance by controlling ammonium availability. In the skeletal muscle, GS synthesizes glutamine which is then consumed for energy production. In the brain, astrocytic GS controls the glutamate level which is relevant for the protection of neurons from ammonium toxicity. In cancer, GS plays a pivotal role in restructuring the cell metabolism in order to enable continued proliferation and survival of malignant cells in poorly vascularized and nutrient-deprived environments. Glutamine is an important resource for cancer metabolism because it is a substrate for nicotinamide adenine dinucleotide phosphate (NADPH) and glutathione (GSH) synthesis. Studies have demonstrated various effects of altered glutamine metabolism in cancer. Glutamine anabolism supports nucleotide synthesis by providing a nitrogen source. Glutamine catabolism, the conversion of glutamine to glutamate, supports cancer cell proliferation by generating anti-oxidants and support of macromolecule biosynthesis. GS can also be upregulated in cells of the tumor microenvironment. Tumor adjacent stroma cells can supply glutamine to cancer cells when glutamine production is insufficient in cancer cells, especially in glutamine catabolism-activated cancer. Furthermore, GS controls angiogenesis by regulating the migration of endothelial cells. Given that GS in the tumor microenvironment supports cancer cell proliferation, targeting tumor microenvironment specific GS would be an attractive option for cancer treatment.
Staining Pattern in Normal Tissues
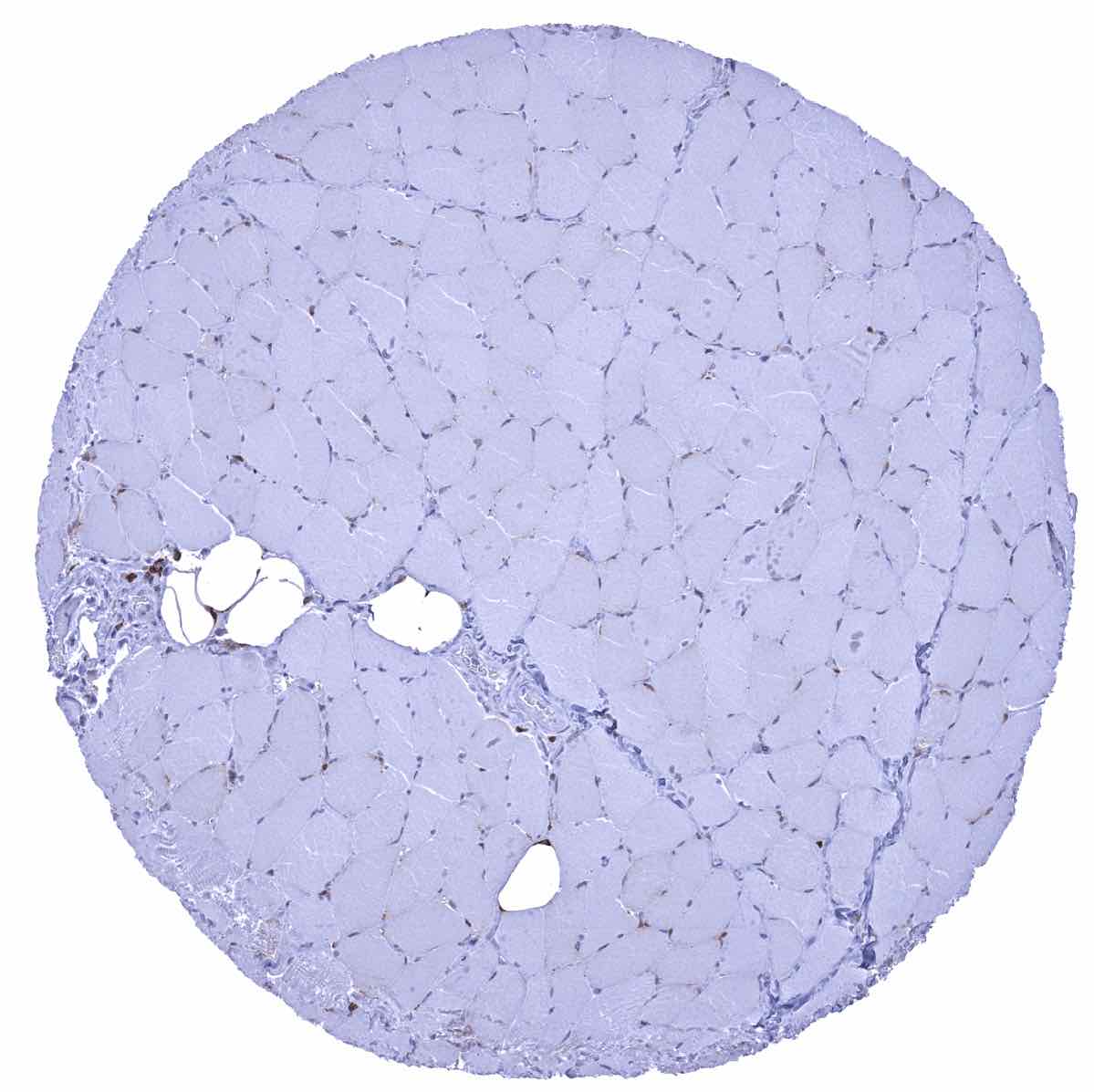
Mesenchymal tissues: A faint GS staining is seen in satellite cells of skeletal muscle. GS staining is variable in fat cells and ranges from negative to strong (dependance on function?). A weak to moderate GS staining of endothelial cells of small capillaries can be seen in various organs including myometrium, muscular wall of the colon and the urinary bladder, as well as in lymphatic and other tissues.
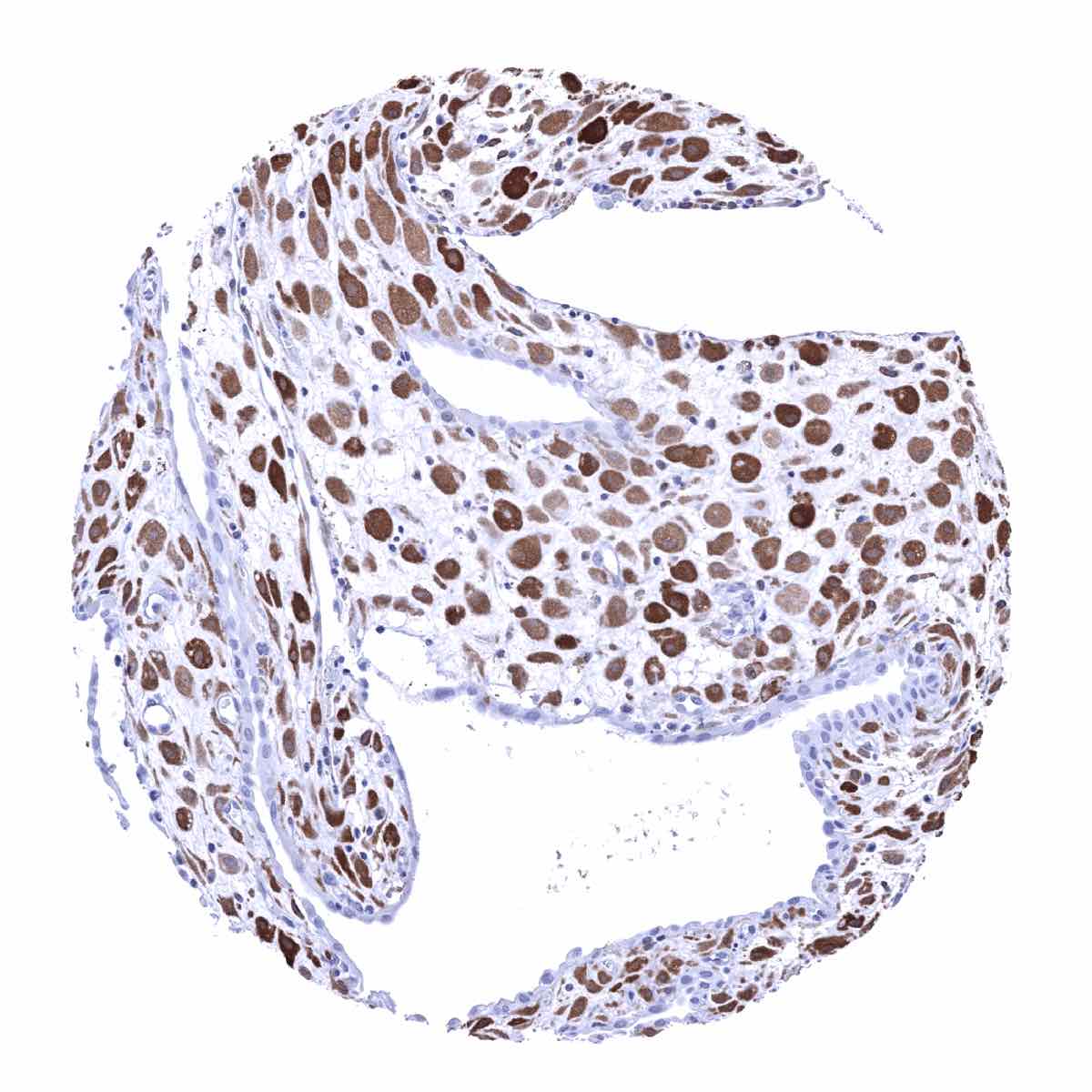
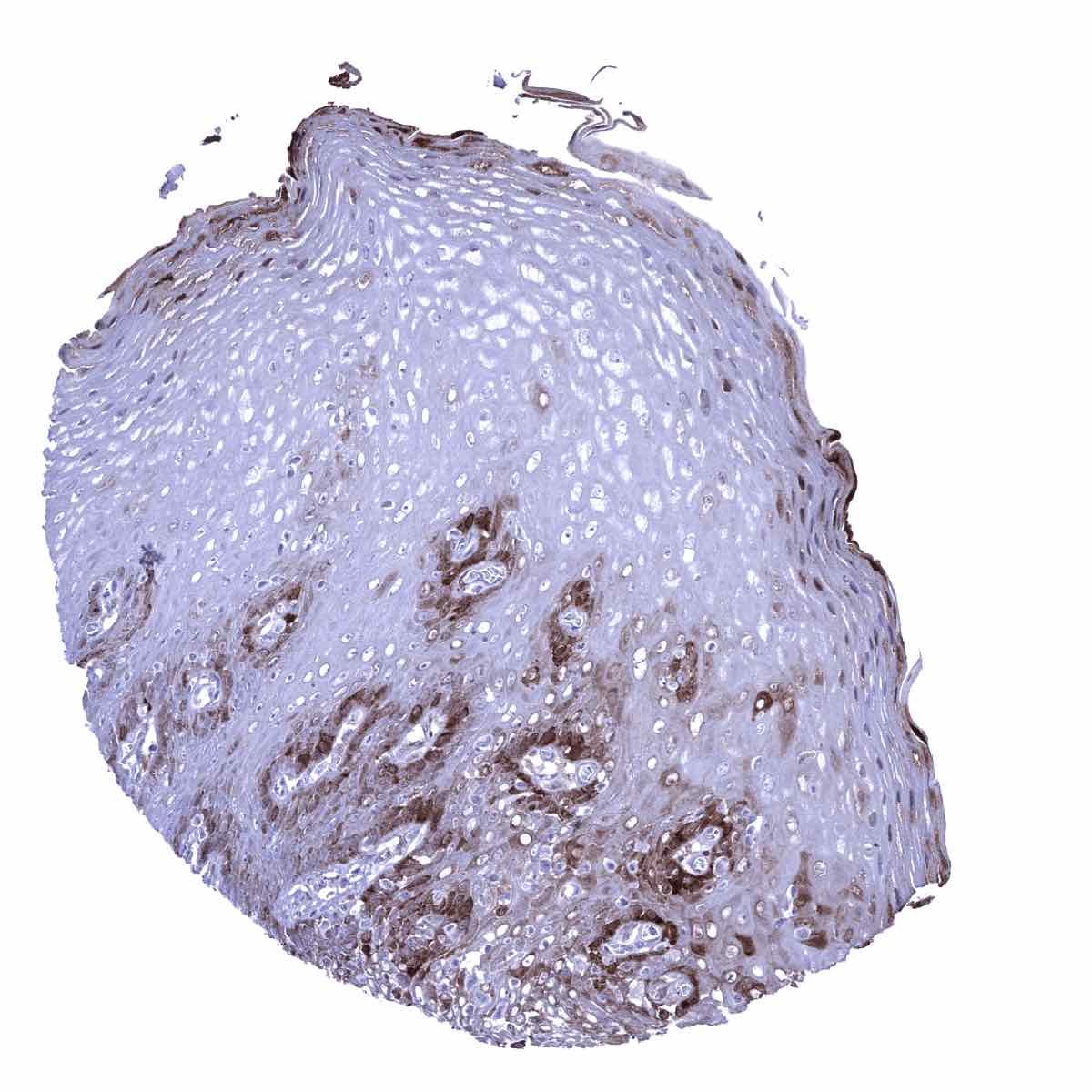
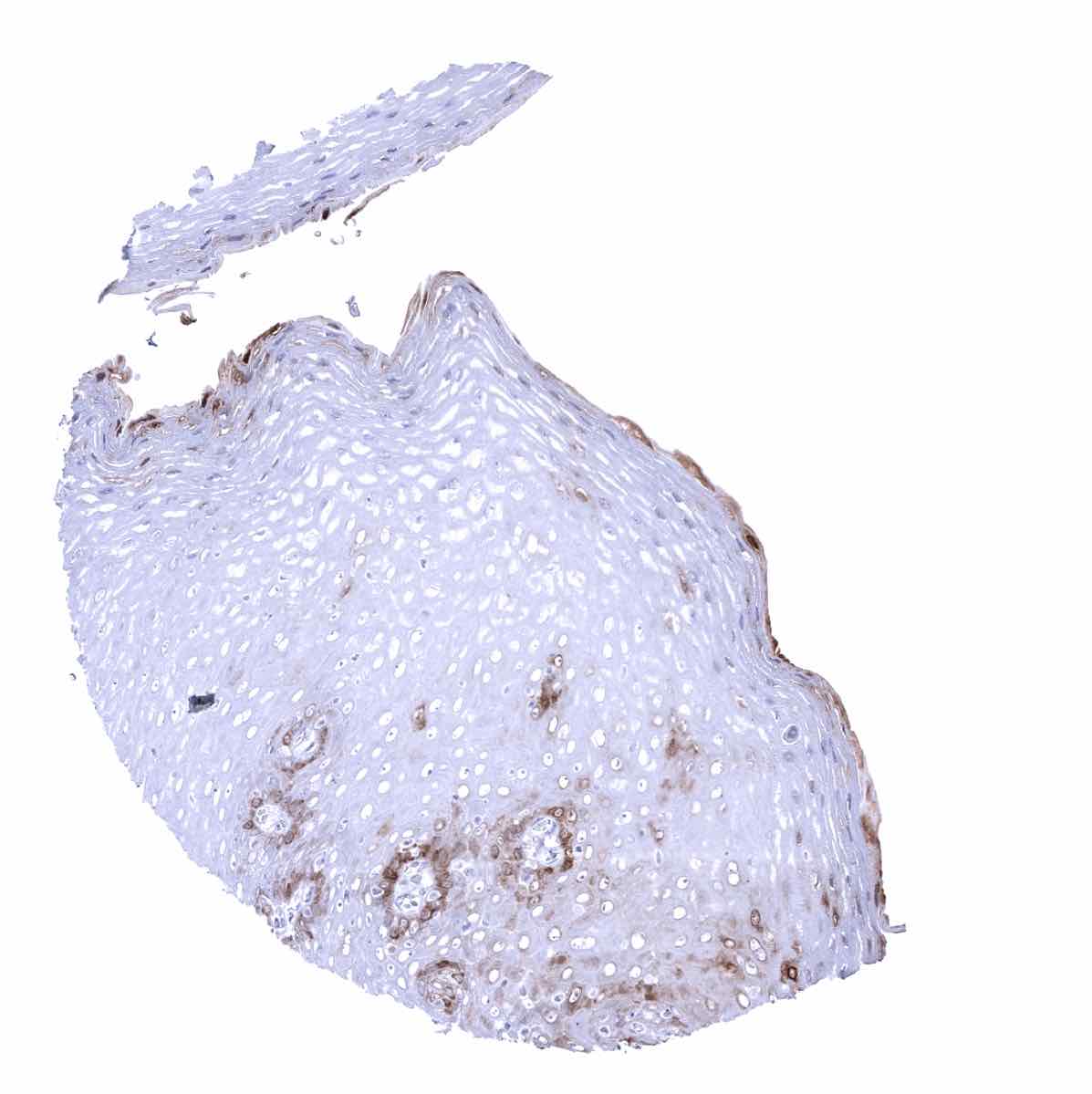
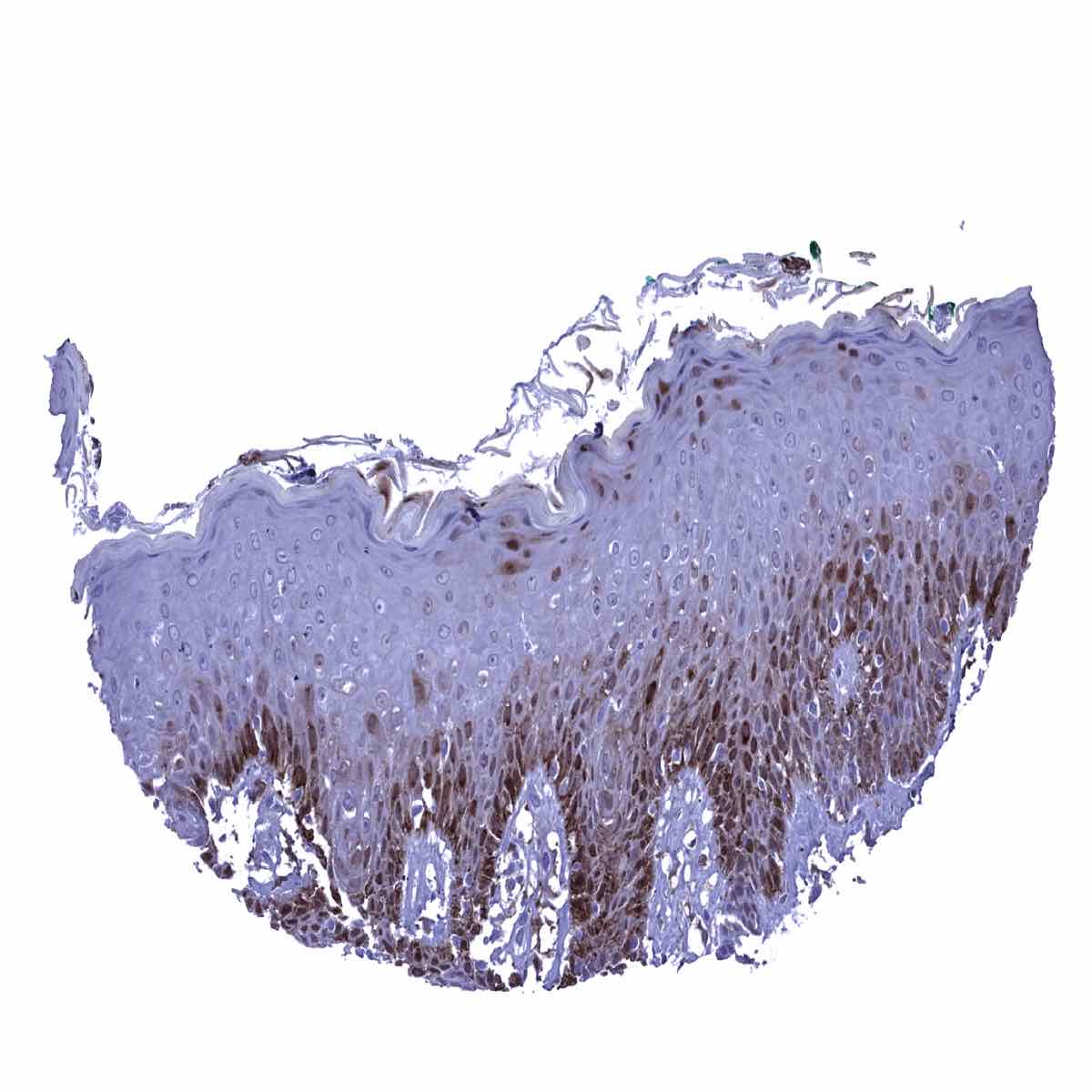
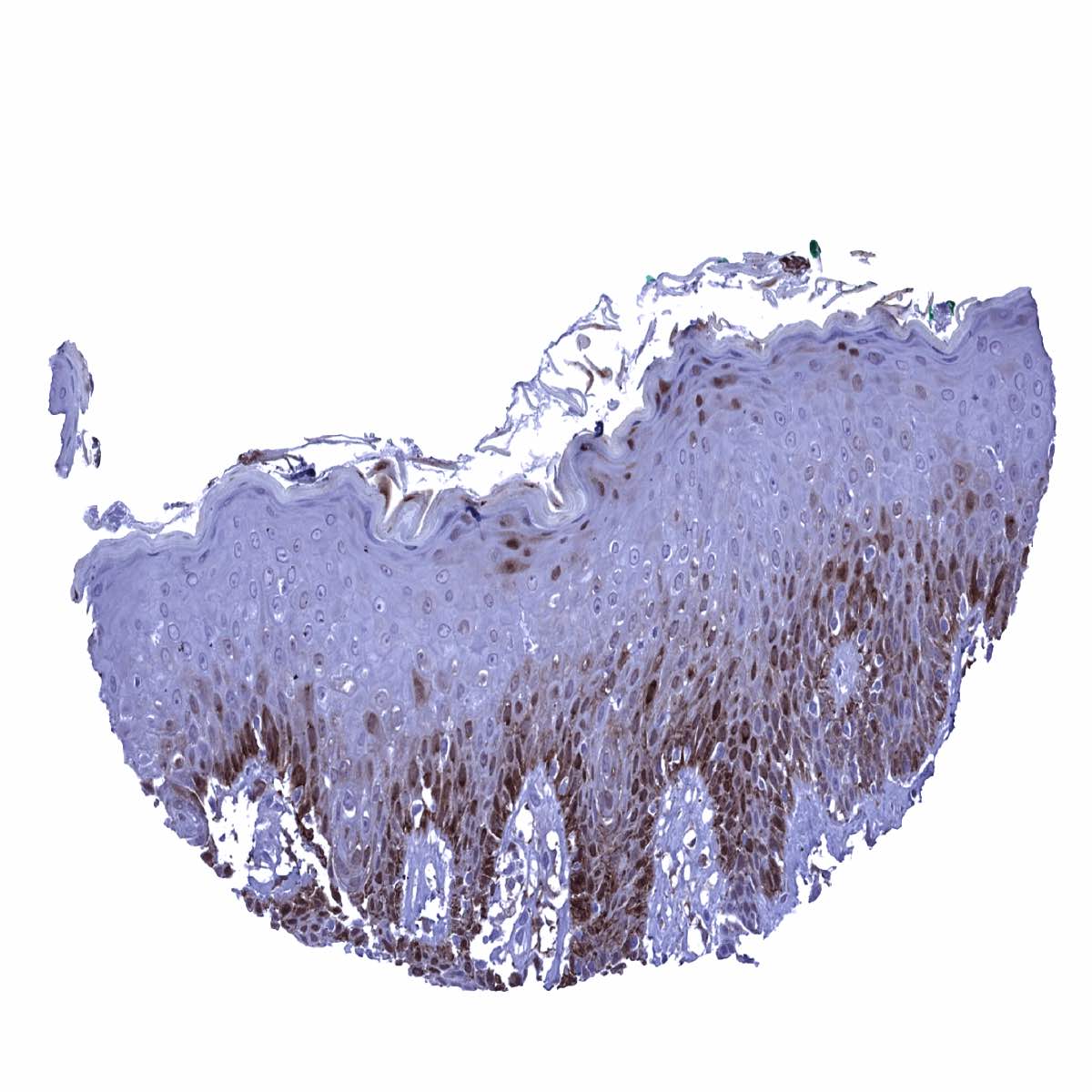
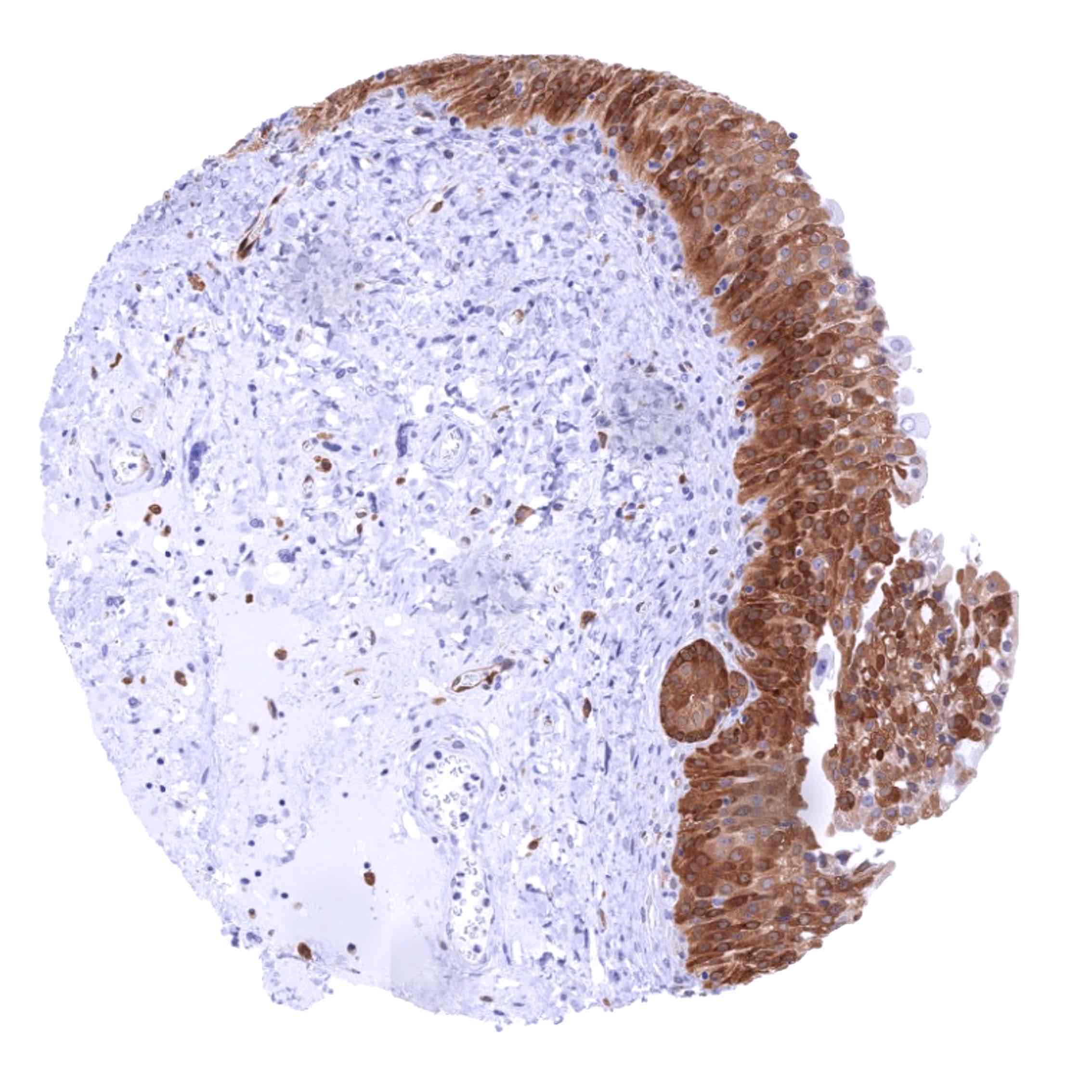
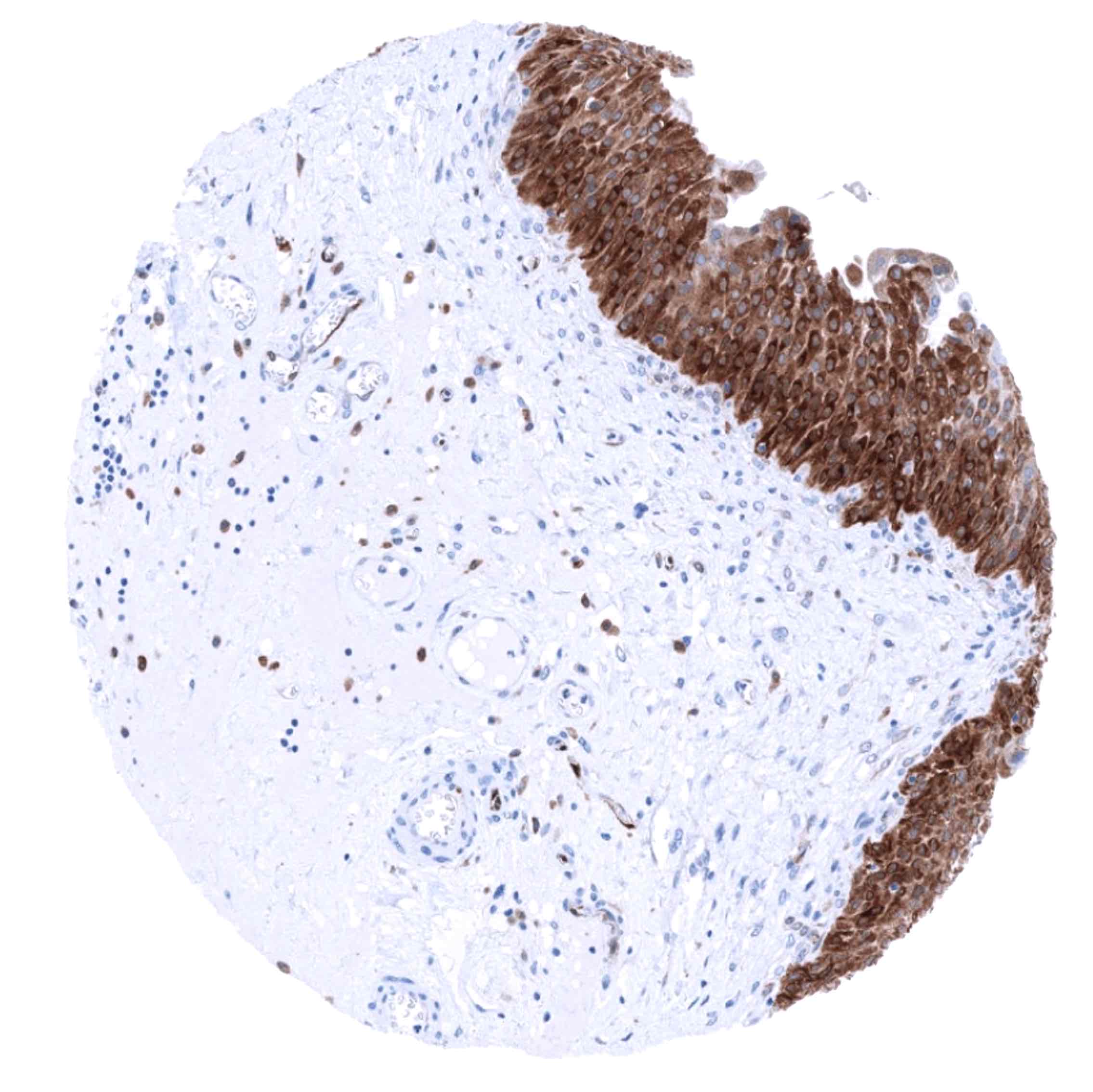
Squamous epithelium: A nuclear and cytoplasmic staining of variable intensity is preferentially seen in the lower third and/or in the top layers of squamous epithelium of various sites including skin and tonsil crypts. A strong staining is also seen in sebaceous glands and hair follicles.
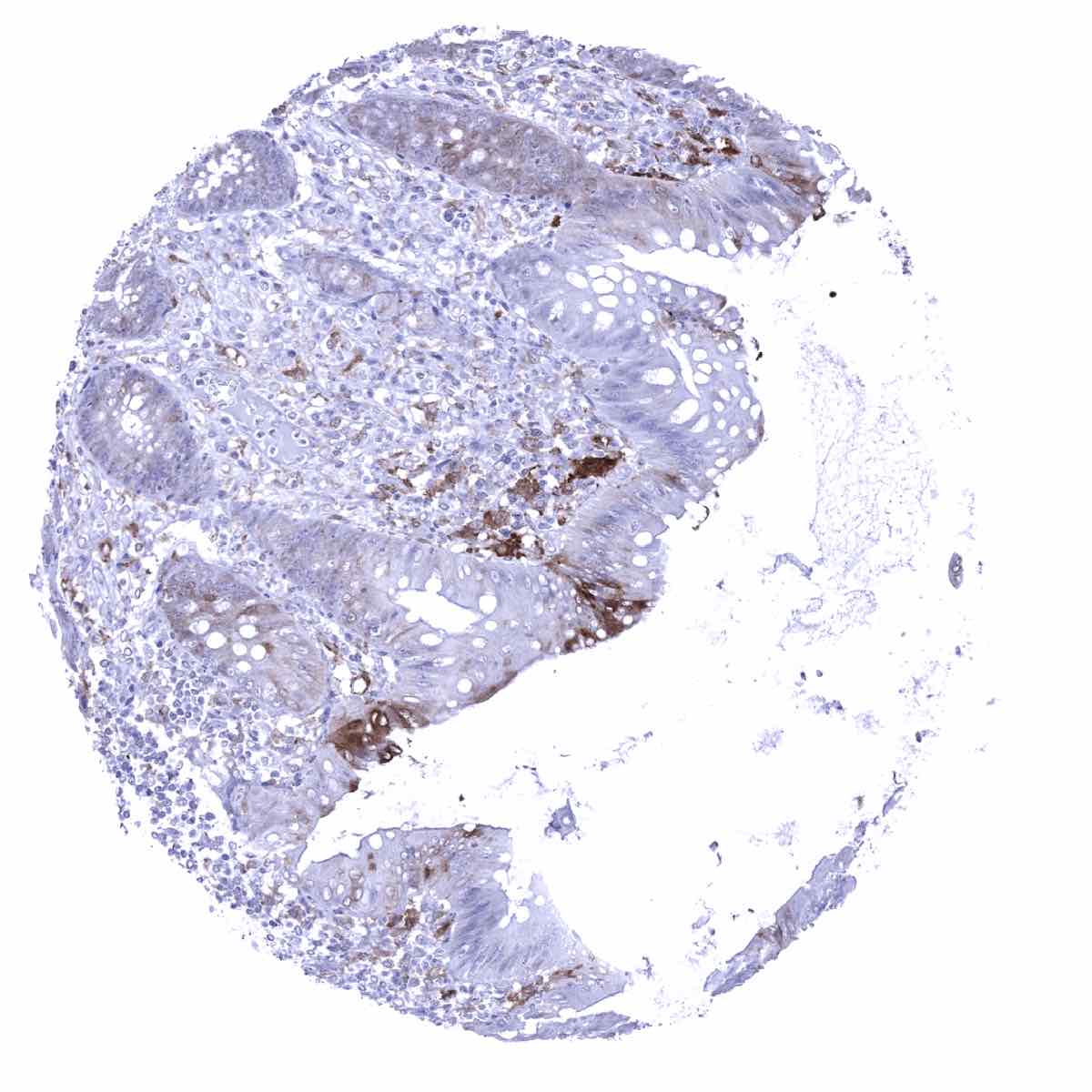
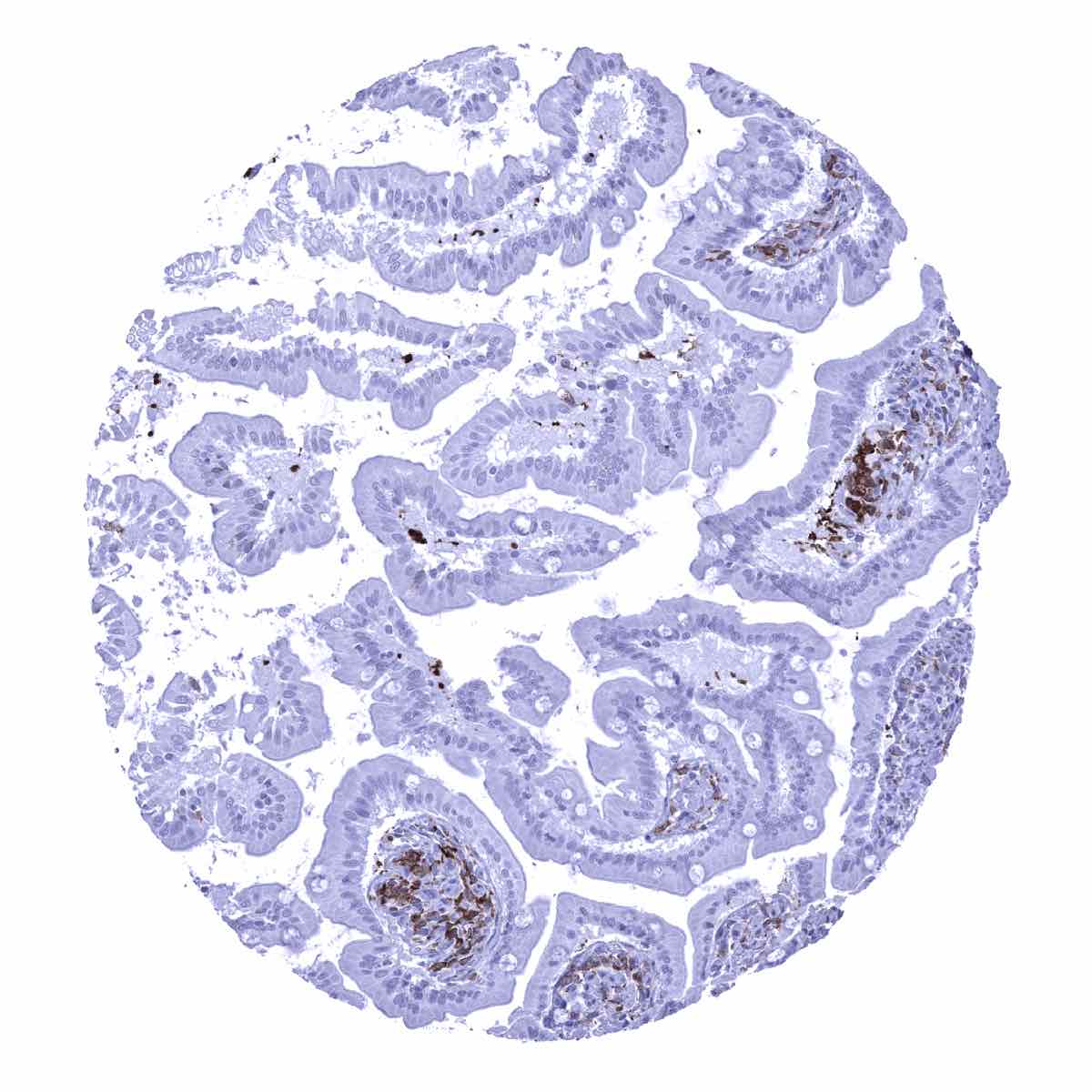
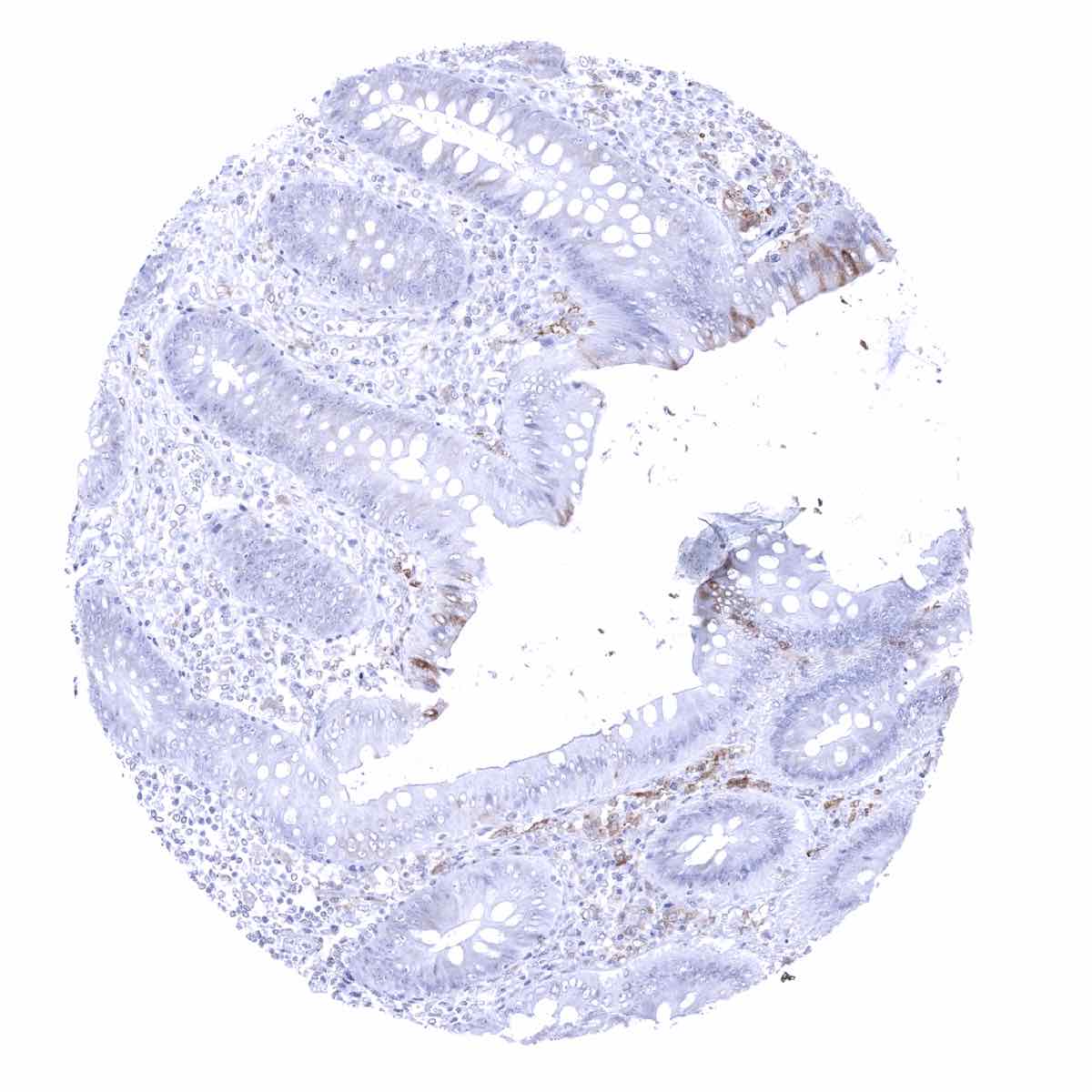
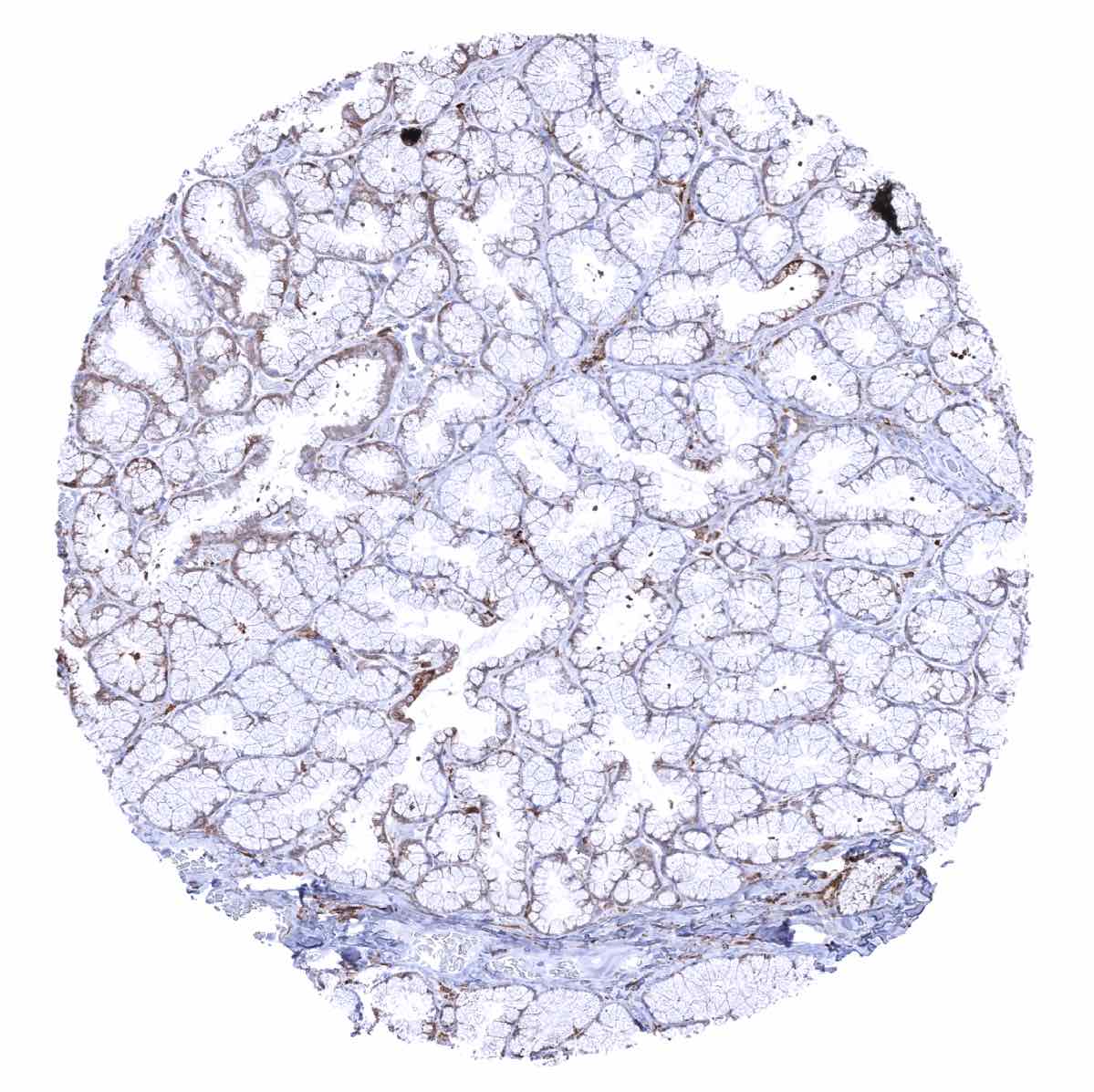
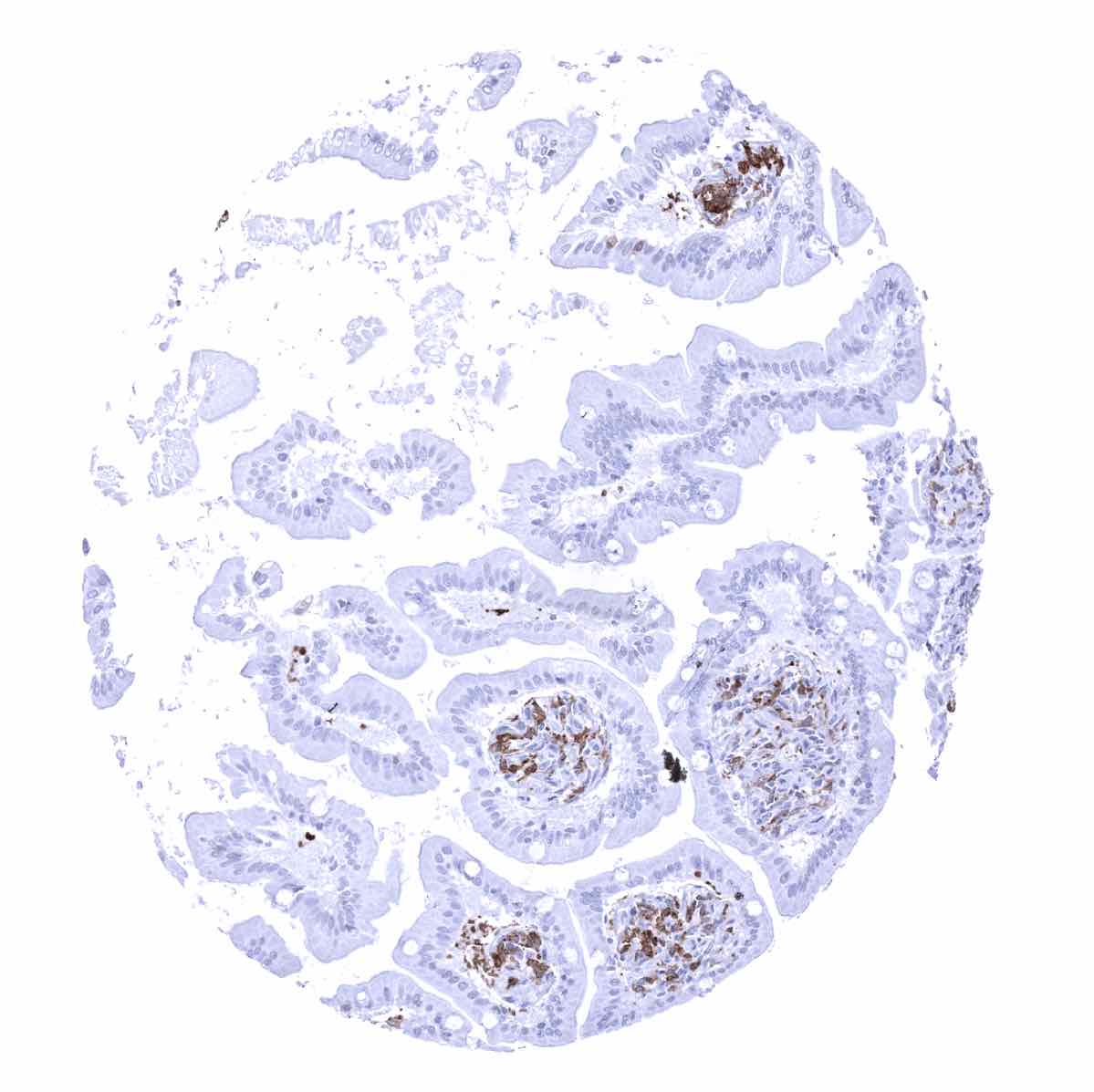
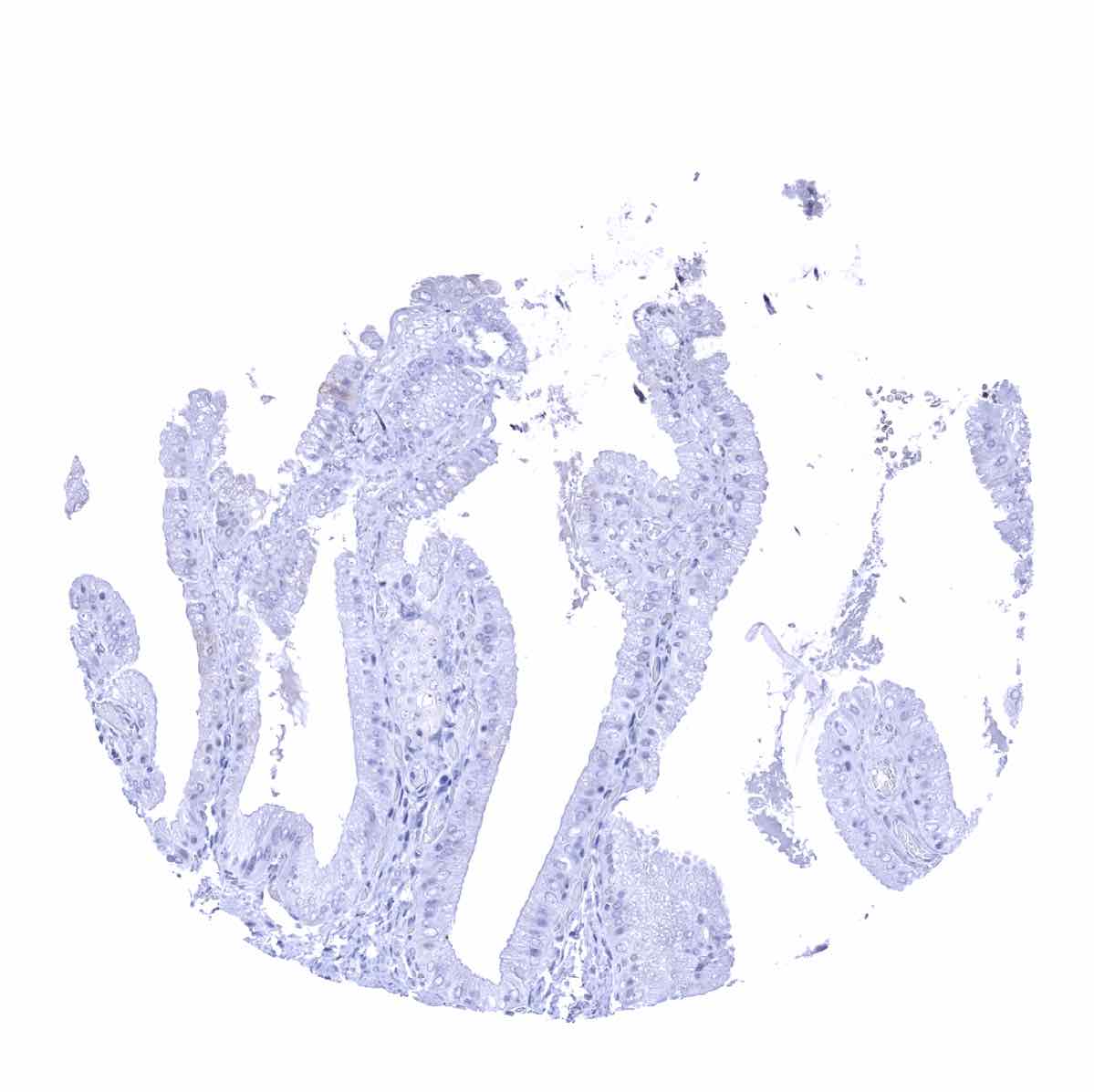
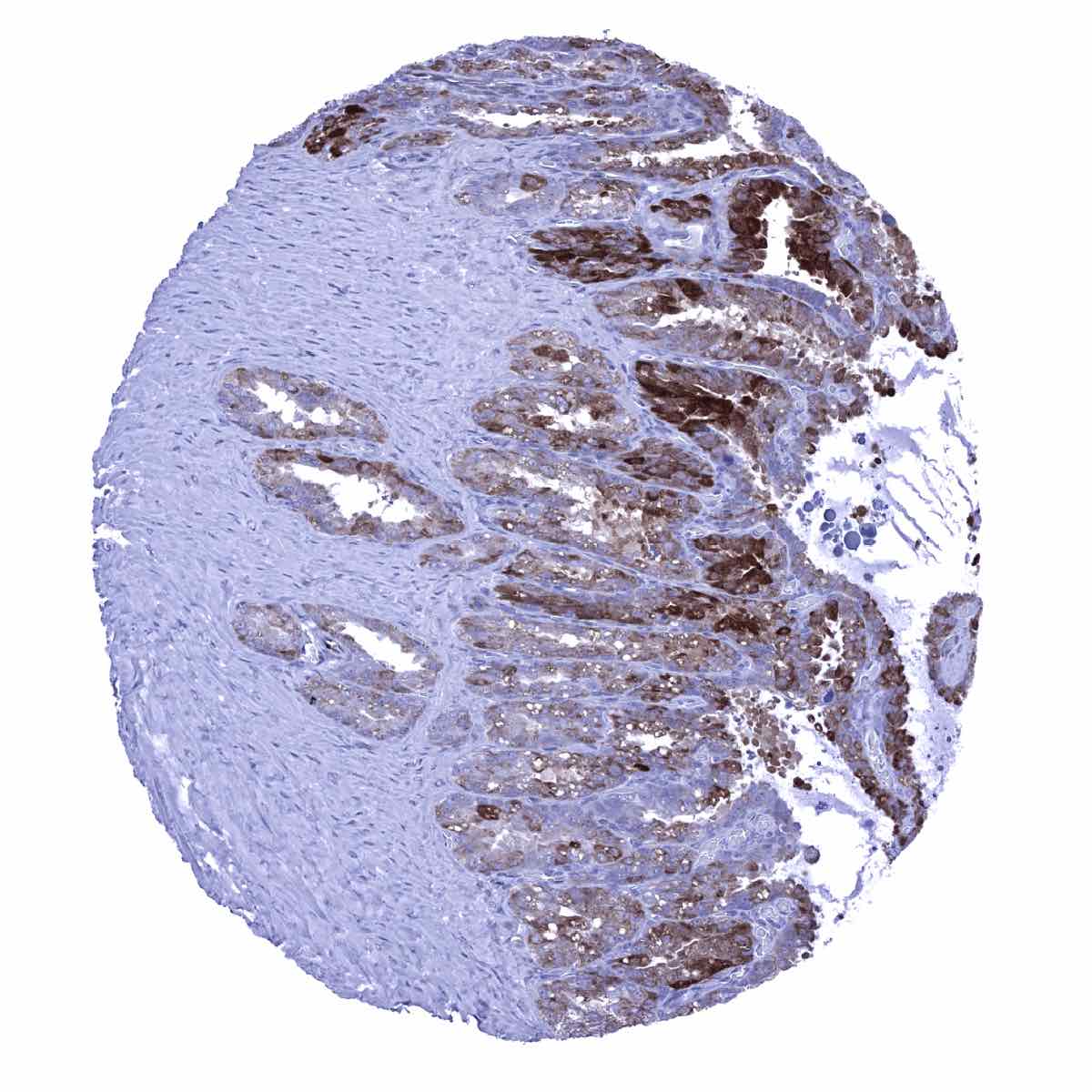
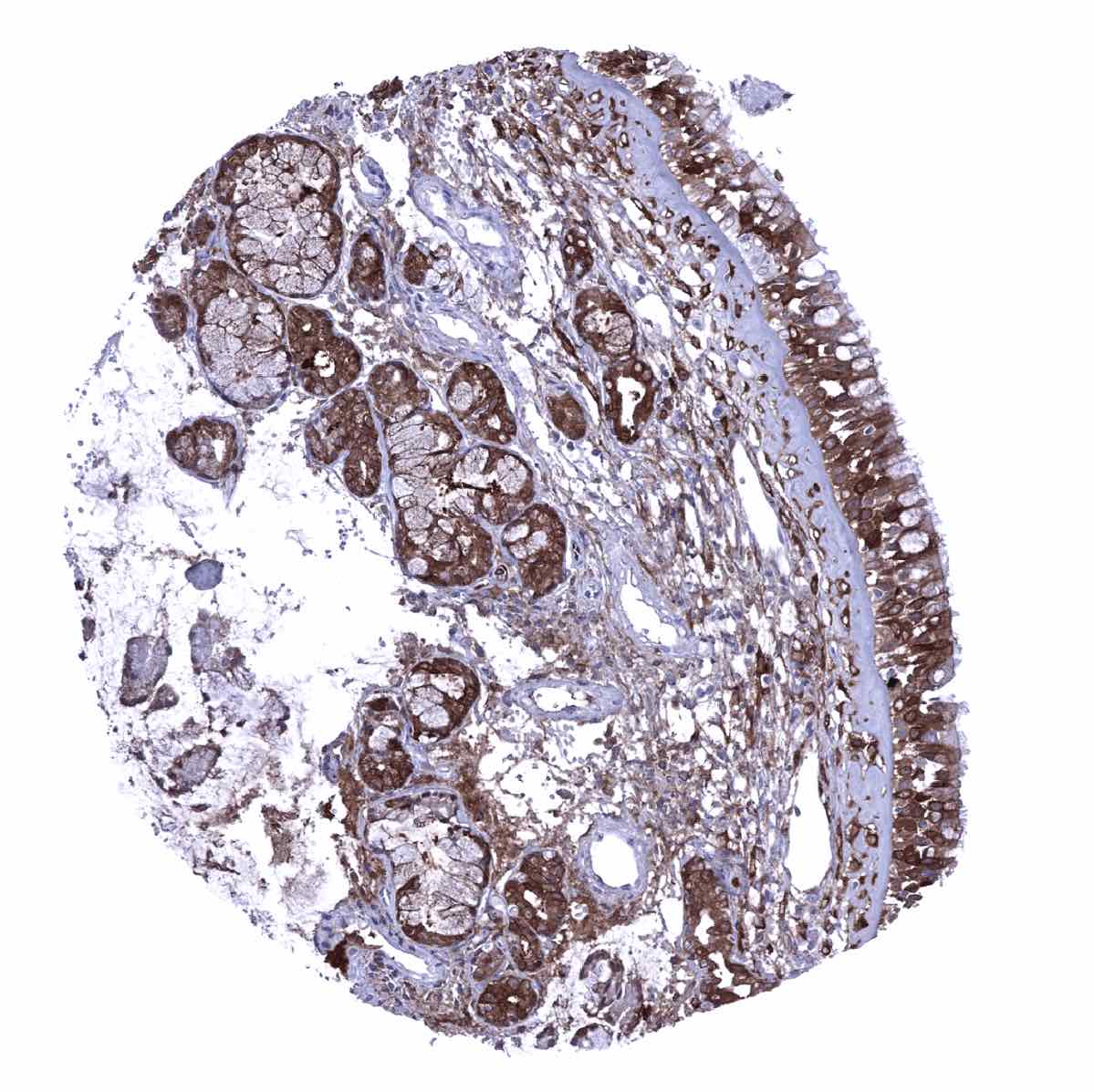
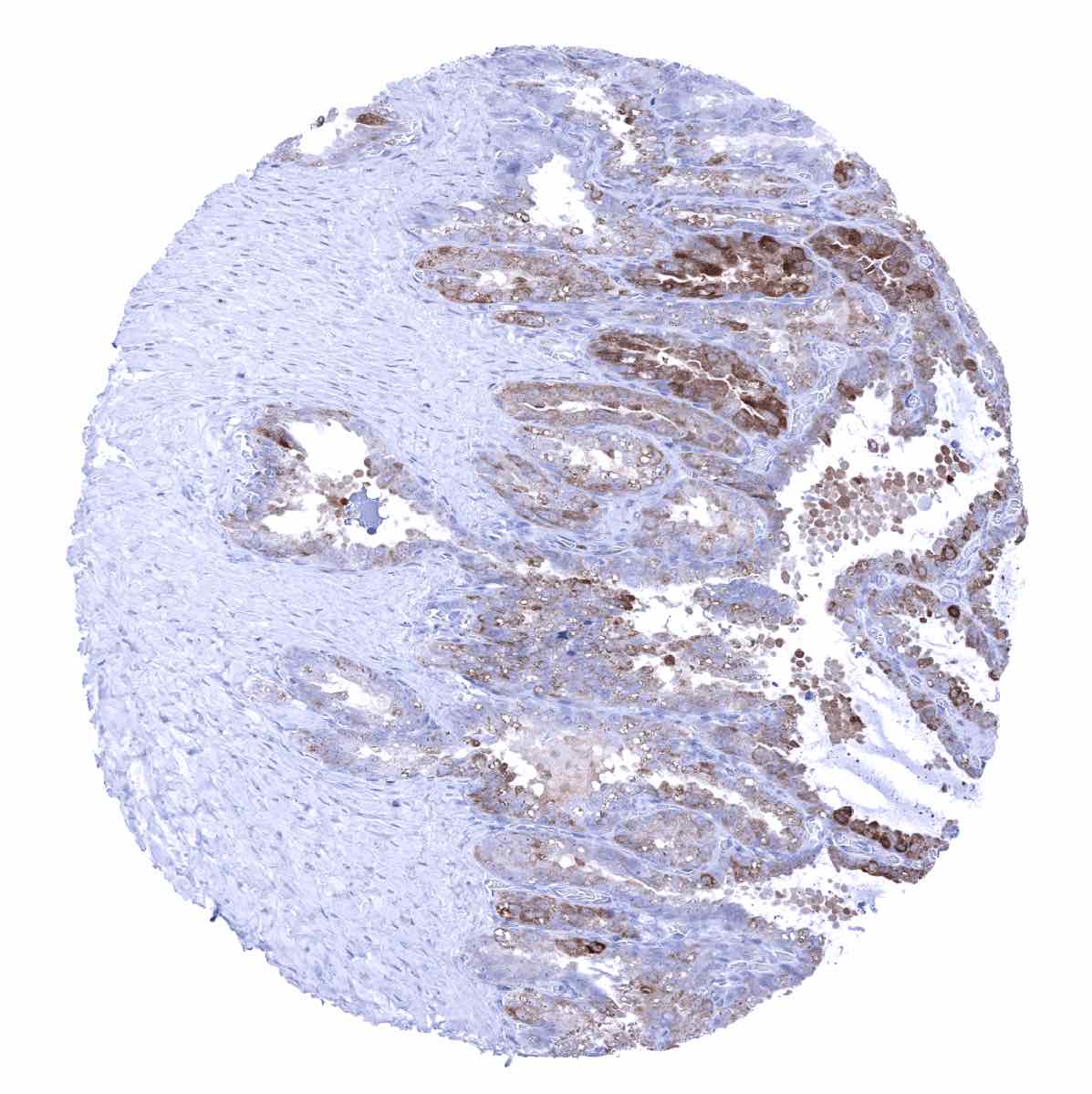
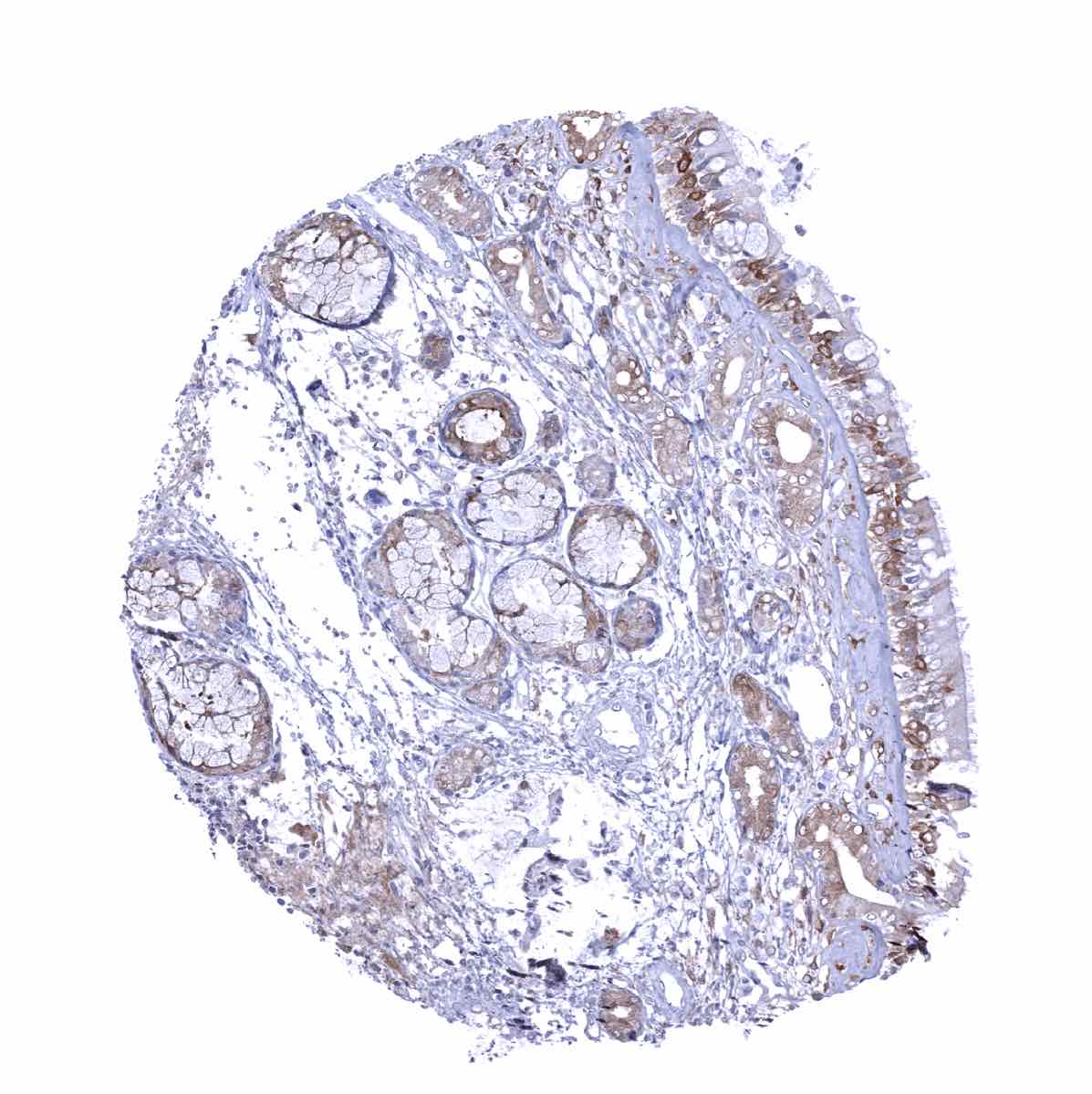
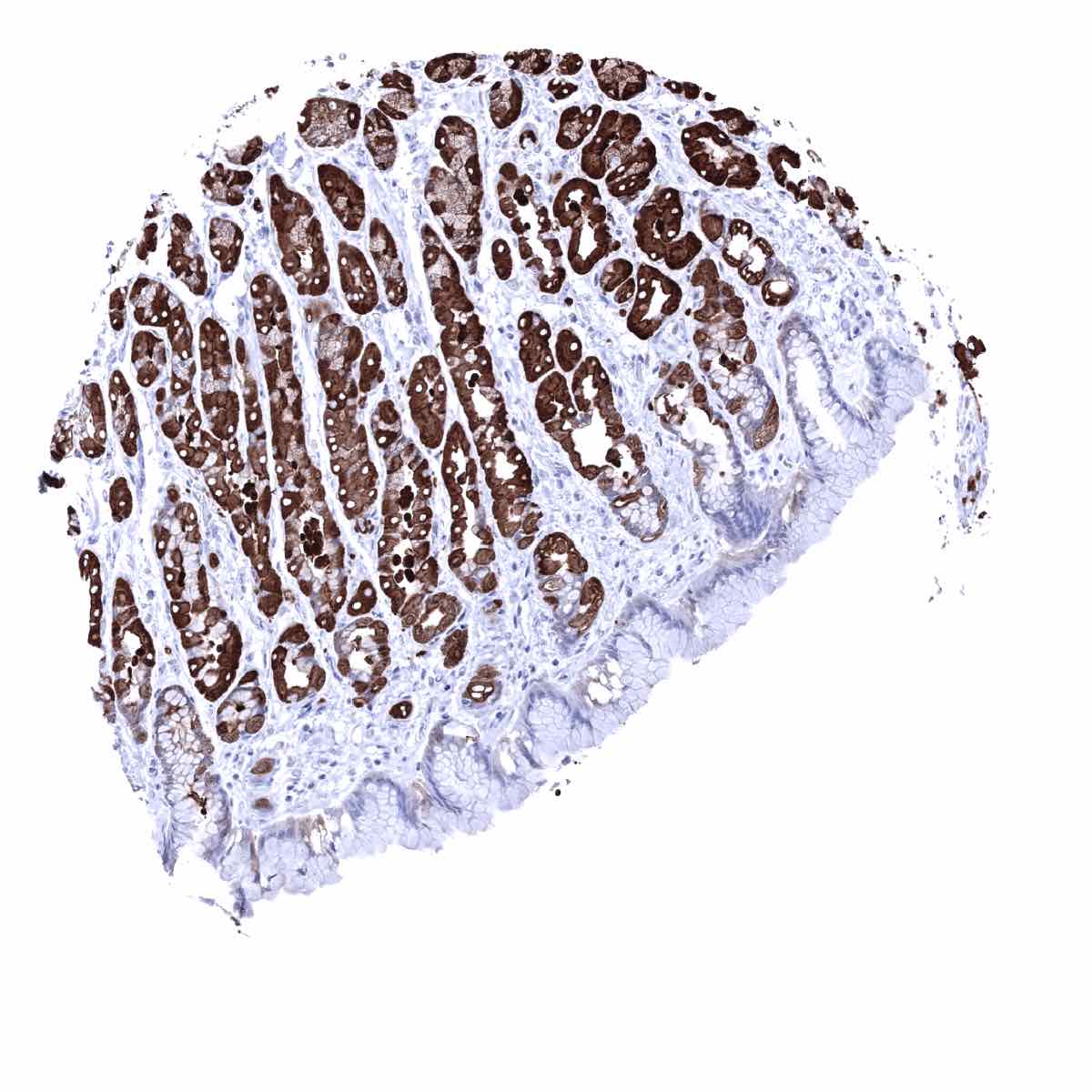
Gastrointestinal tract: Epithelial cell staining is strongest in the stomach (glandular cells > surface cells, corpus>antrum). In the small intestine and colorectum, GS staining predominates in inflammatory cells and is only focal and faint in epithelial cells. A strong staining is also seen in the transitional epithelium of the anal canal. In the liver, staining is strong in centrilobular hepatocytes, weak to moderate in Kupffer cells but absent in periportal hepatocytes and bile ducts. Also in the gallbladder, epithelial cell staining is focal and faint. In the pancreas, a weak to moderate staining can be focally observed in acinar cells, intercalated ducts and excretory ducts while islet cells are negative. In salivary glands, a variable, mostly weak GS staining can be seen in excretory and intercalated ducts, glandular (mucinous>serous), and myoepithelial cells
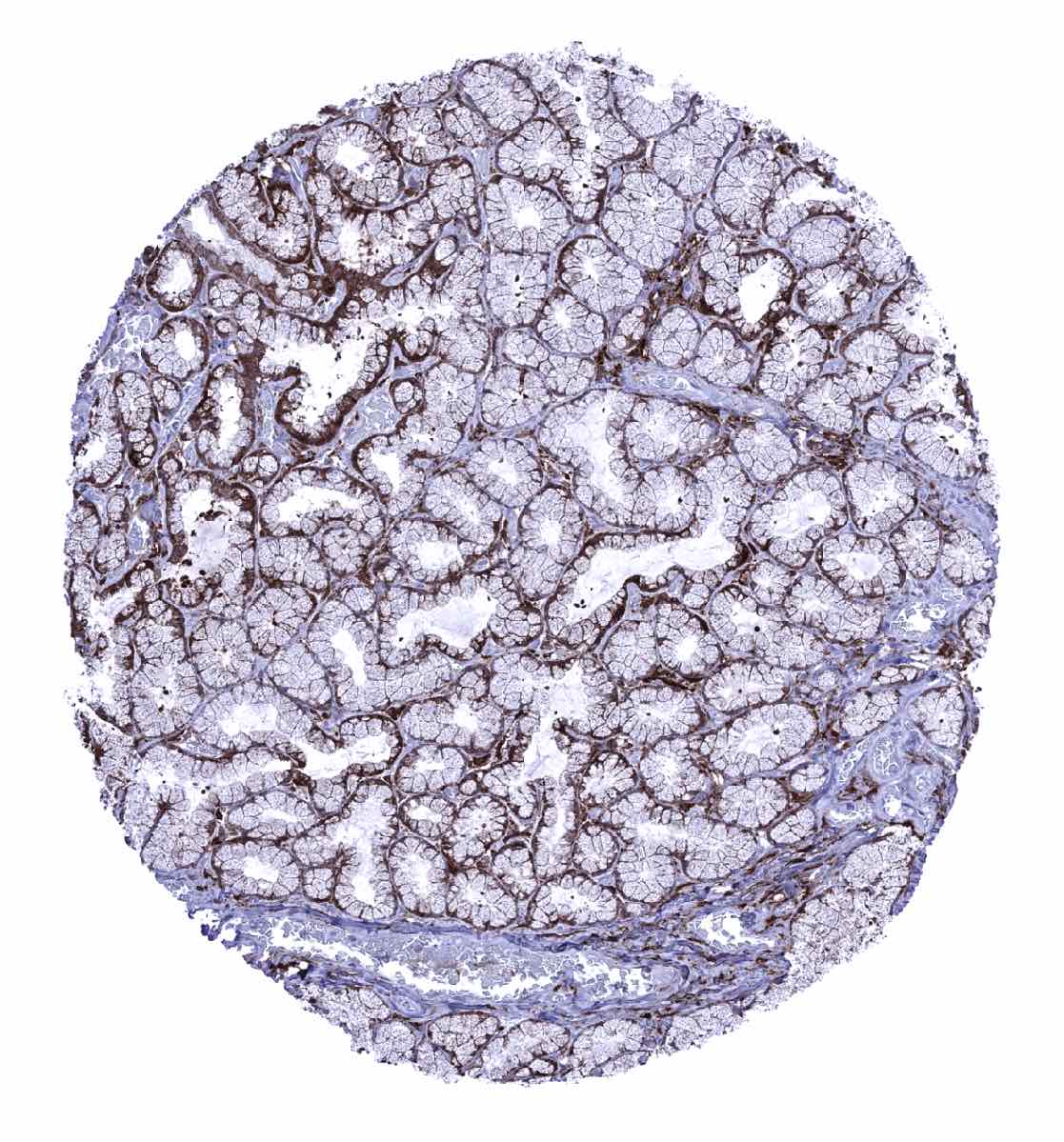
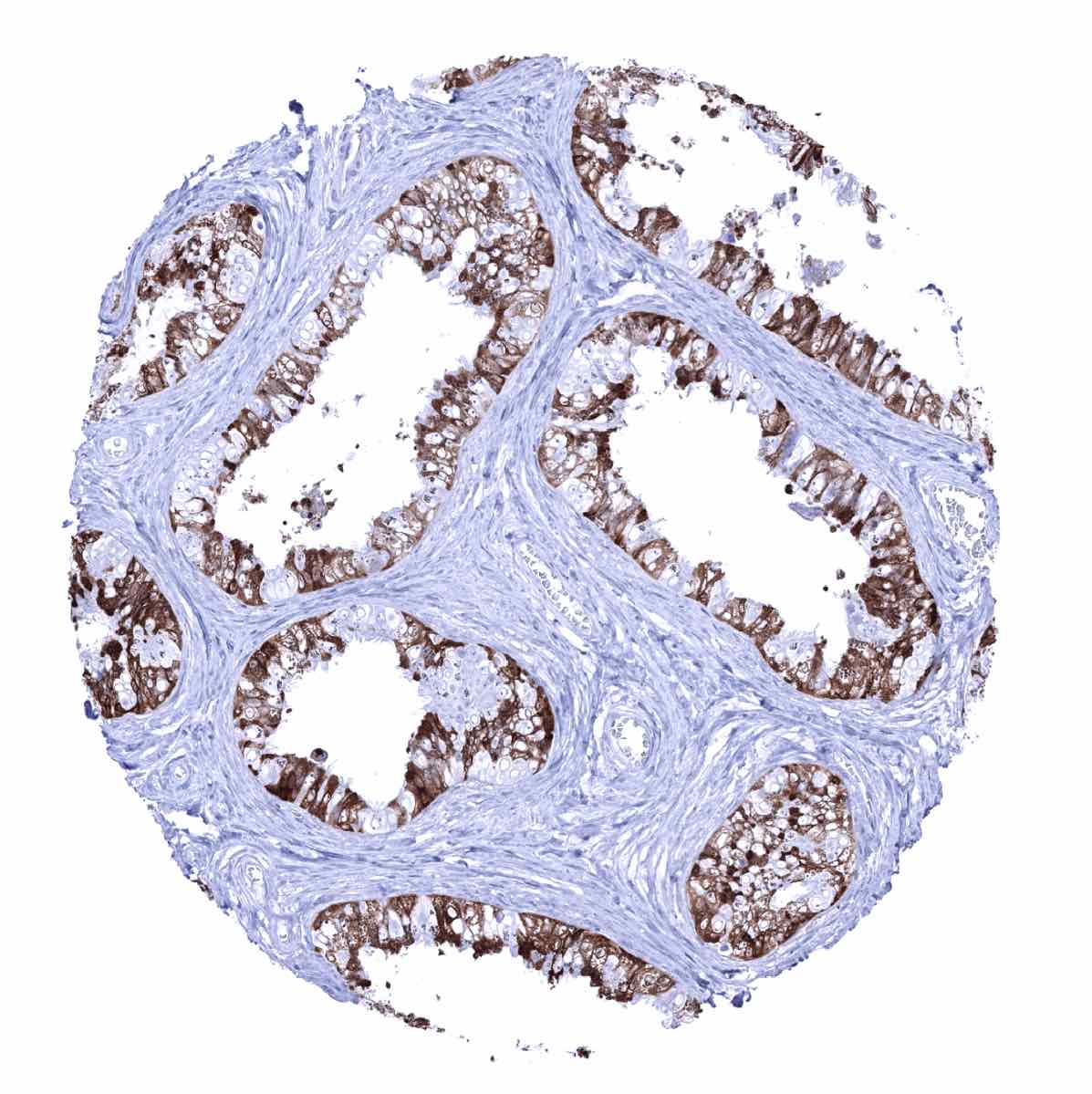
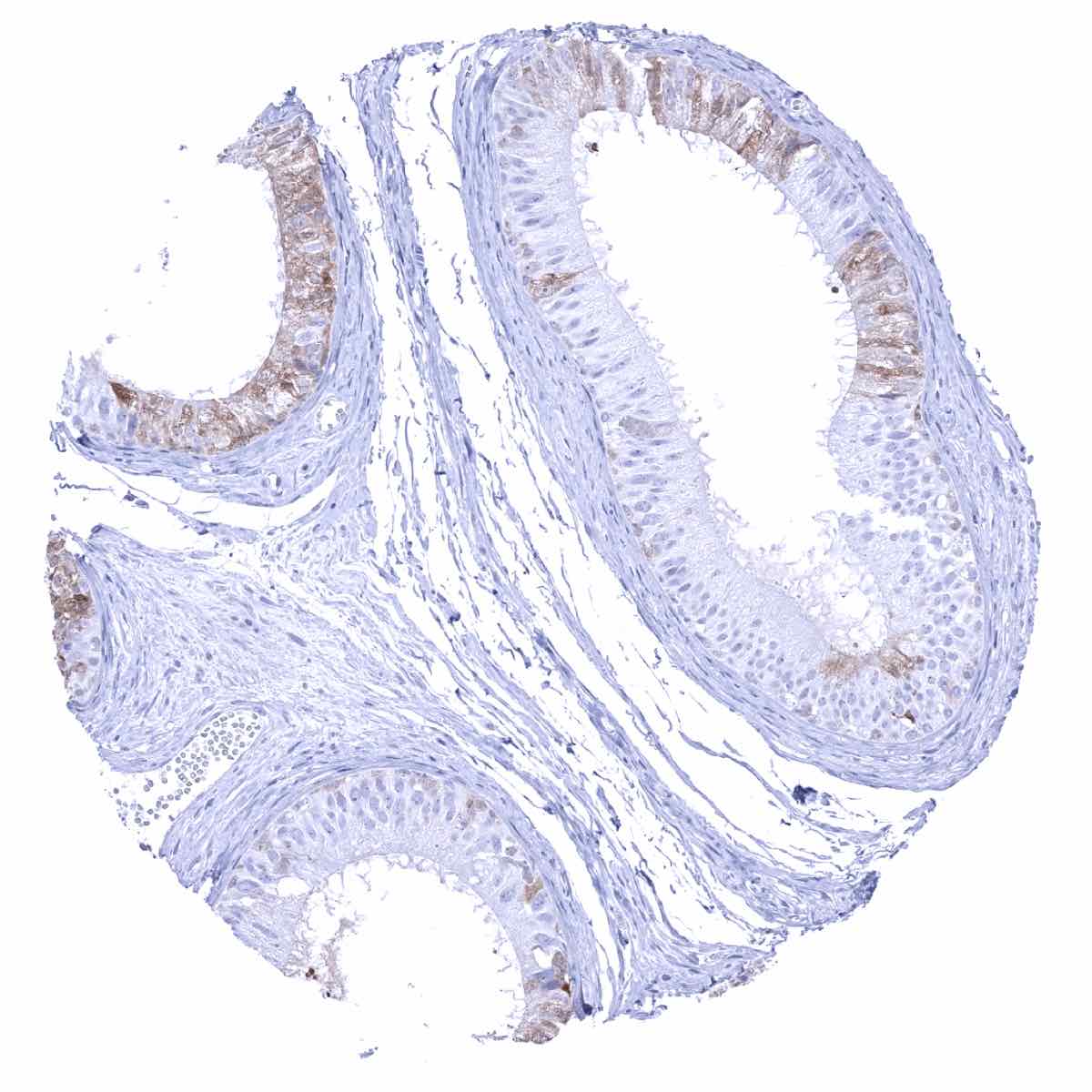
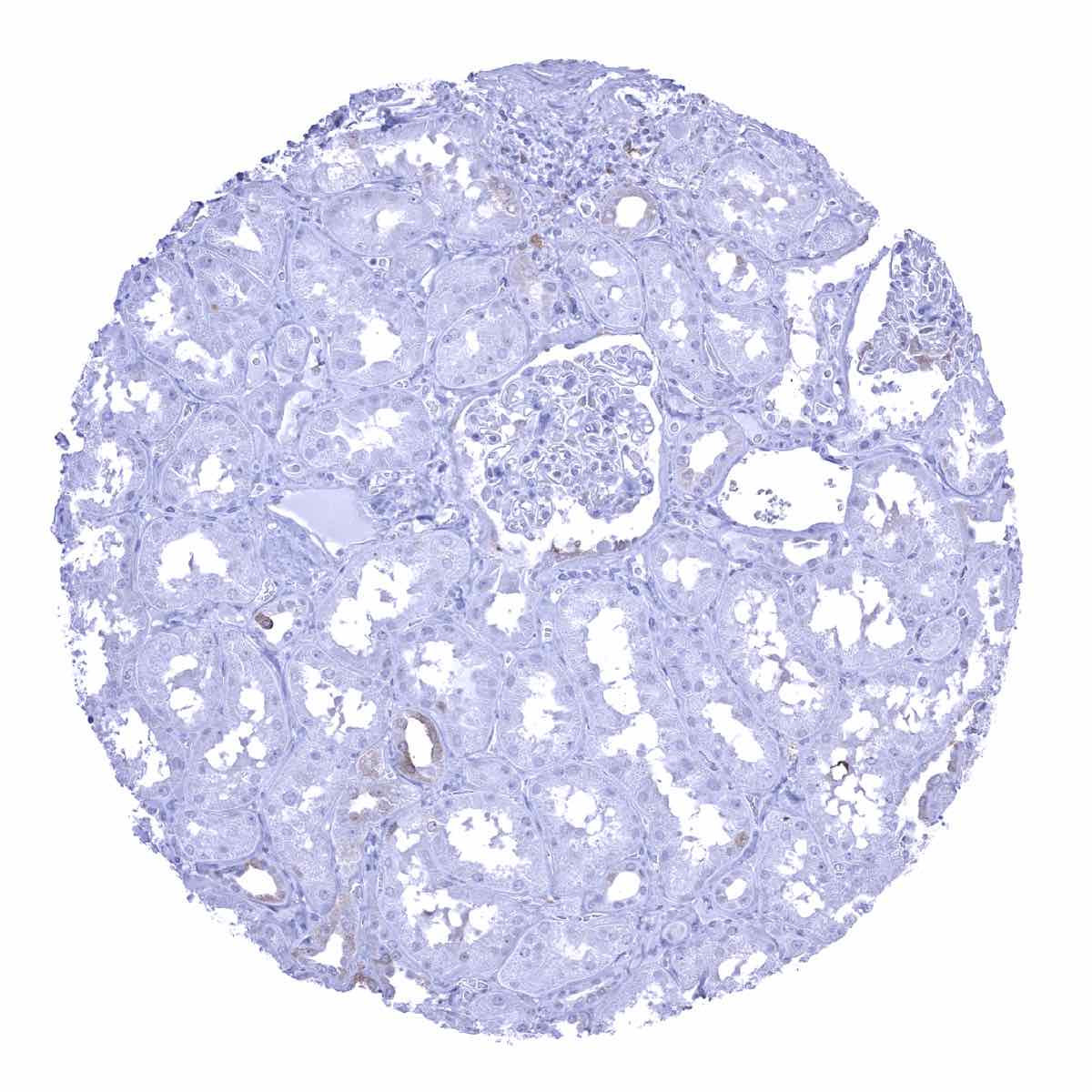
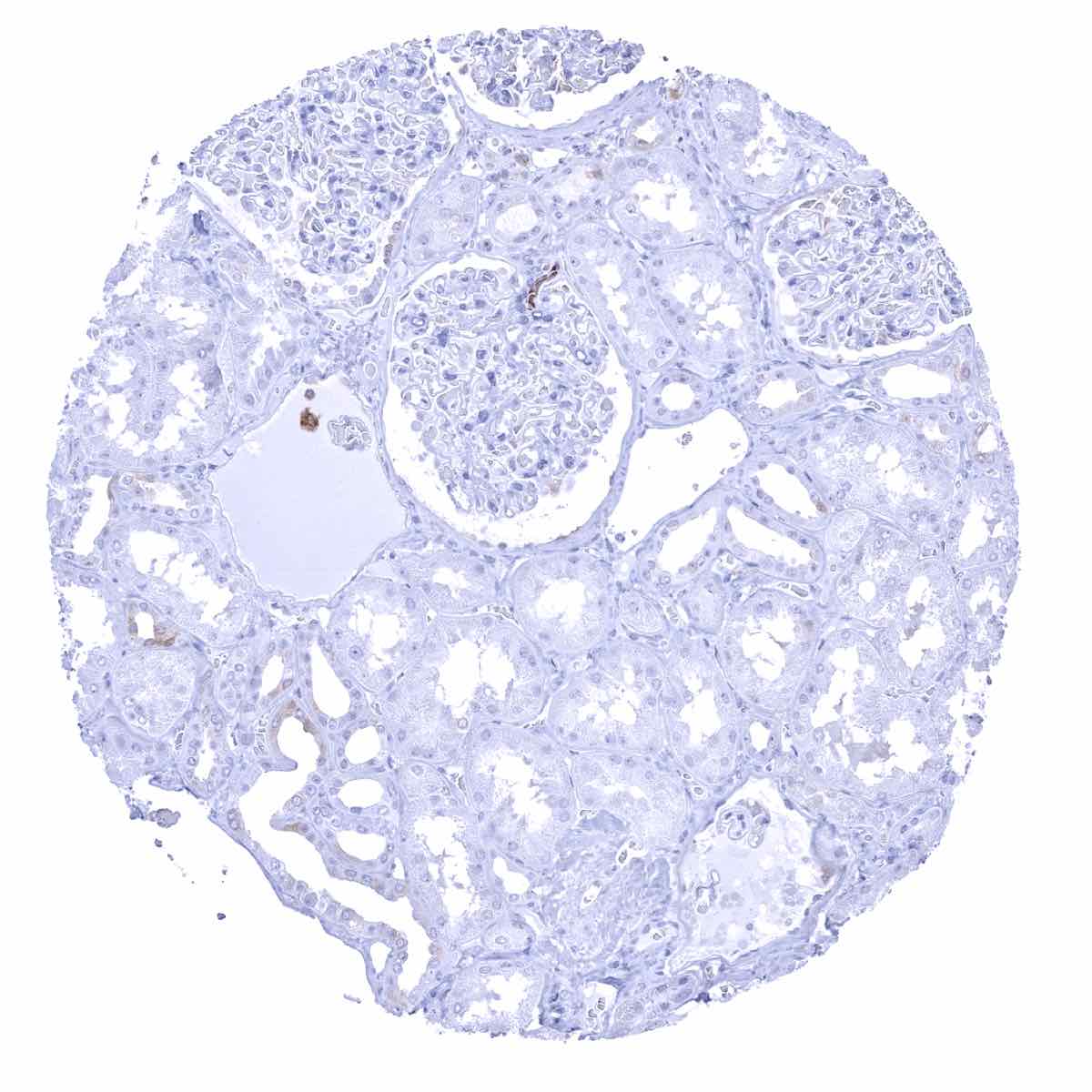
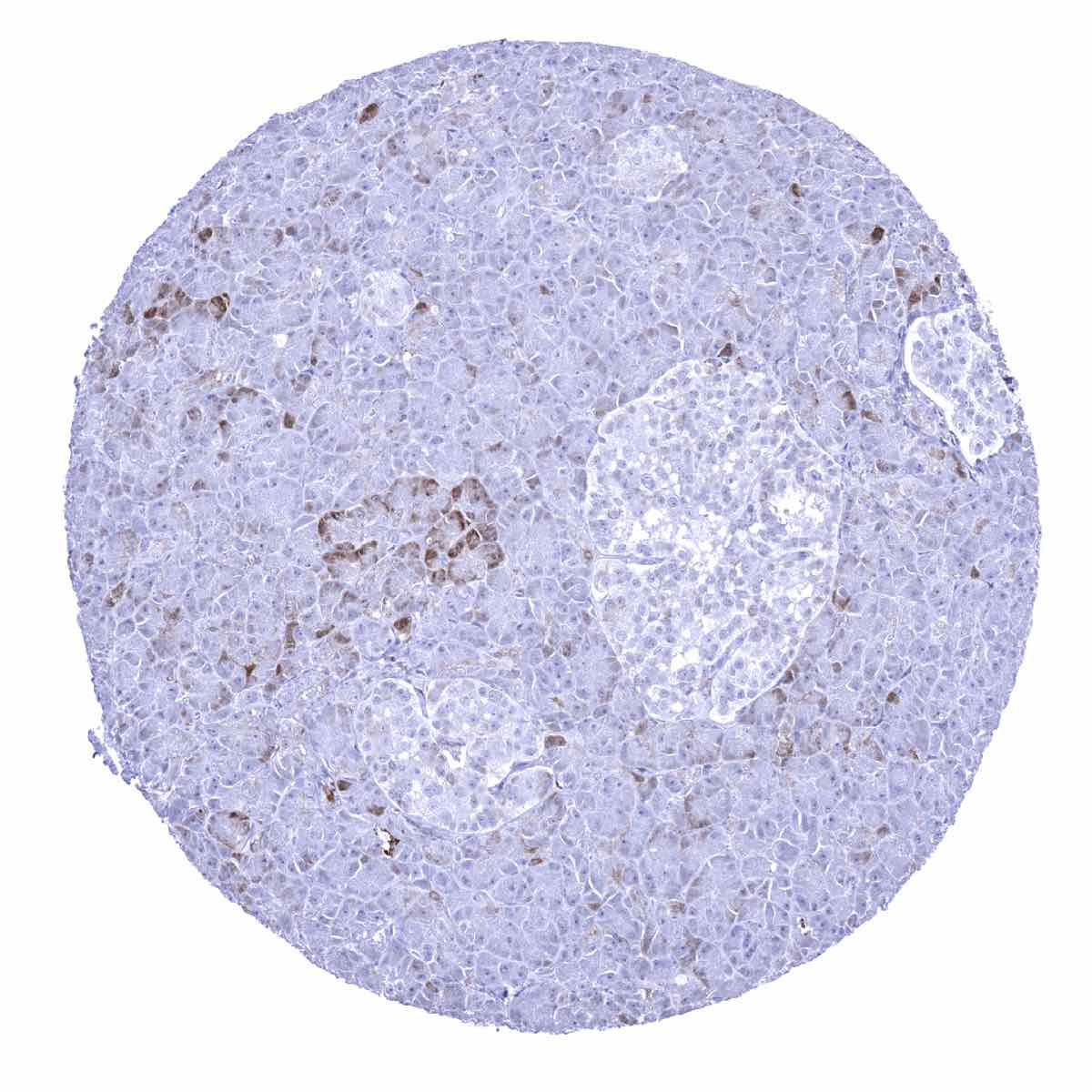
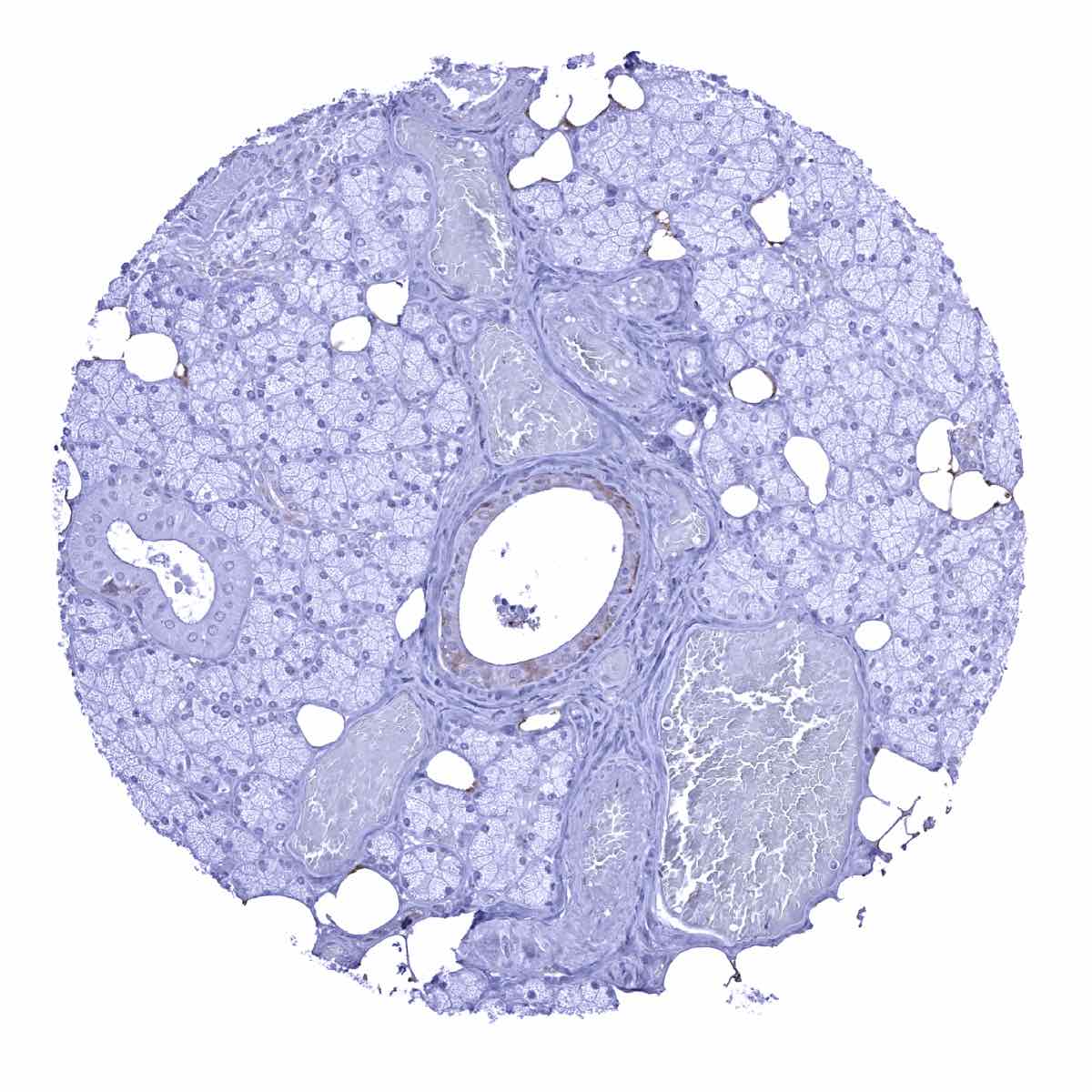
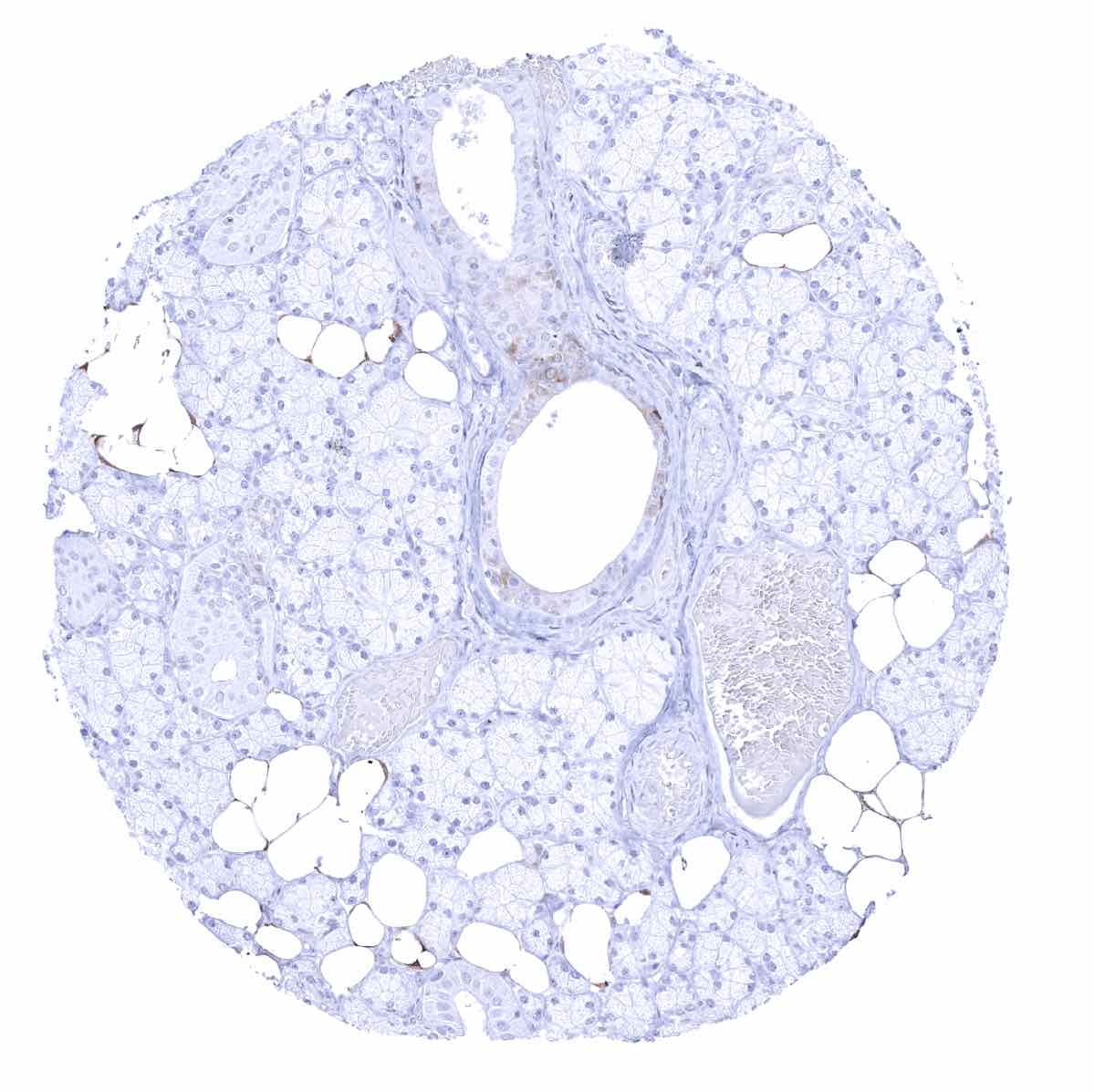
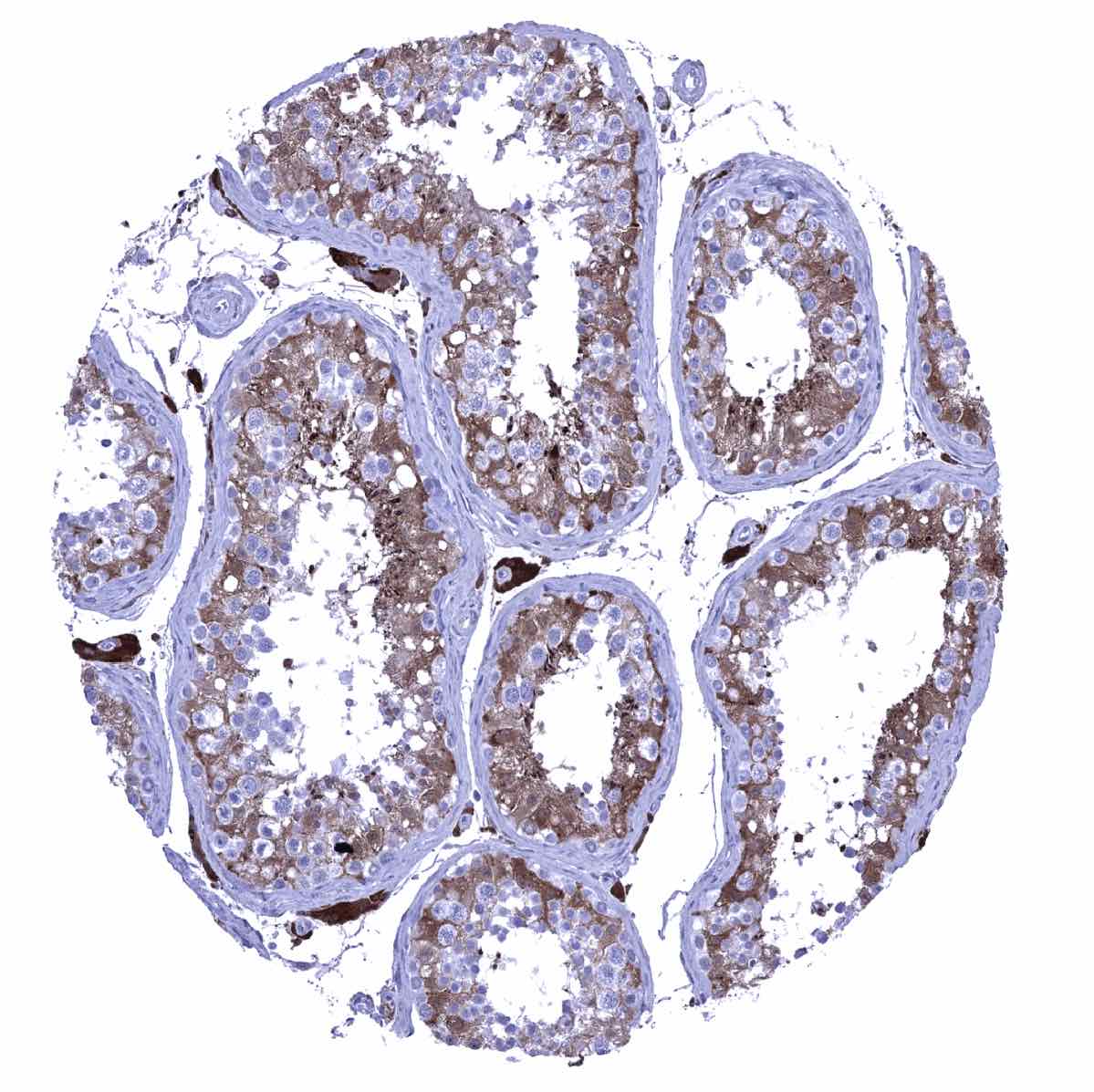
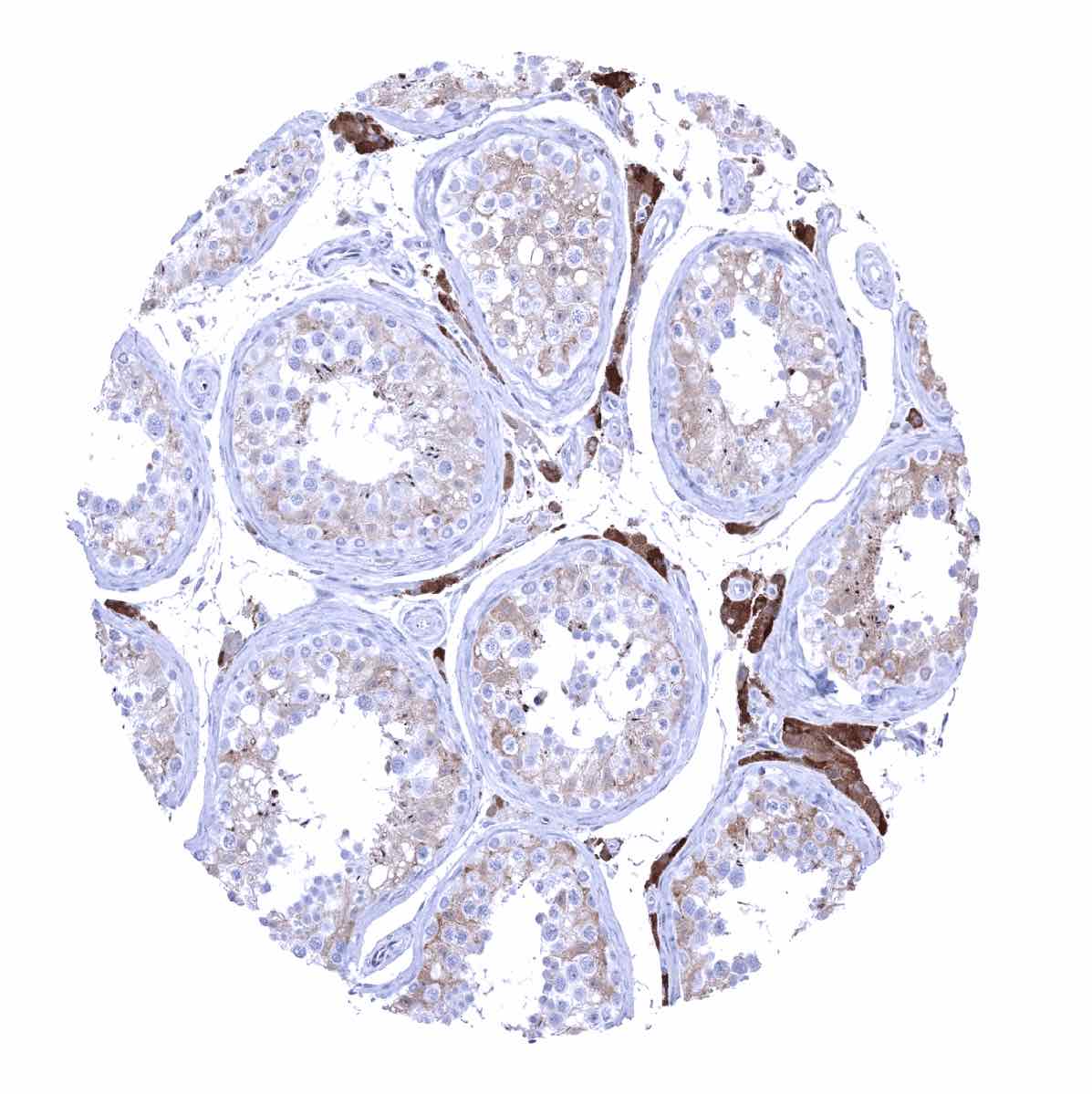
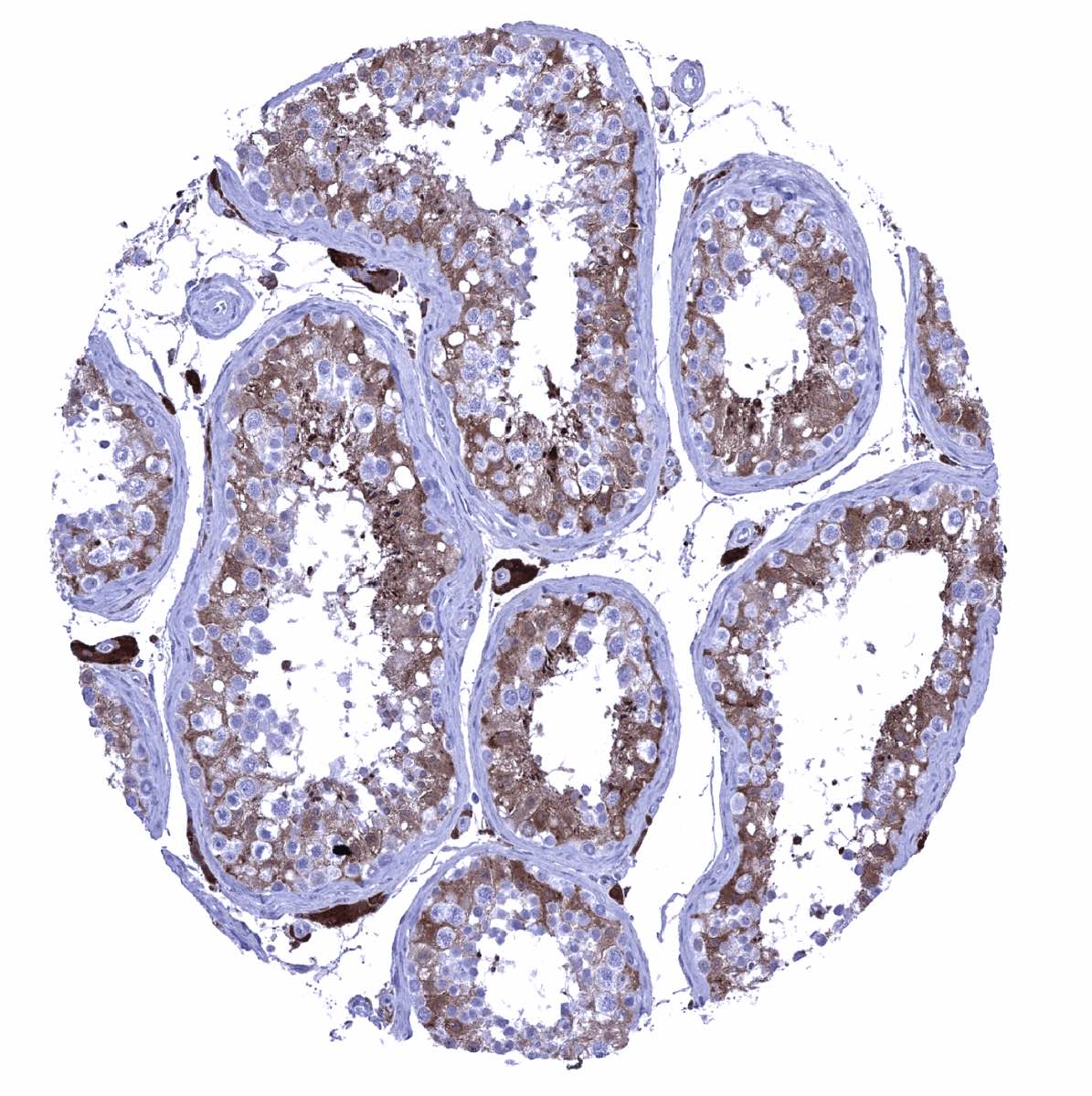
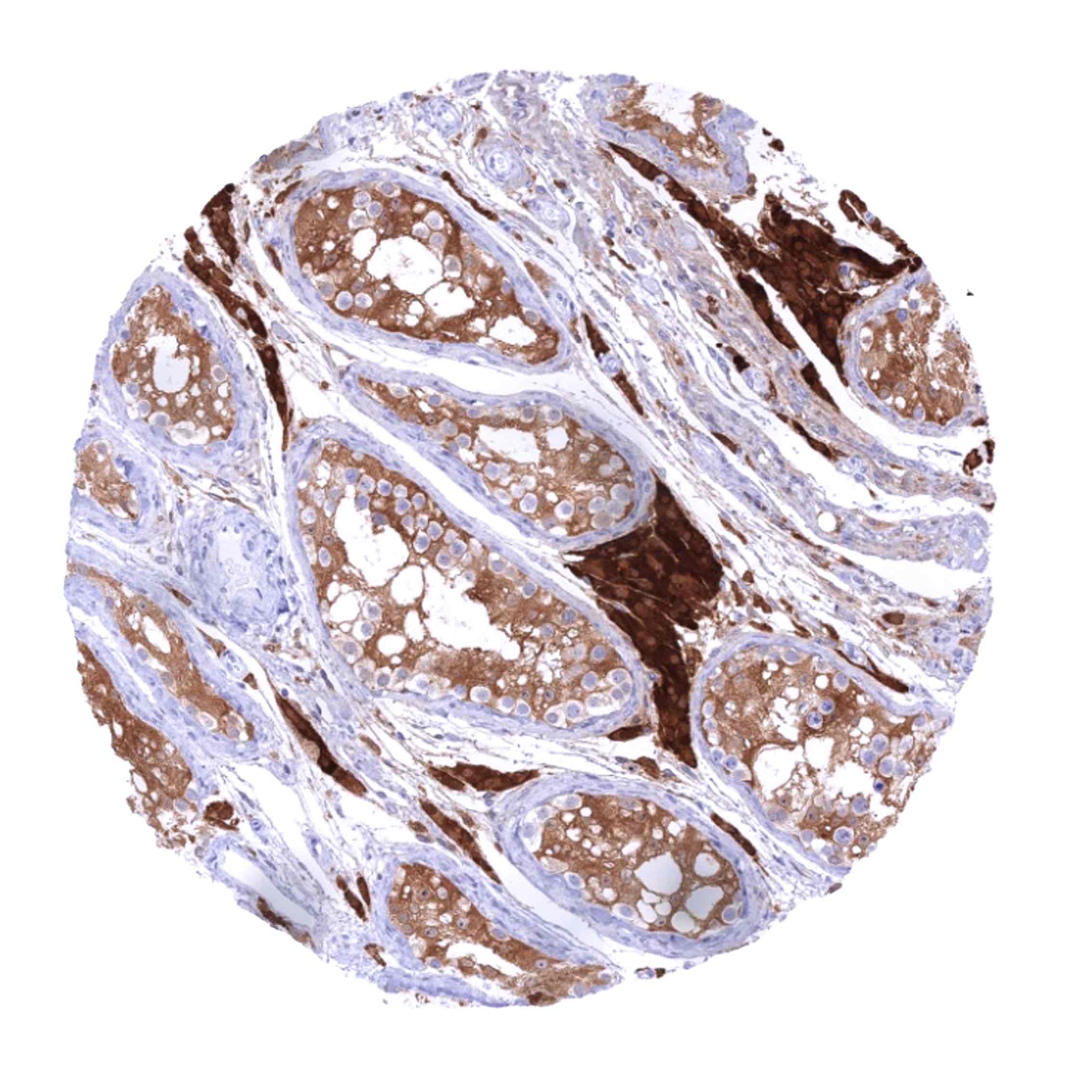
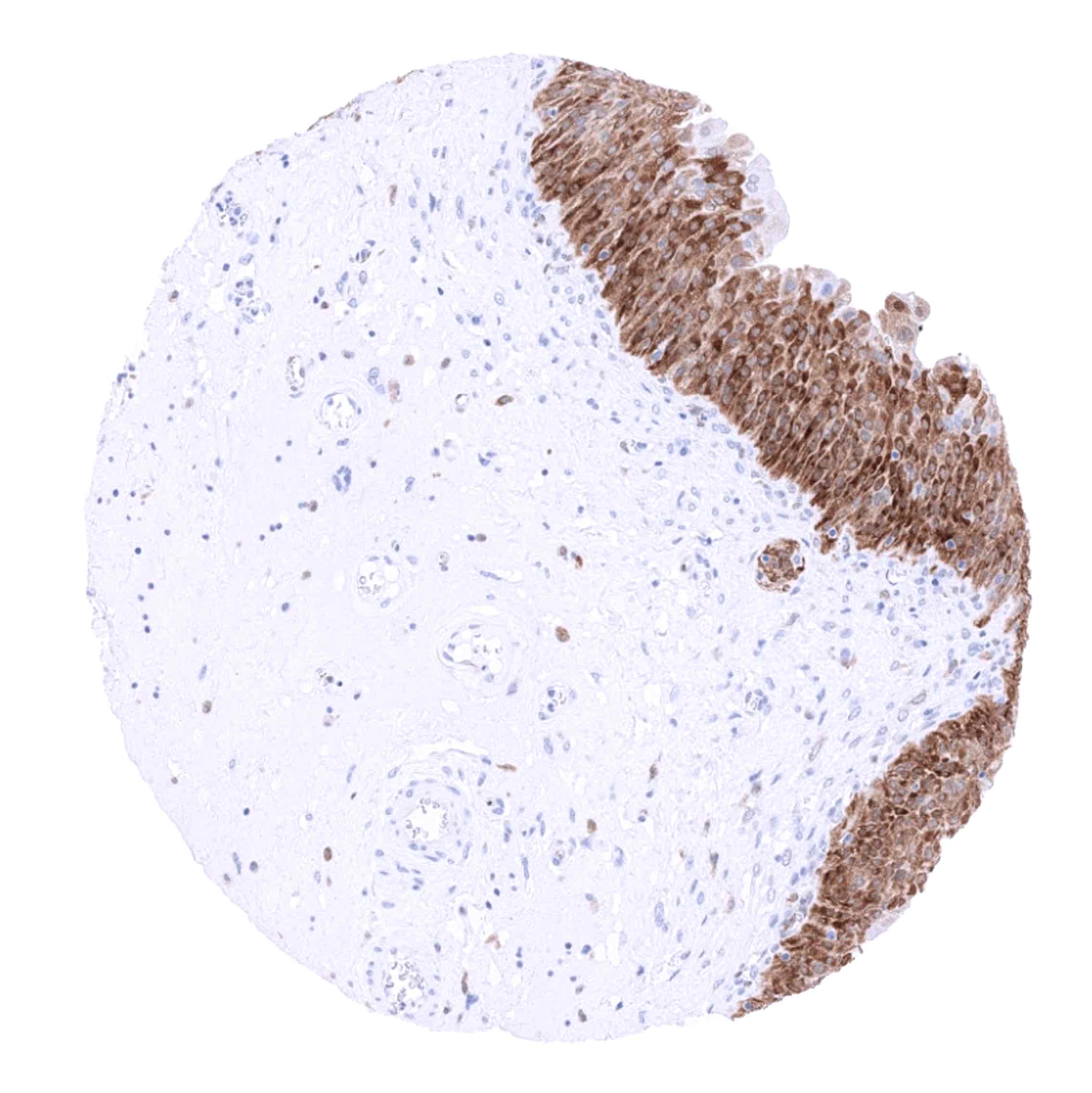
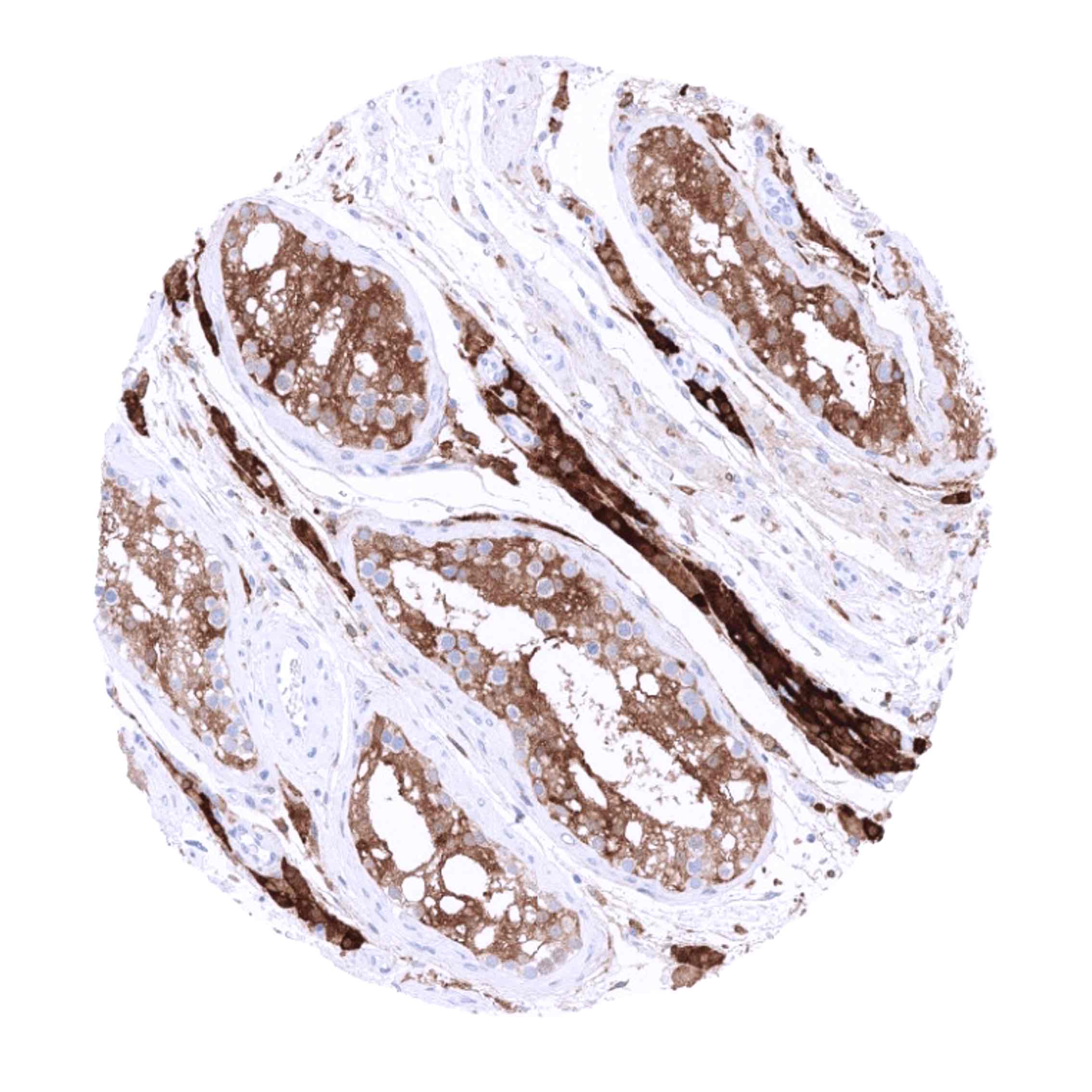
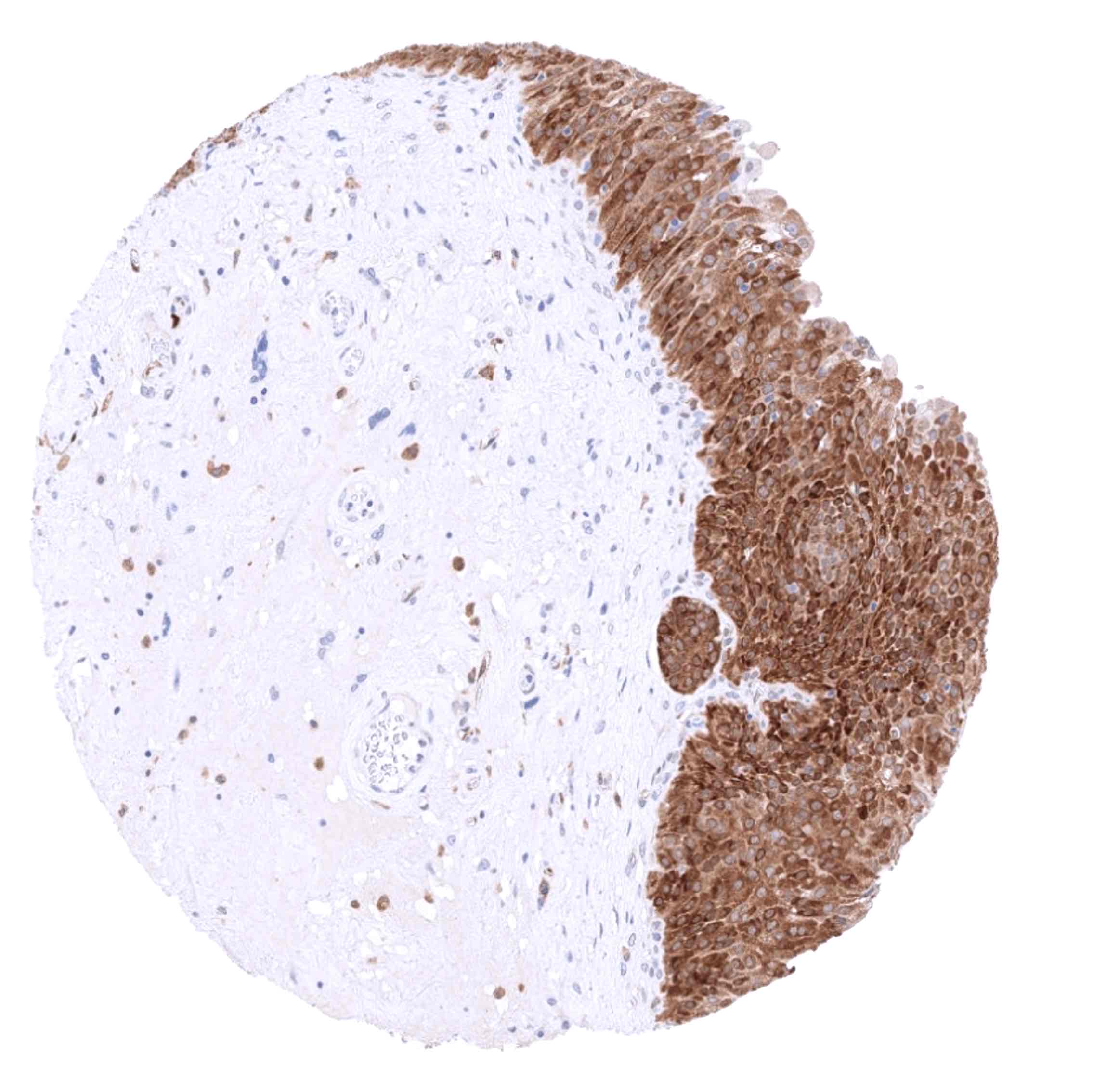
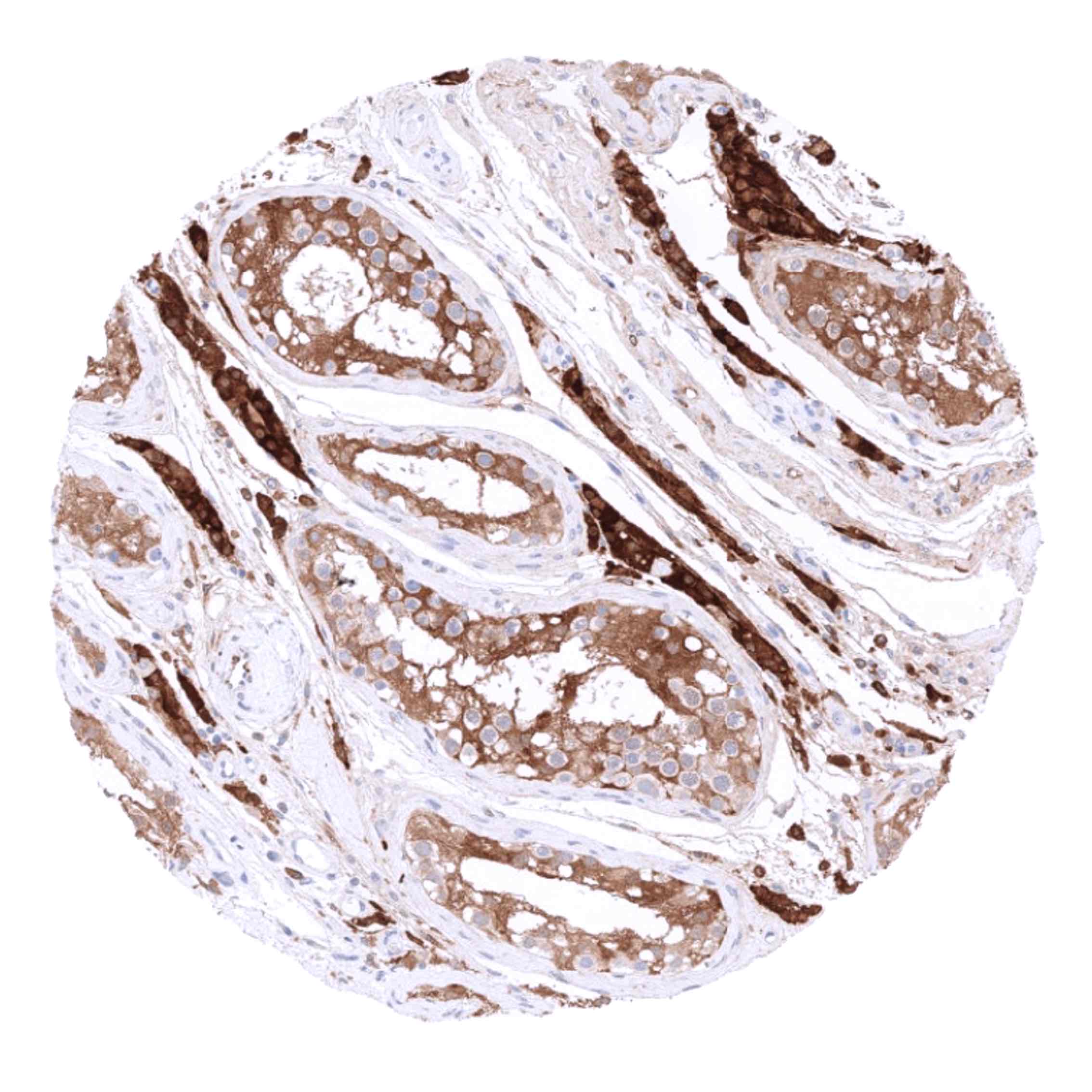
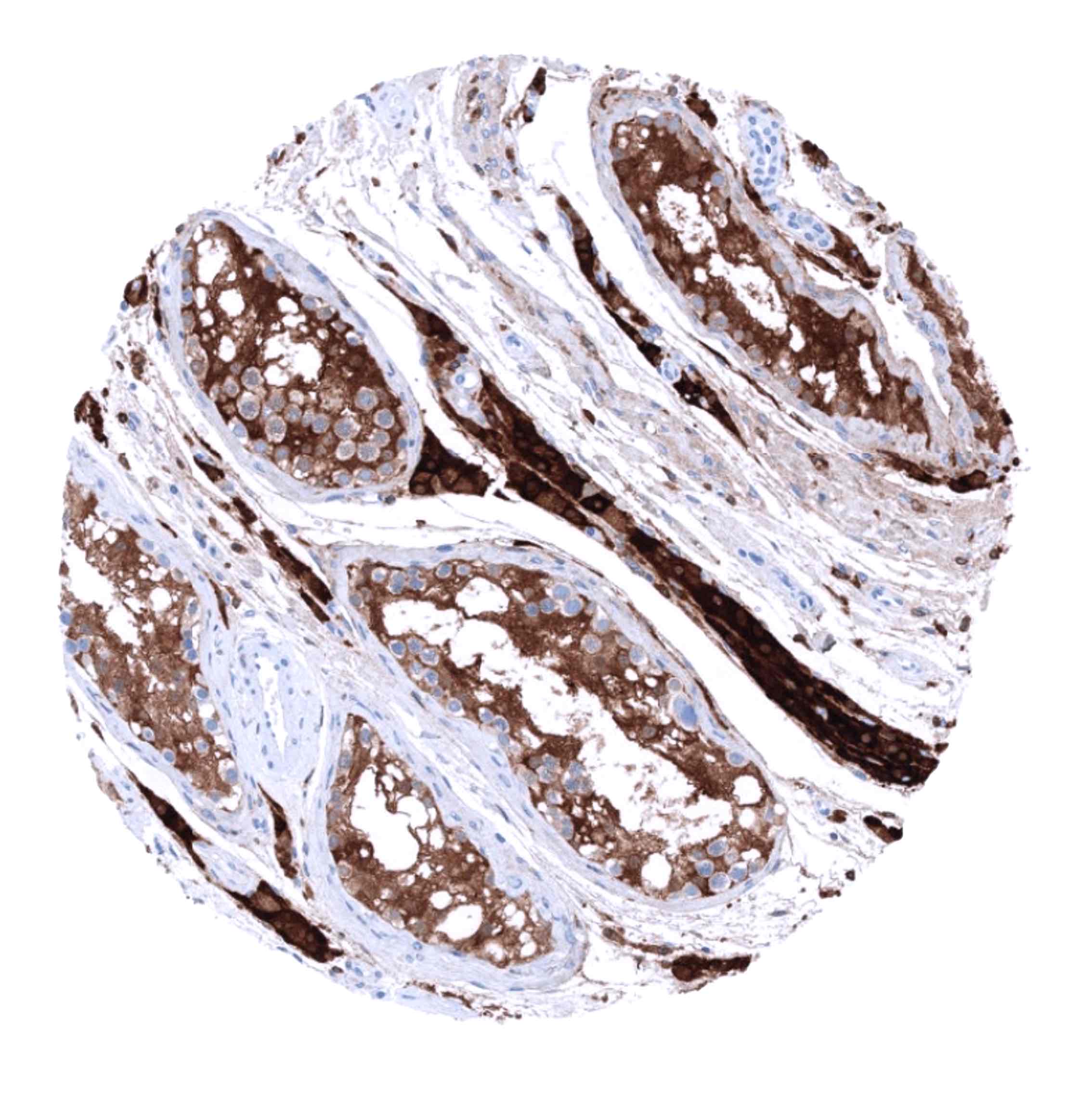
Genitourinary tract: GS staining is highly variable in urothelium. GS staining can be intense in all cells, completely absent, or limited to umbrella cells. The kidney is GS negative, but few distal tubuli or collecting ducts may stain positive. In the testis, staining is weak to moderate in Sertoli cells and strong in Leydig cells. In the epididymis, a strong staining occurs in most epithelial cells of the cauda while staining is weaker, only focal and not always seen in the corpus. Seminal vesicles show a variable positivity in a fraction of cells. The prostate is usually GS negative but a fraction of samples shows basal cell or atrophic gland staining.
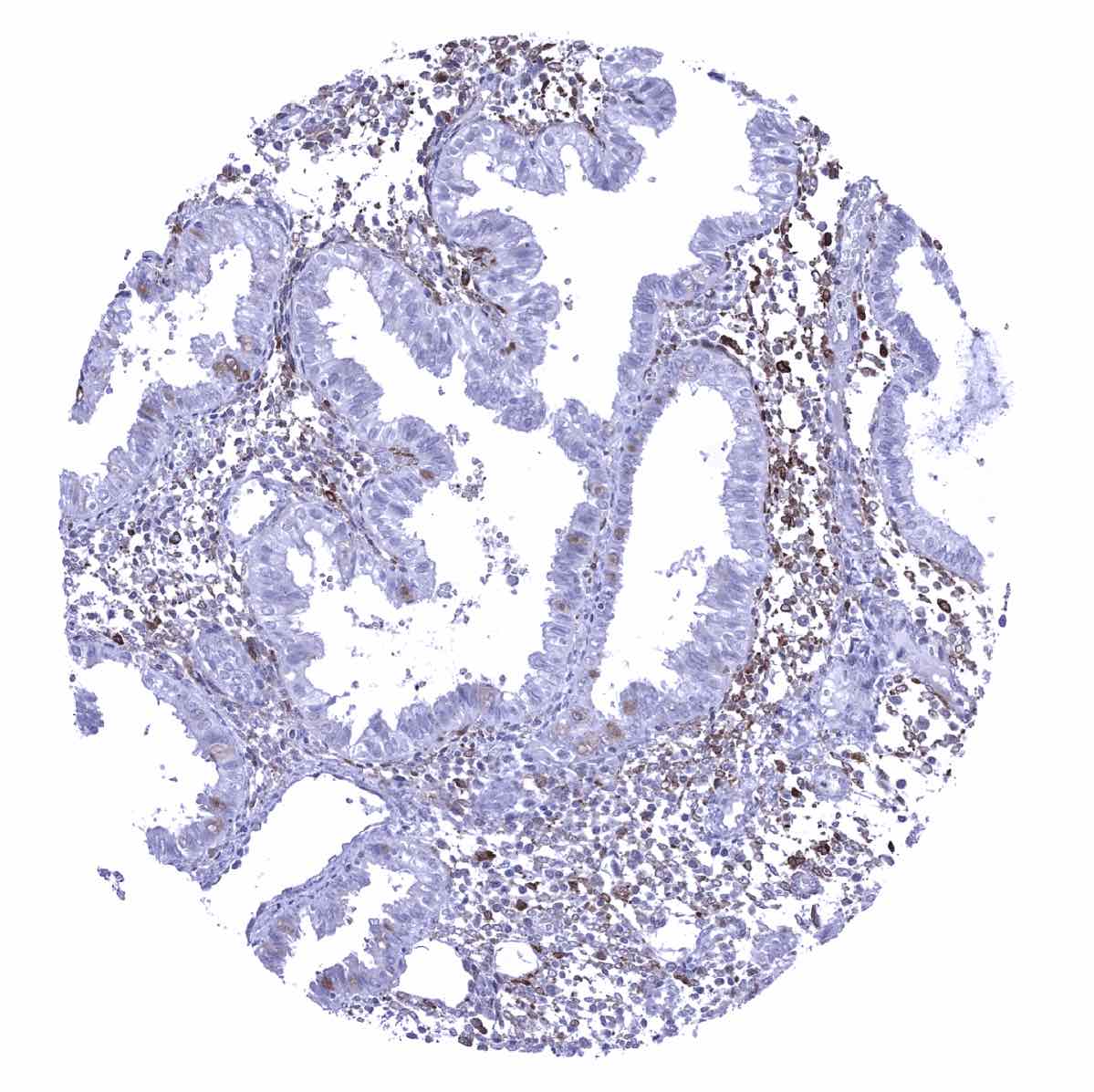
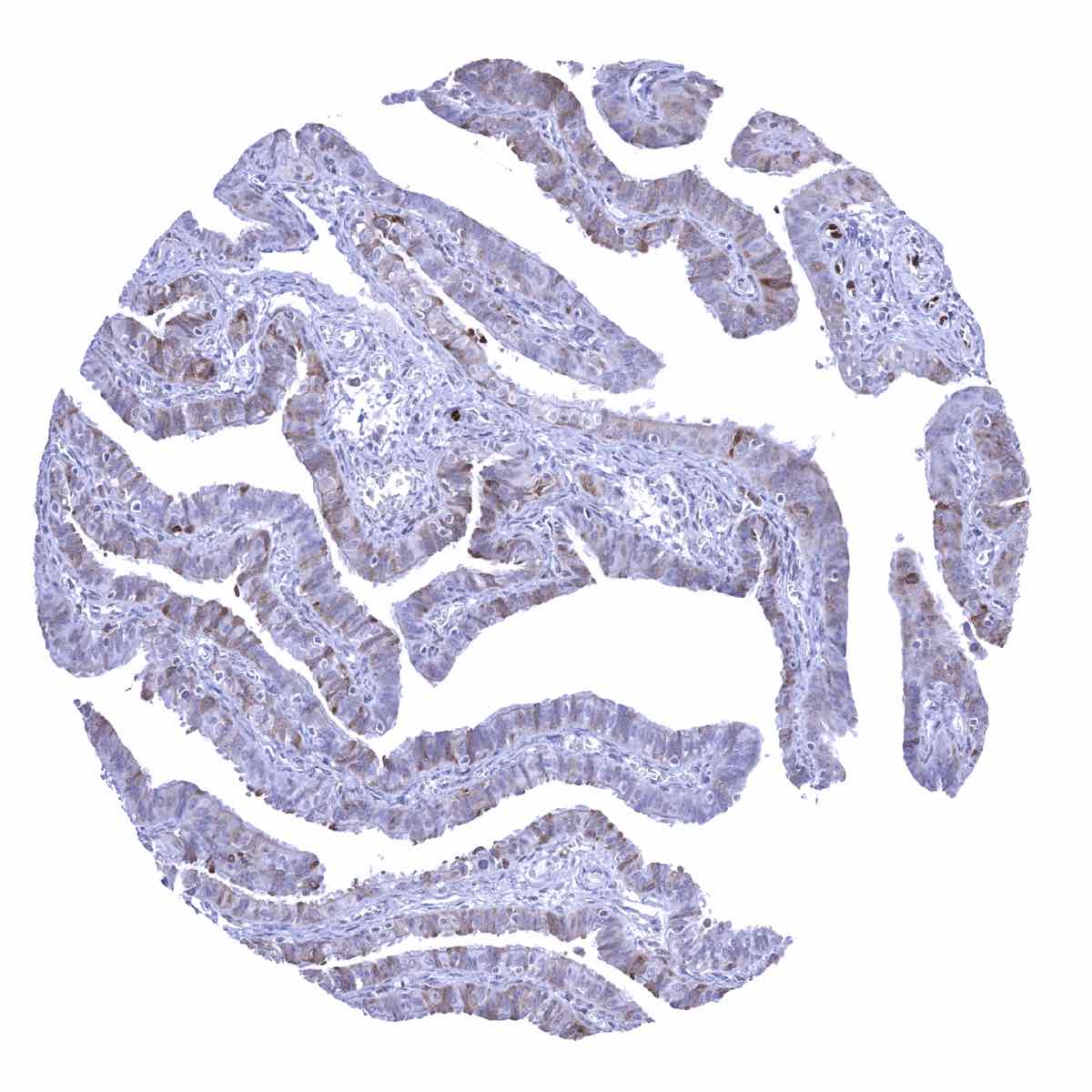
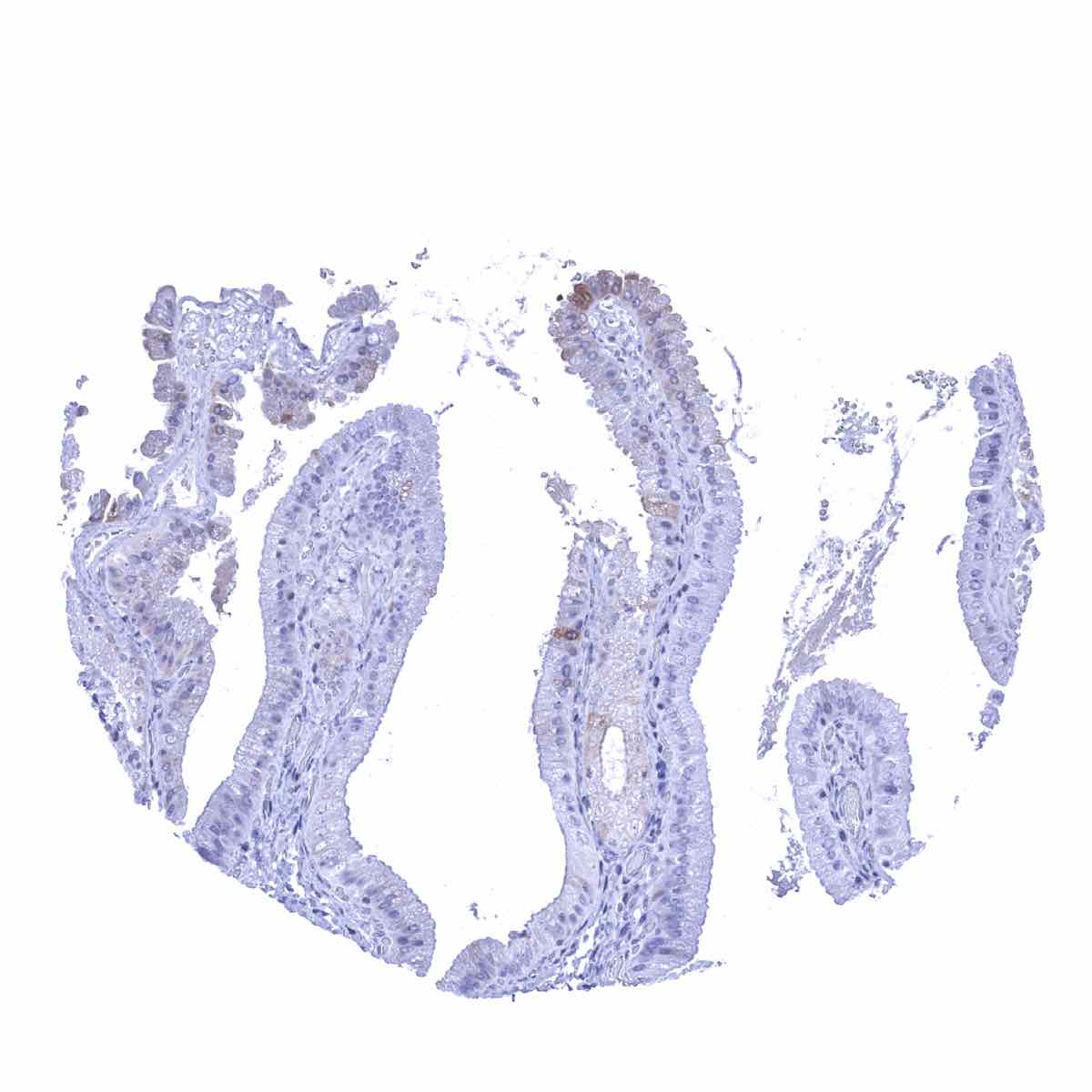
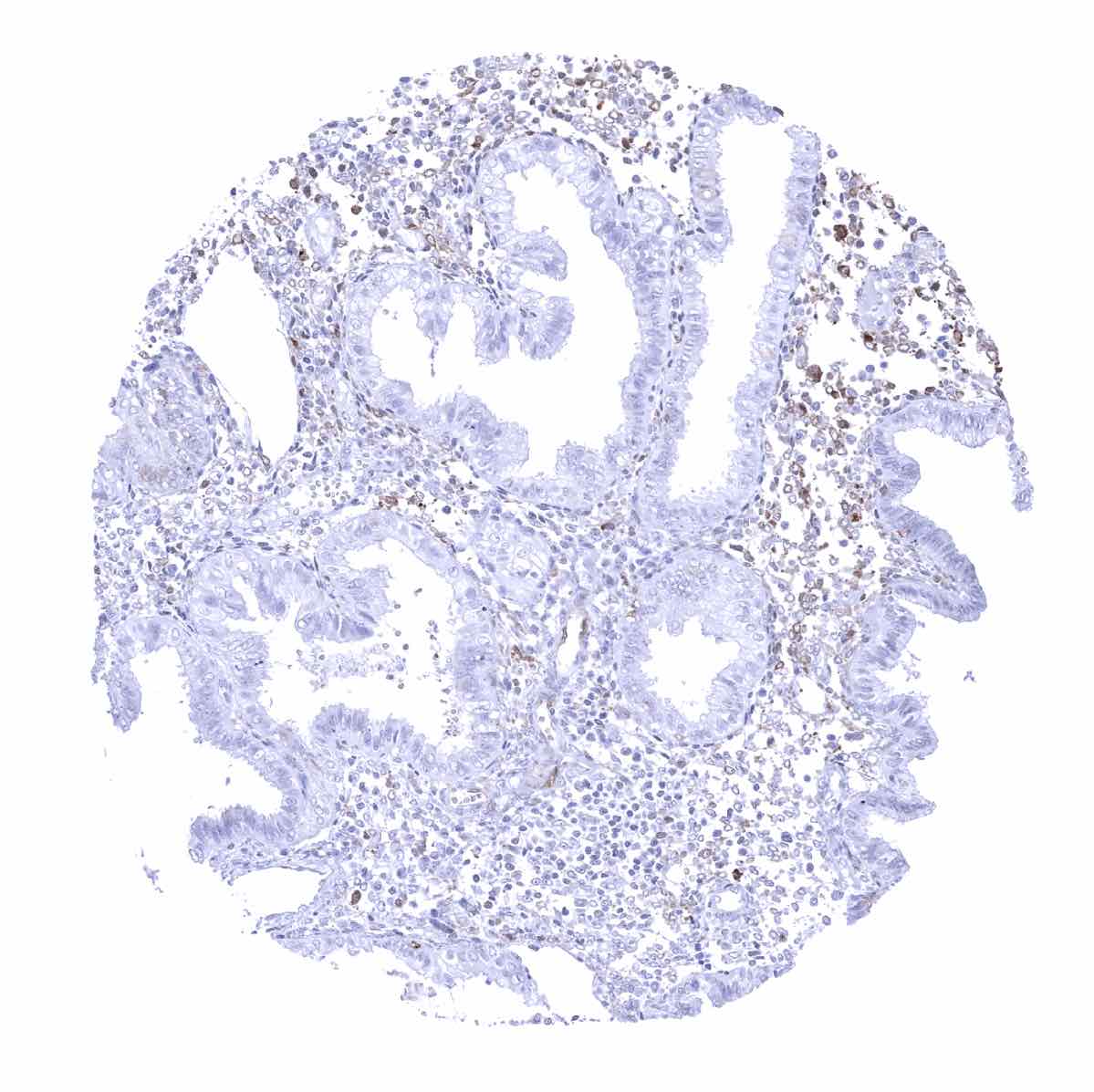
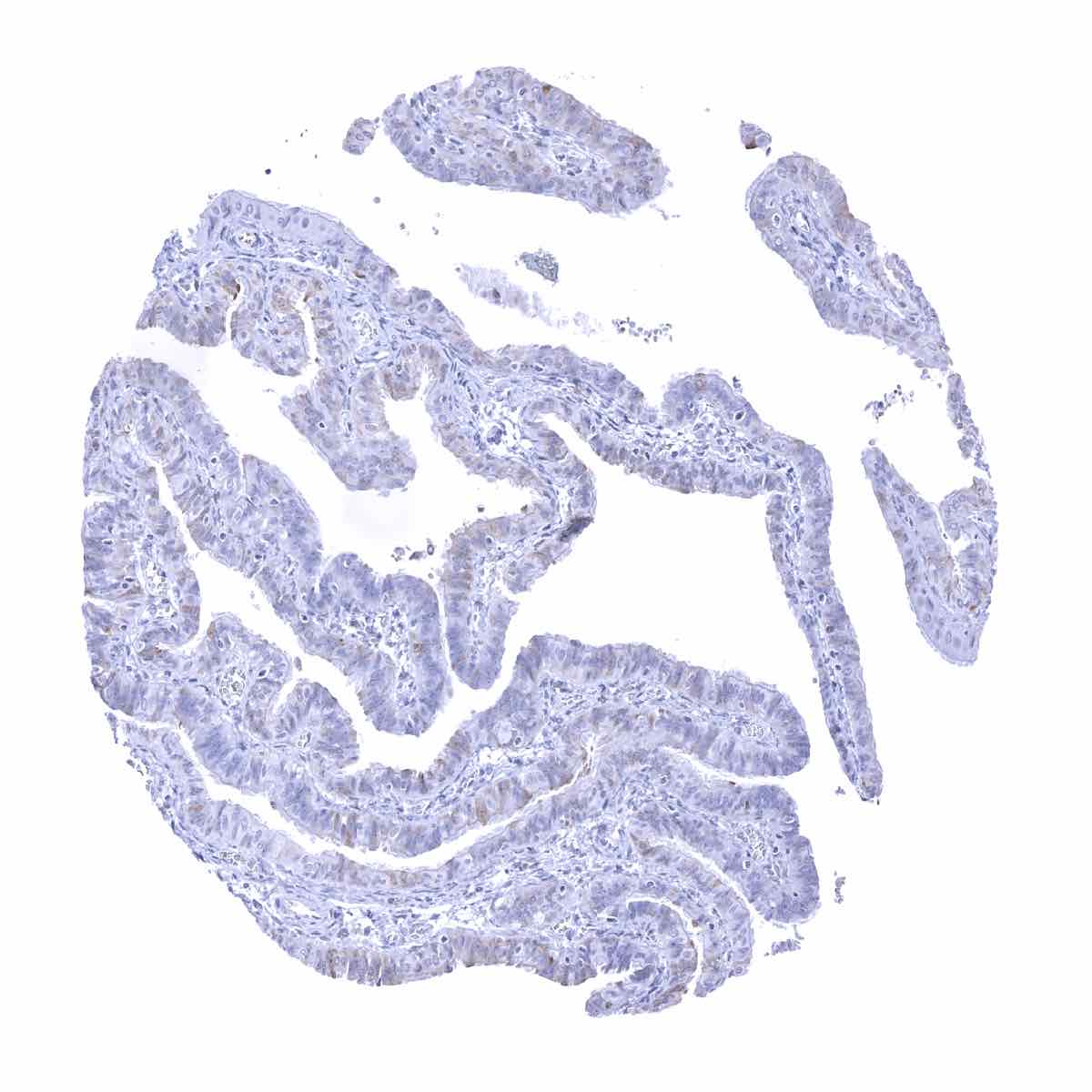
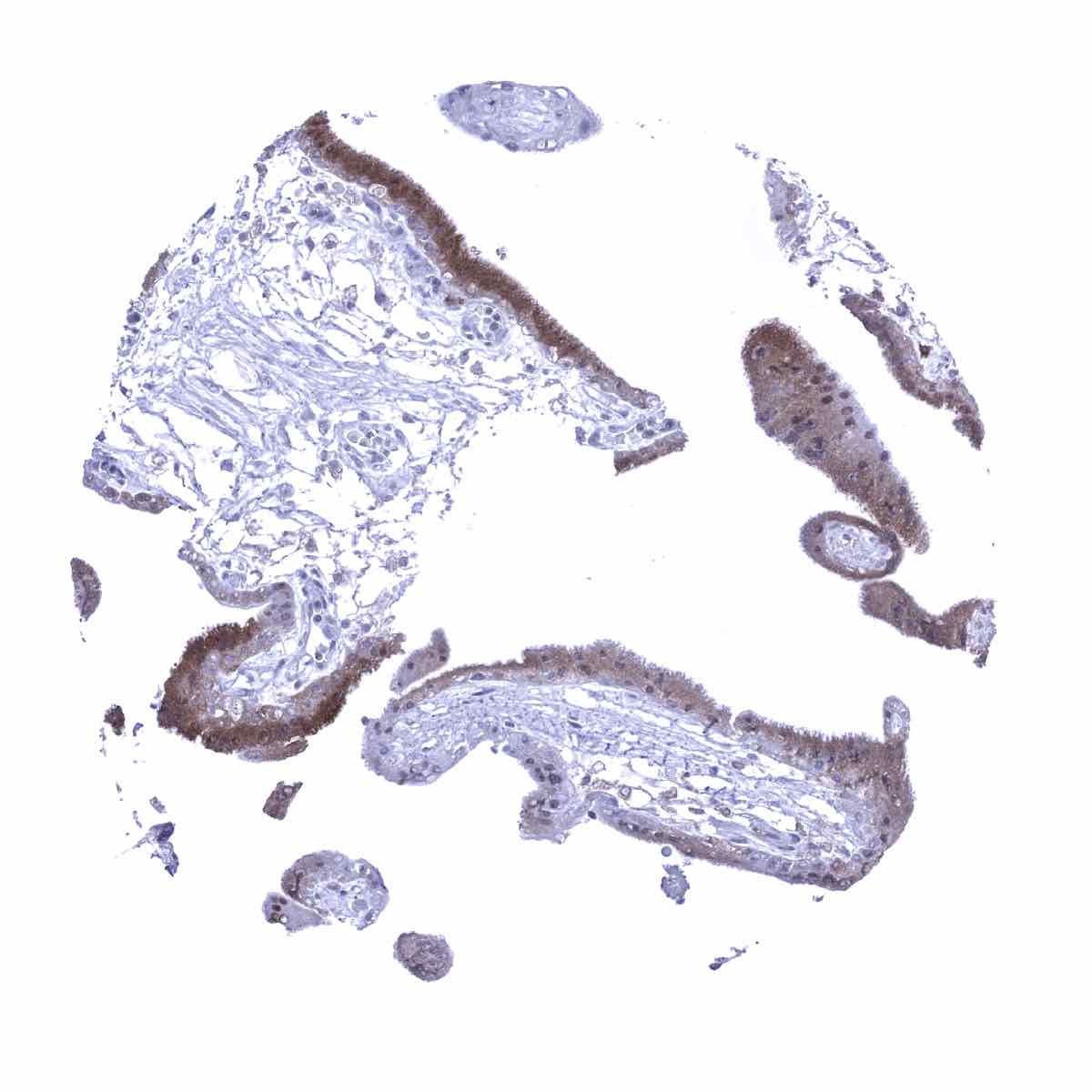
Female organs: Acinar cells of the breast may show a weak staining. In the endometrium staining is variable, predominates in stromal and inflammatory cells and is only focal and faint in epithelial cells. Staining may be more intense in the secretion than in the proliferation phase of the endometrium. A fraction of epithelial cells shows a weak to moderate staining in the fallopian tube. In the placenta, chorion and amnion cells are negative but trophoblast (early > mature) and stroma cells can show a variable positivity. GS staining is very intense in decidua cells. In the ovary, a variable staining intensity is seen in cells of the corpus luteum (mosaic pattern) and a weak to moderate staining occurs in theca and granulosa cells.
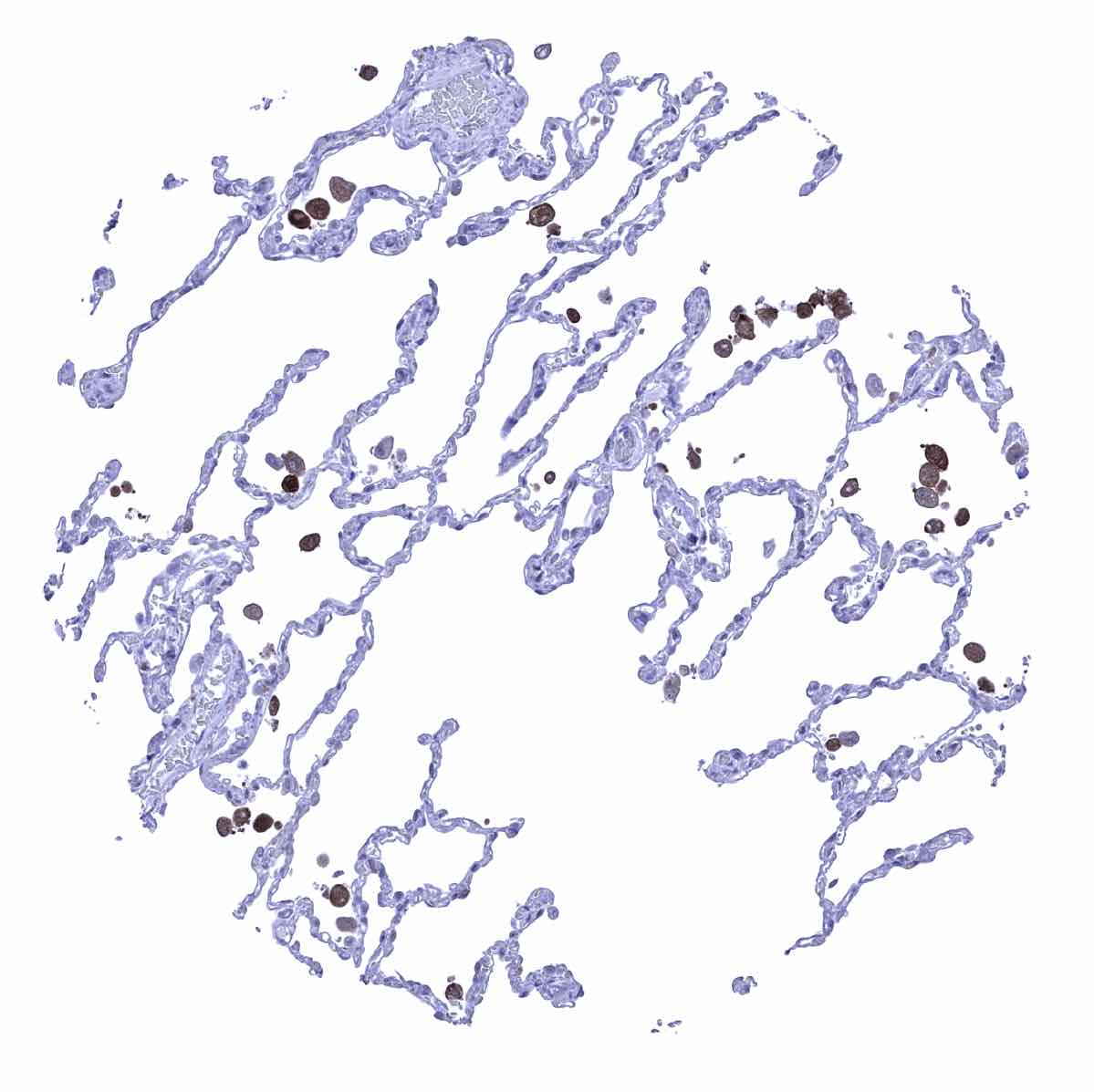
Respiratory tract: A fraction of (mostly) non-ciliated cells of the respiratory epithelium show a moderate to strong staining. In the lung, staining is usually limited to macrophages.
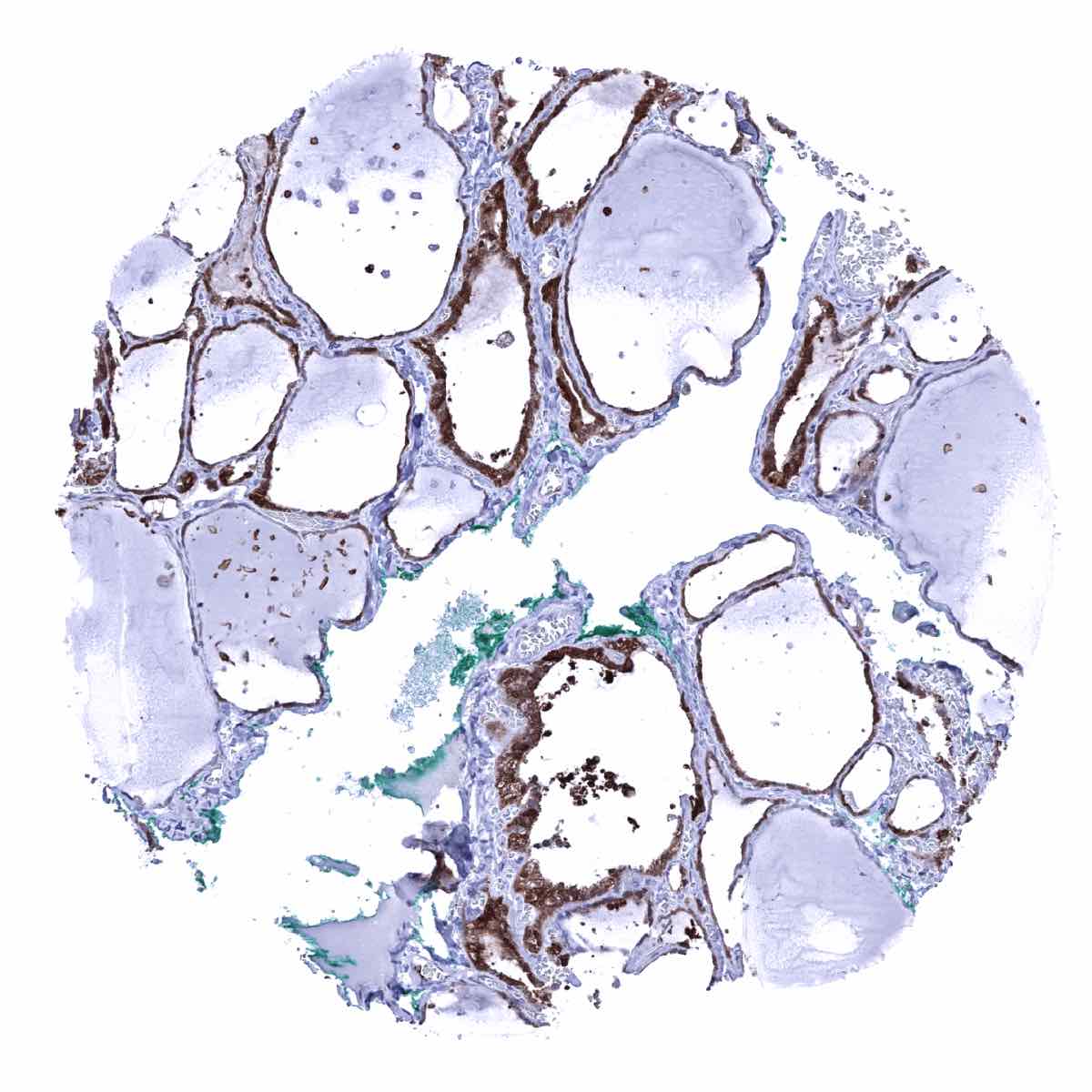
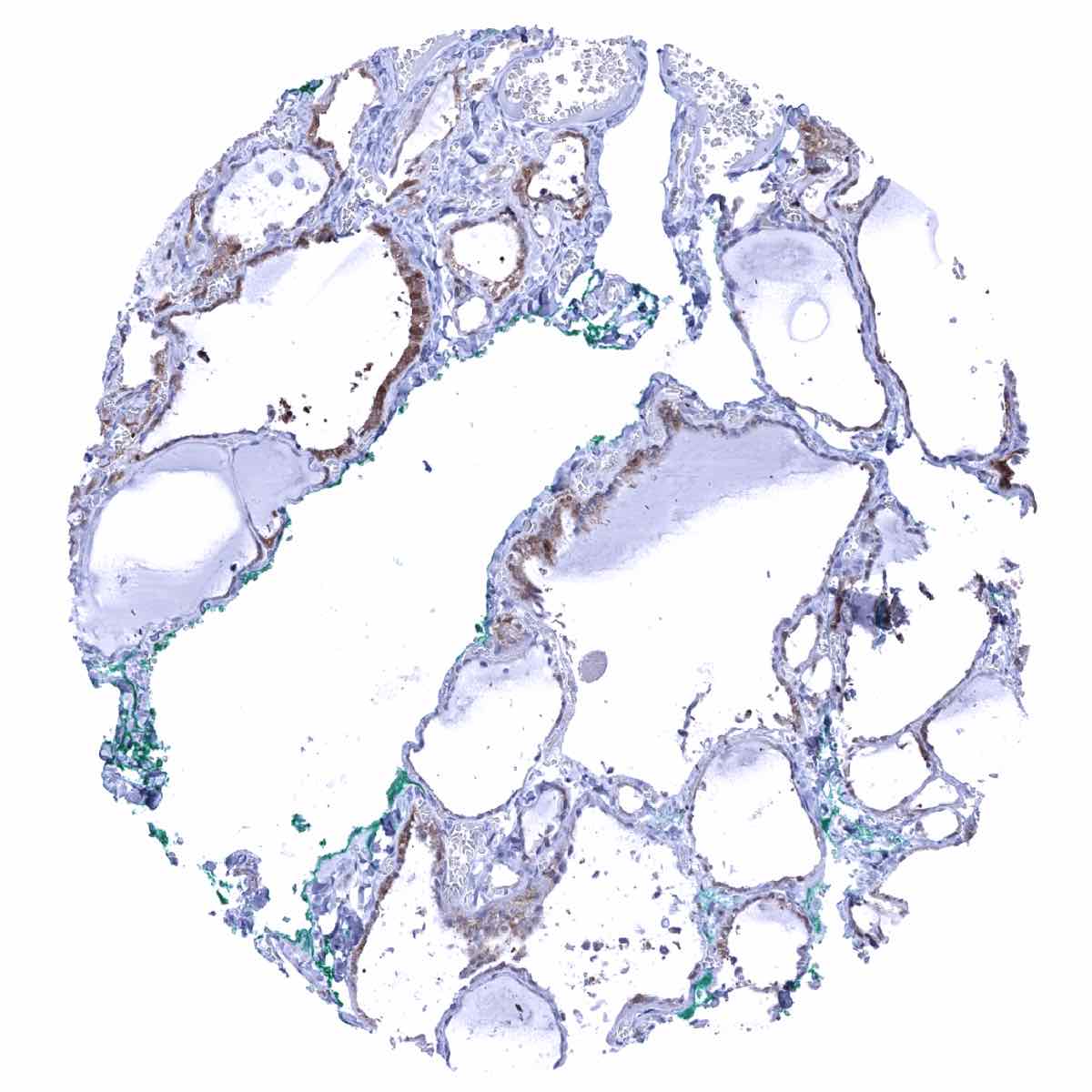
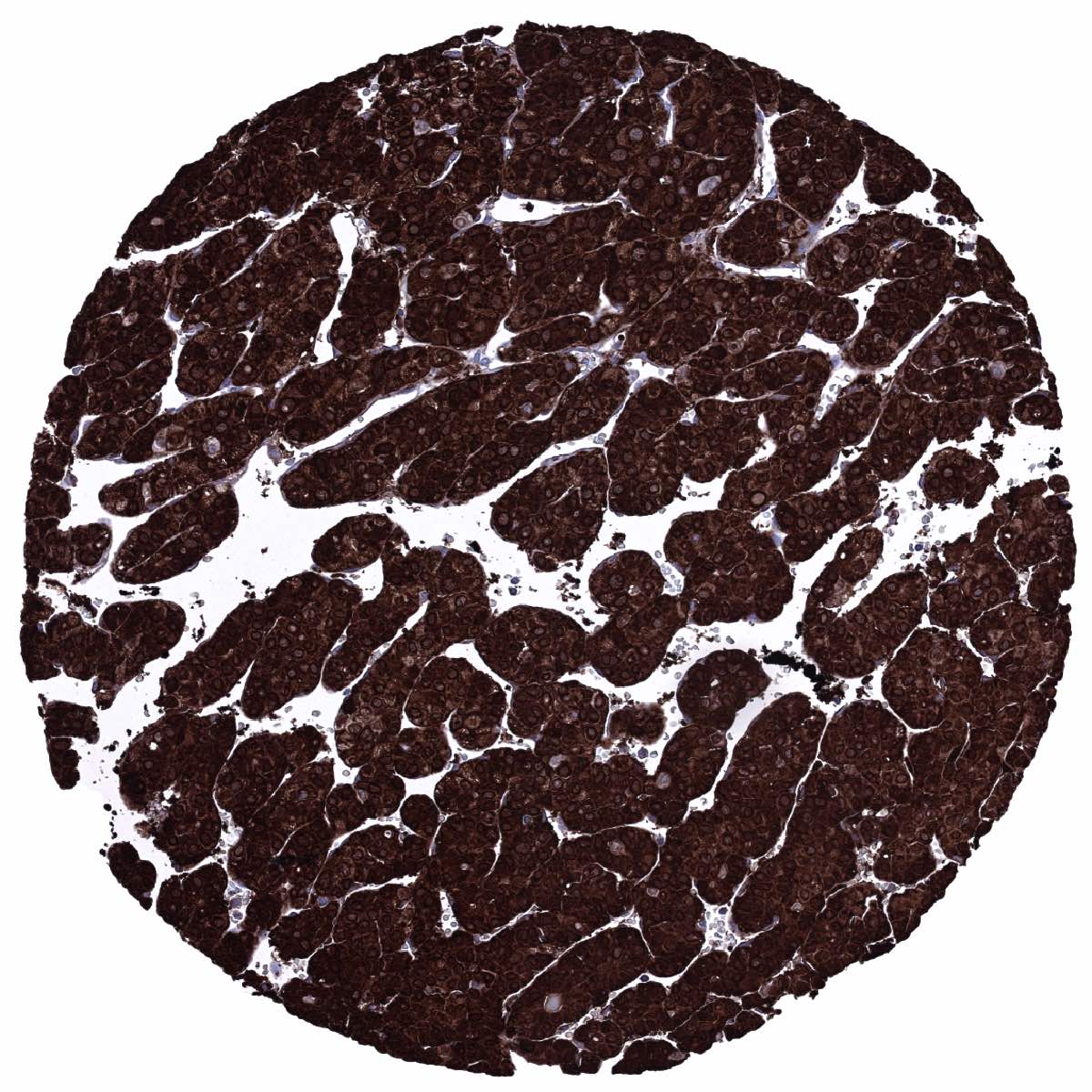
Endocrine organs: GS staining occurs in follicle cells of the thyroid (strong), a fraction of adrenal cells (variable intensity), and can also be seen in few cells of the adenohypophysis (weak to moderate). Staining is largely absent in the parathyroid gland.
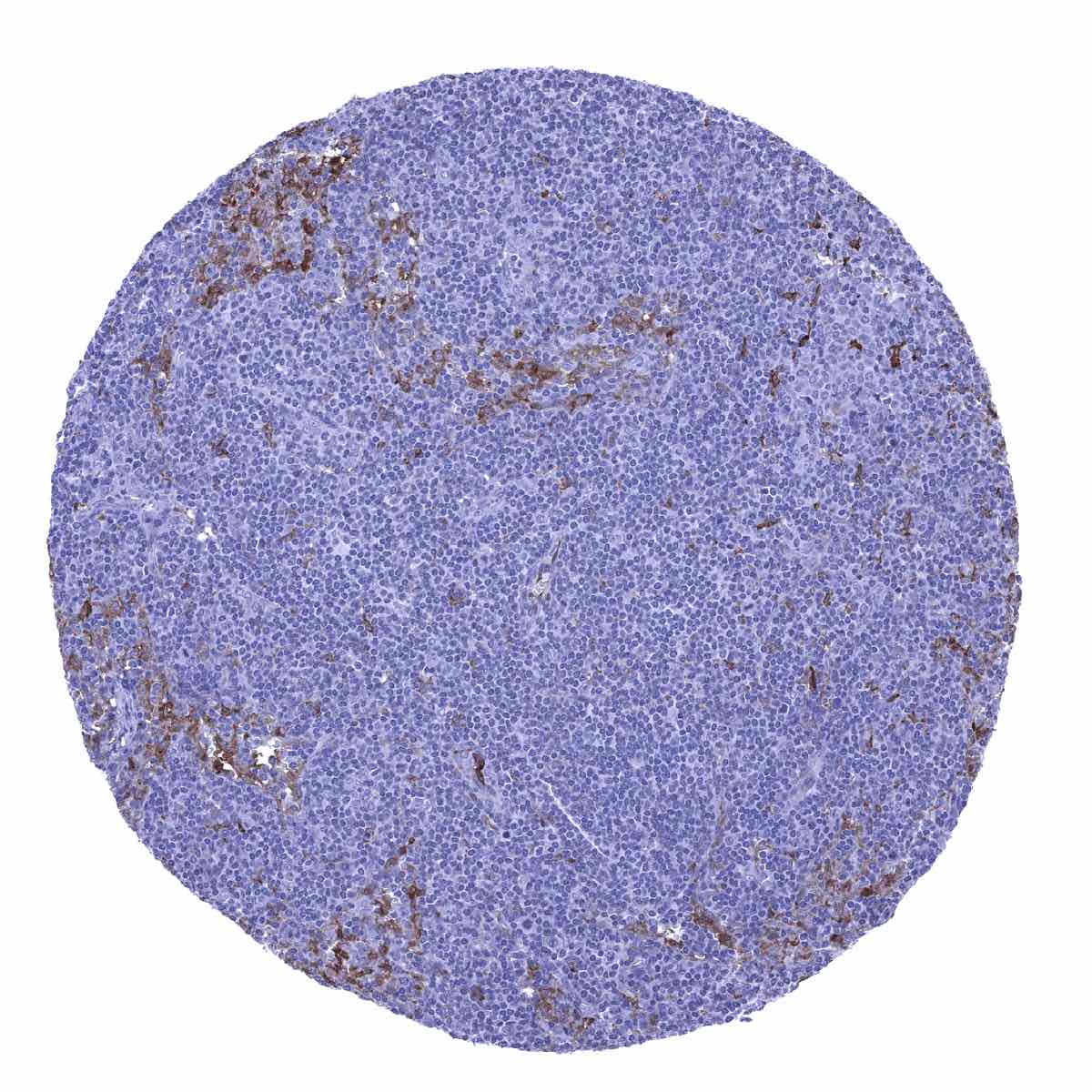
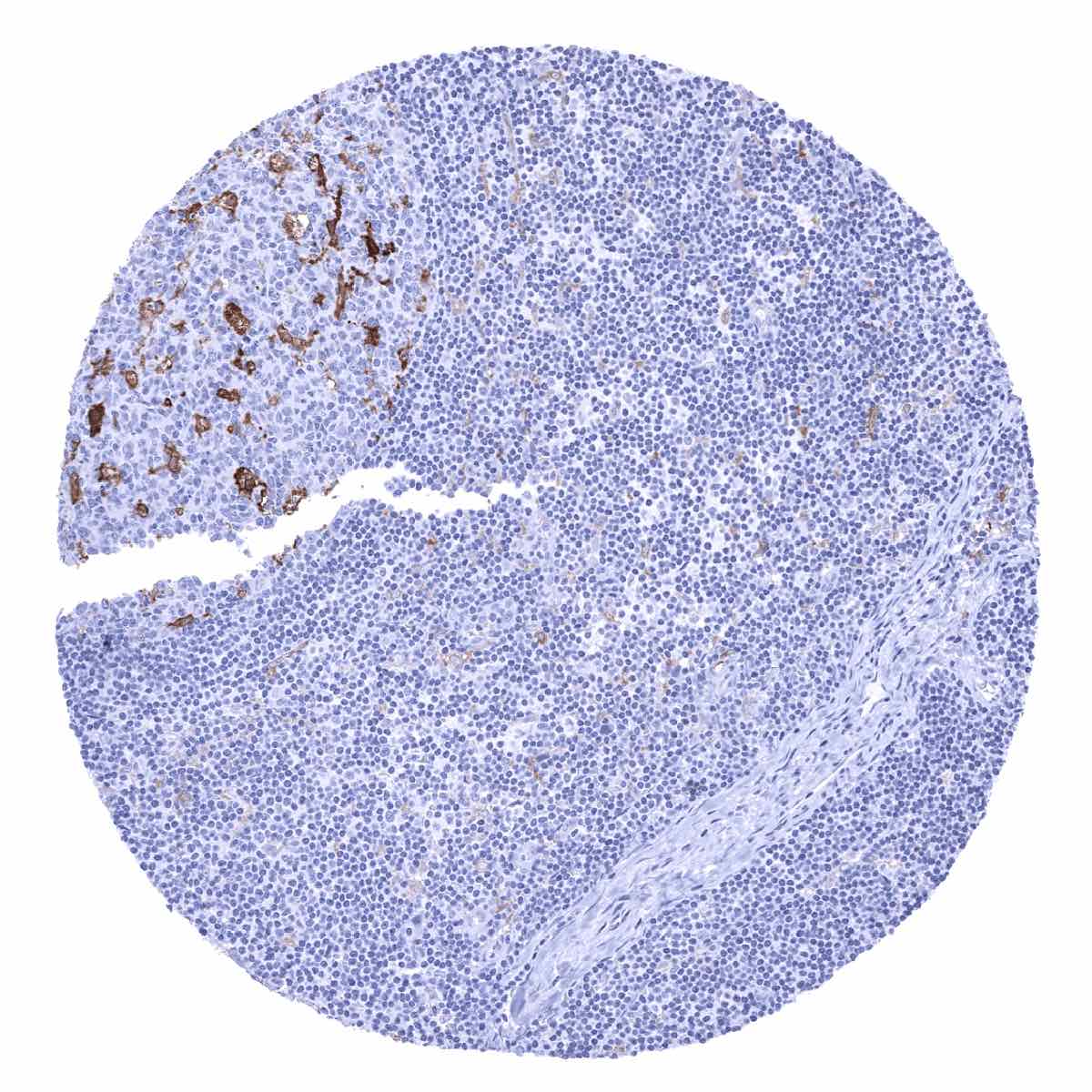
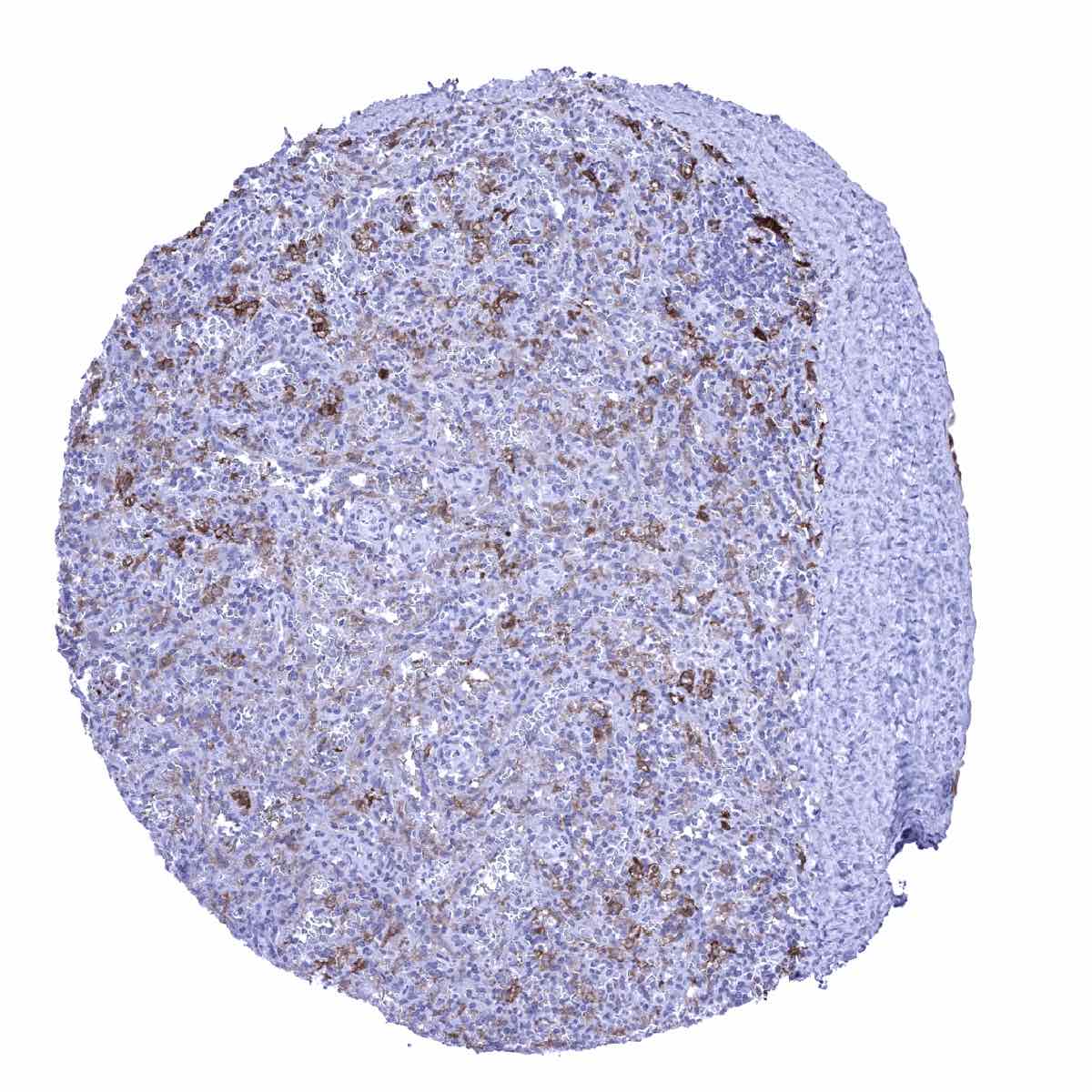
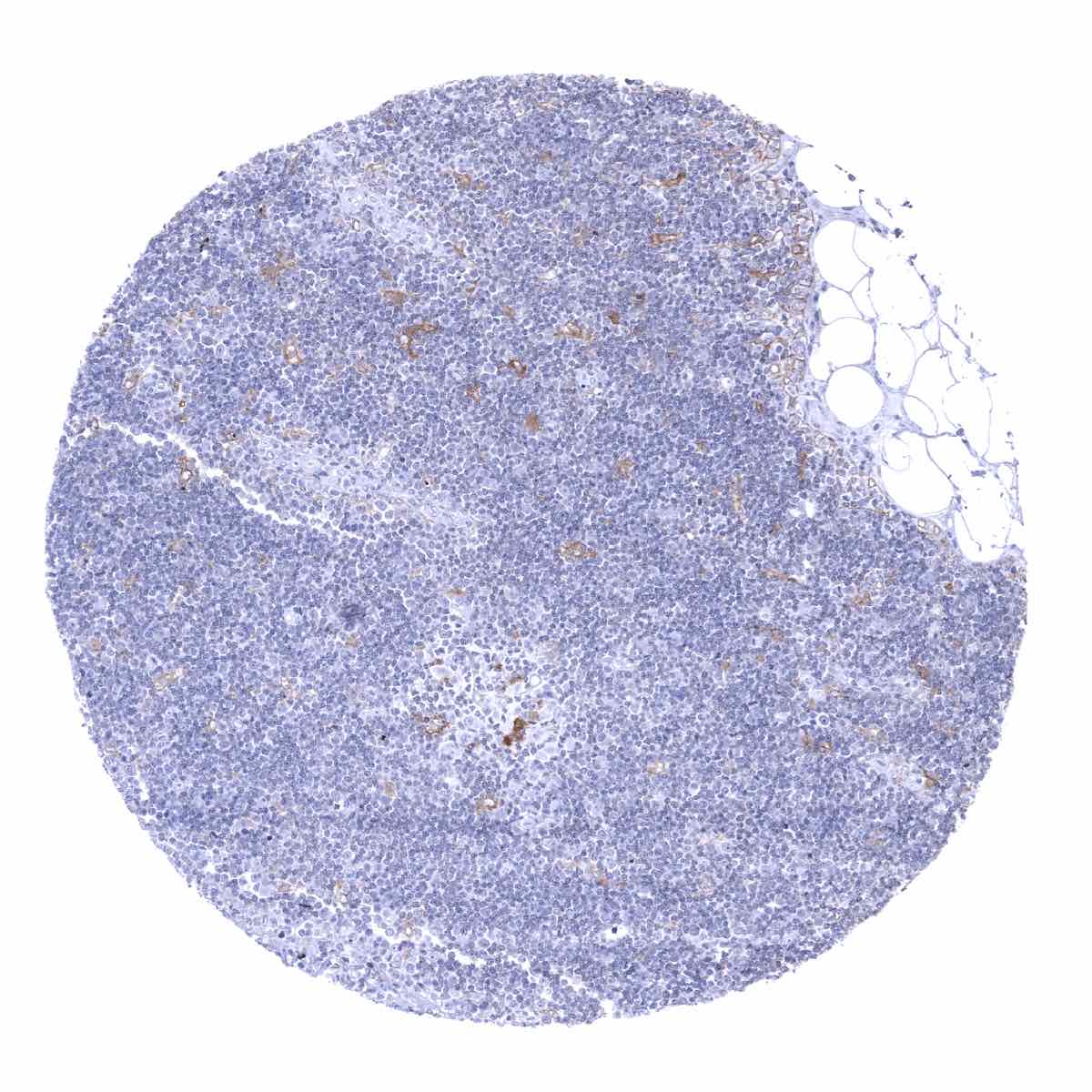
Lymphatic tissues and bone marrow: Dendritic cells in germinal centres and other macrophages/histiocytes as well as granulocytes show GS positivity of variable intensity.
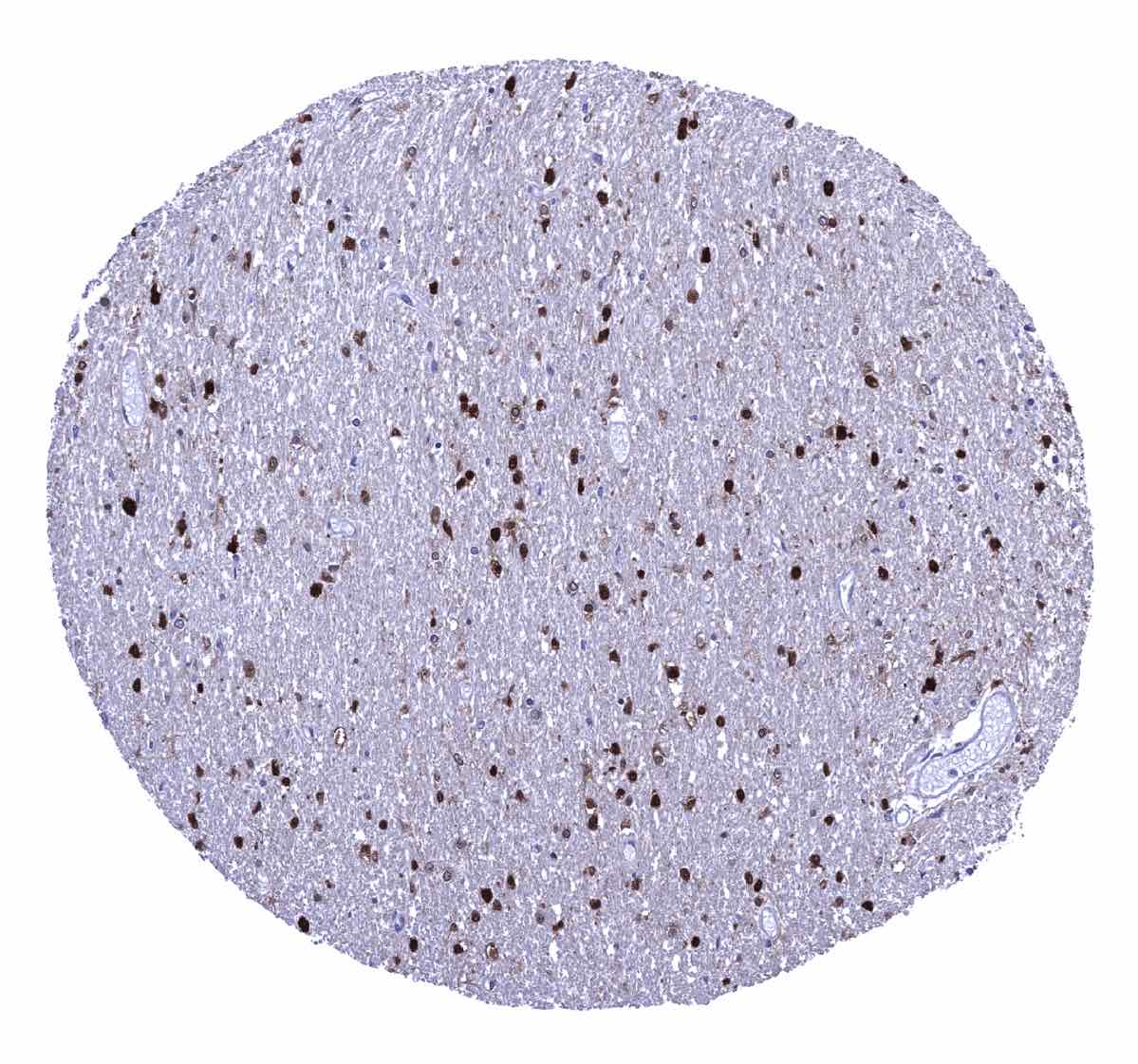
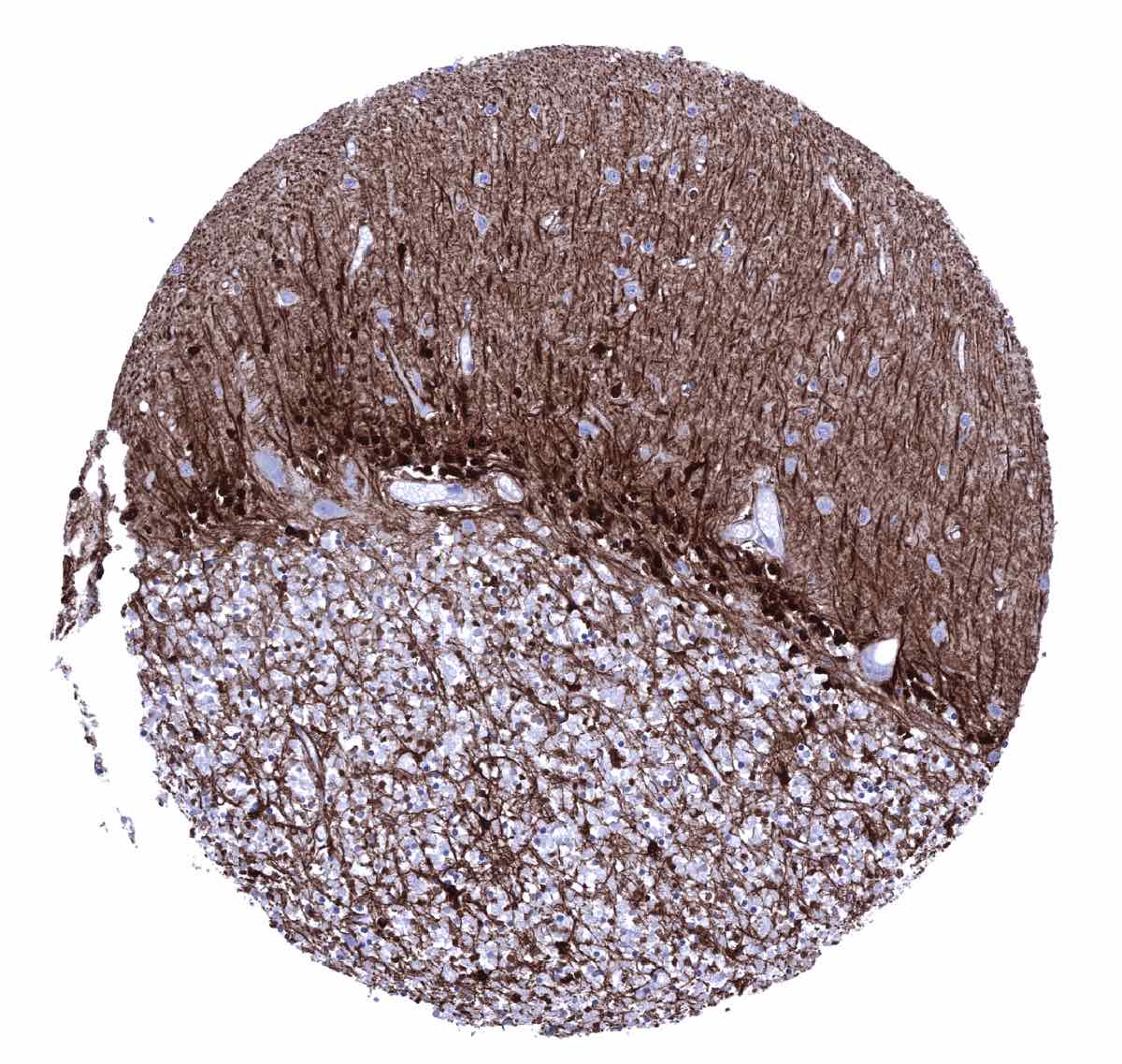
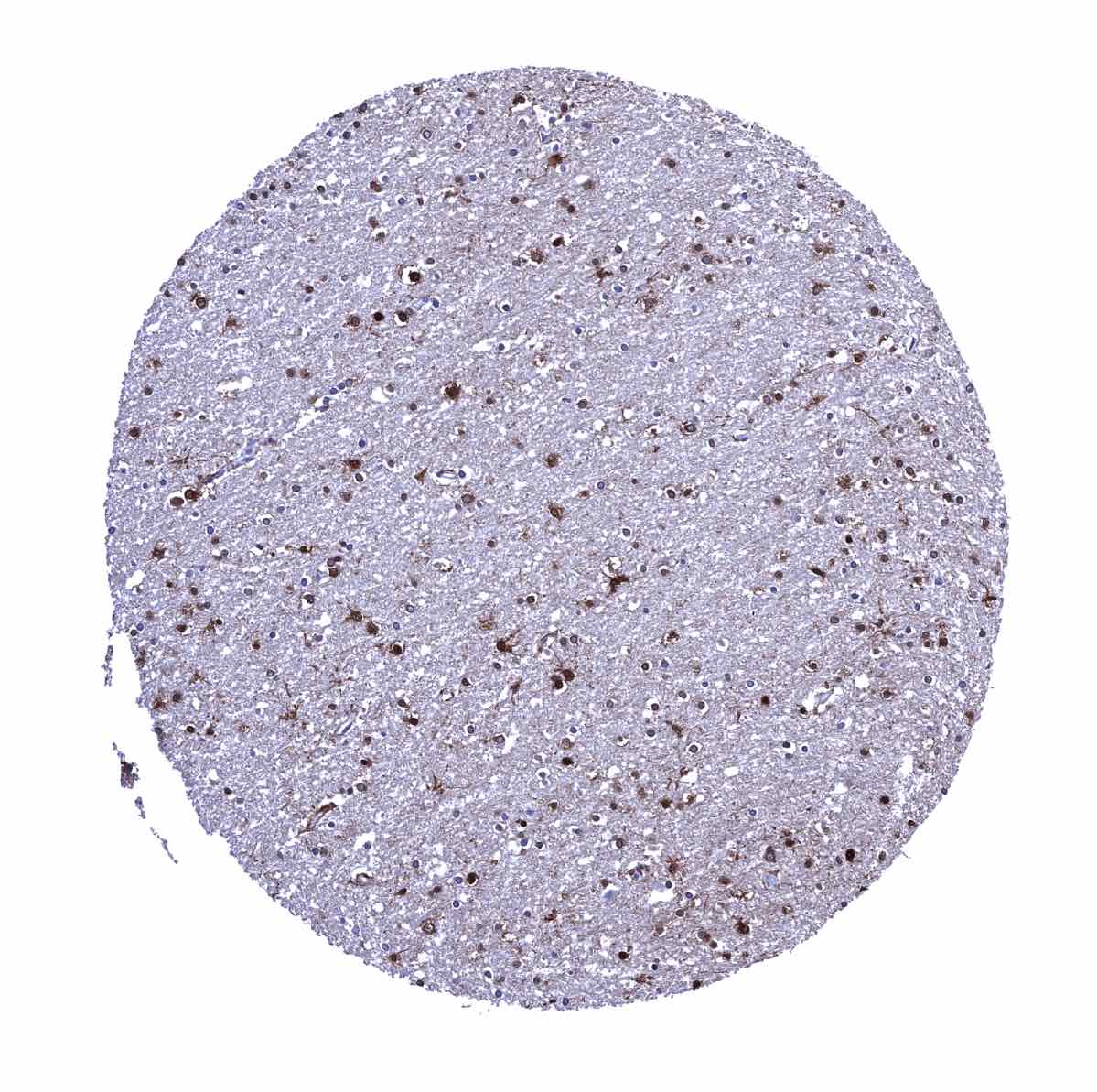
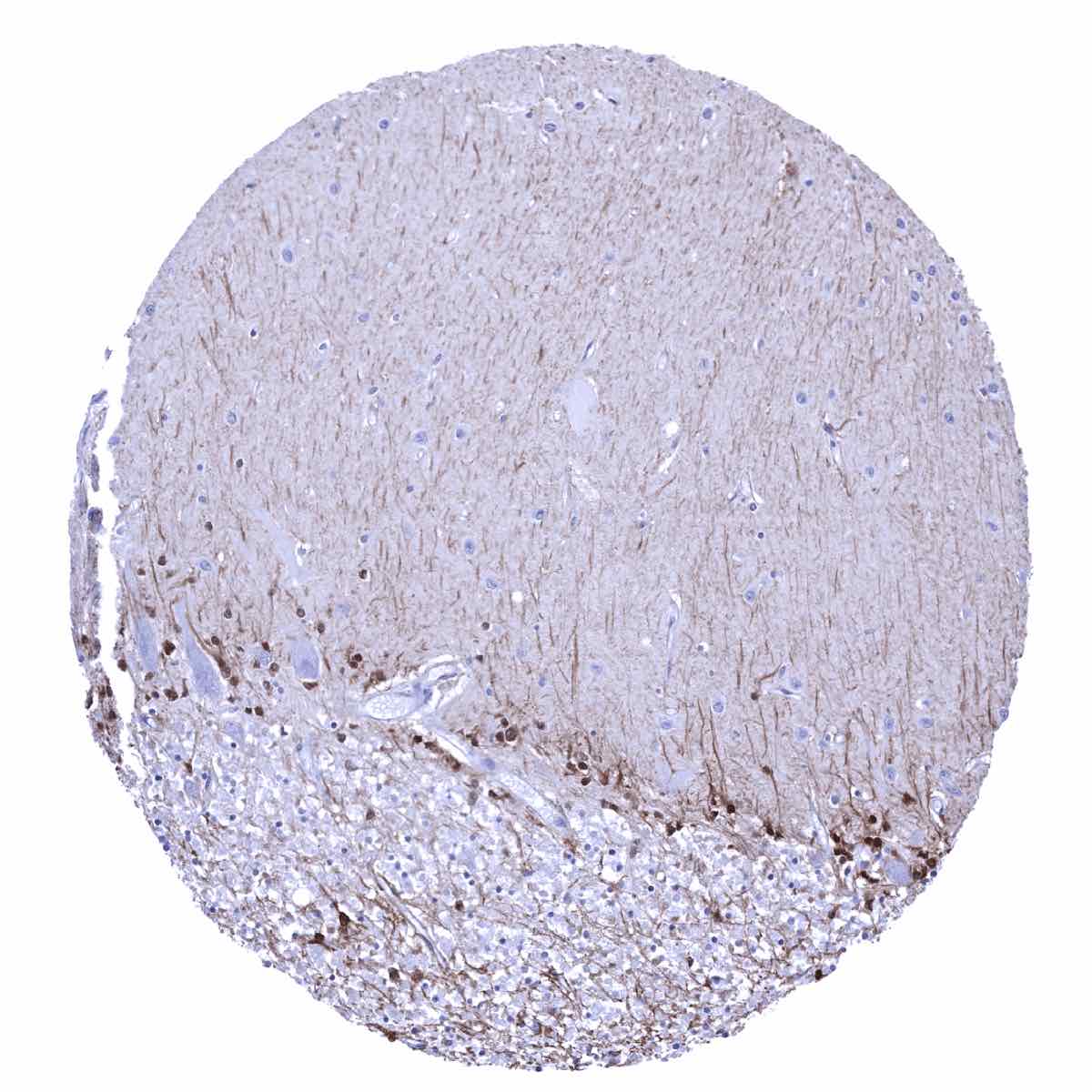
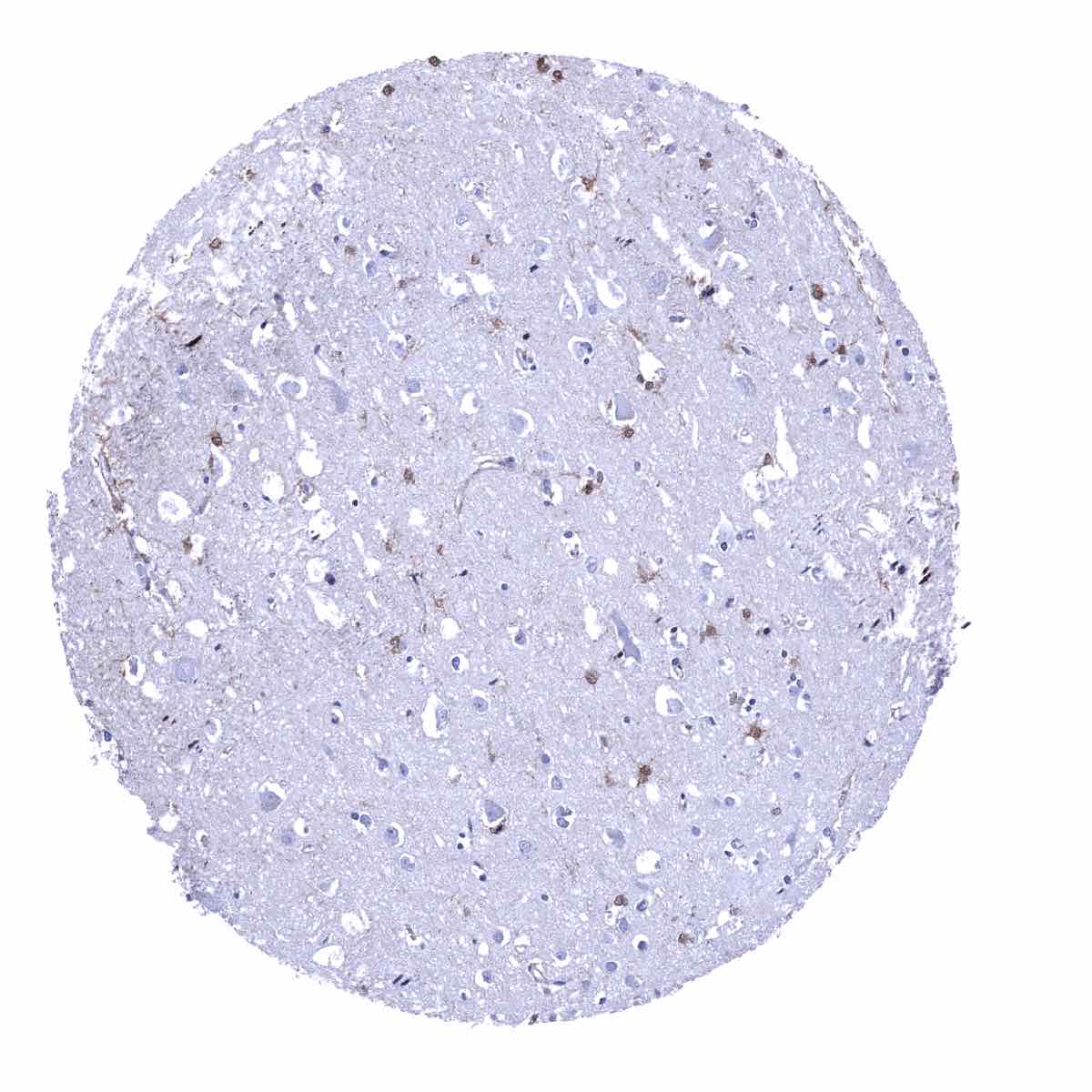
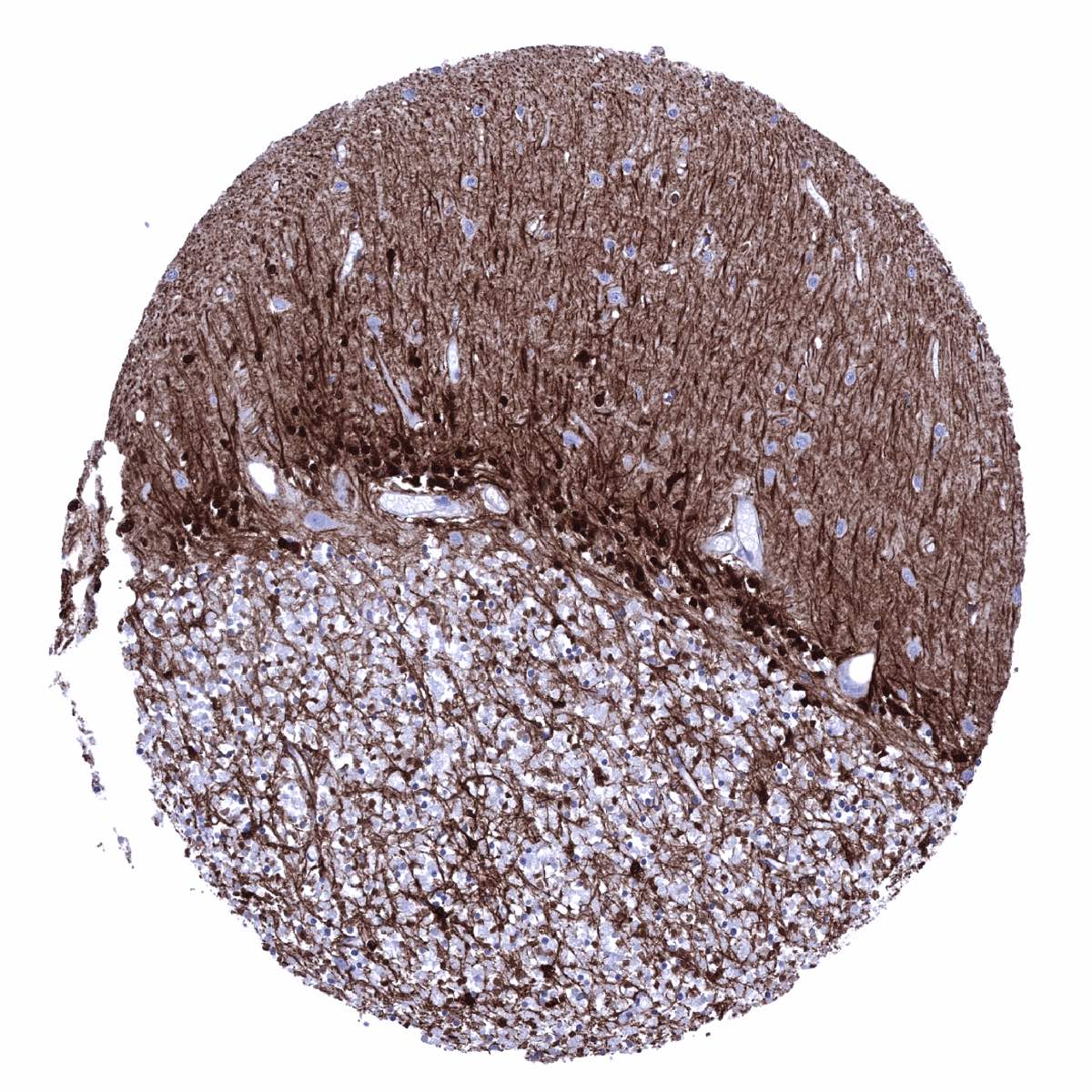
Brain: An intense positivity occurs in all glia cells and in associated fibres. Neurons and Purkinje are GS negative.
These findings are largely consistent with the RNA and protein data described in the Human Protein Atlas (Tissue expression Glutamine Synthetase)
Positive control = Liver: A strong GS staining should be seen of centrilobular hepatocytes while staining is weak to moderate in Kupffer cells.
Negative control = Liver: Periportal hepatocytes must be GS negative in the normal liver.

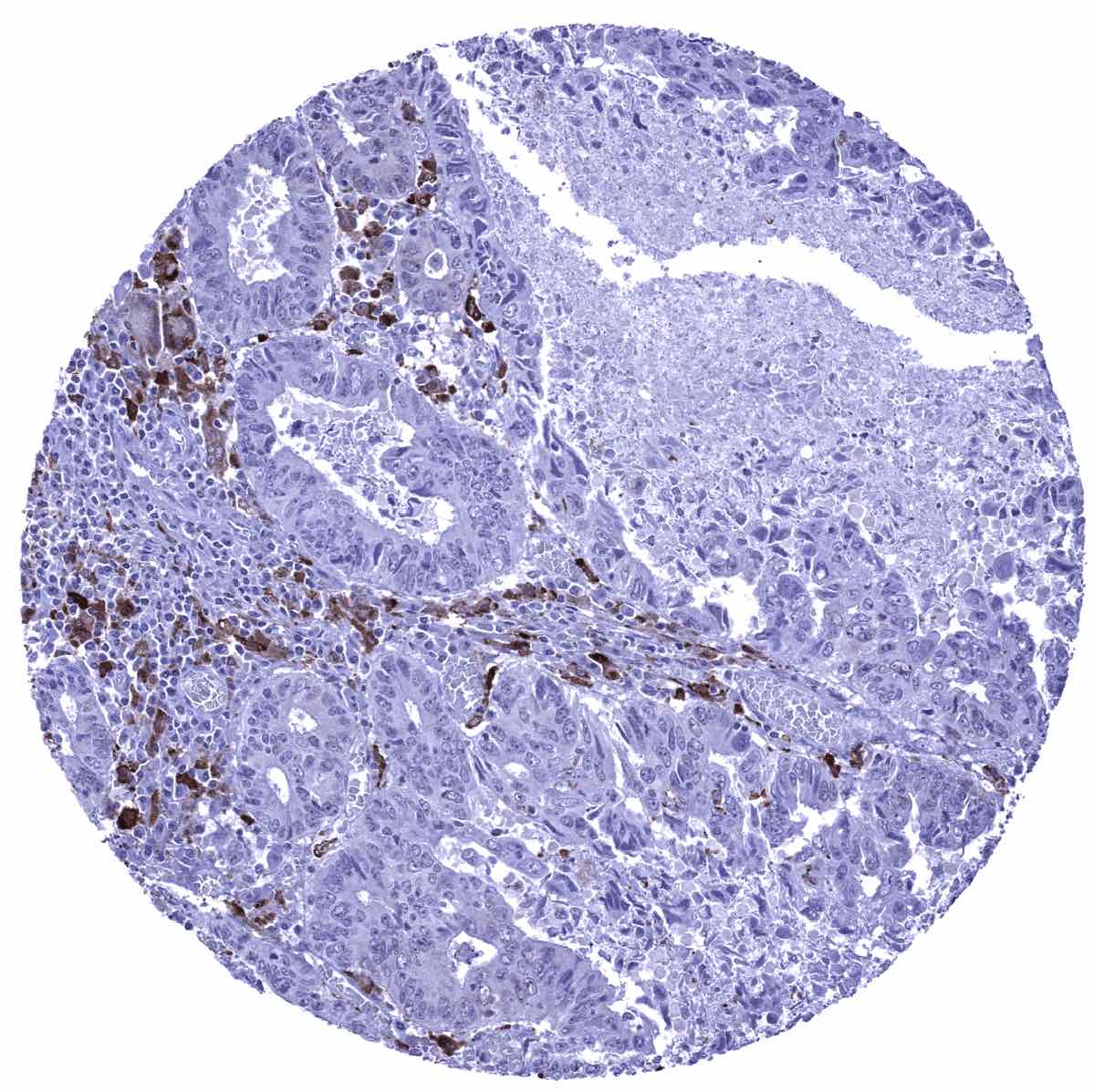
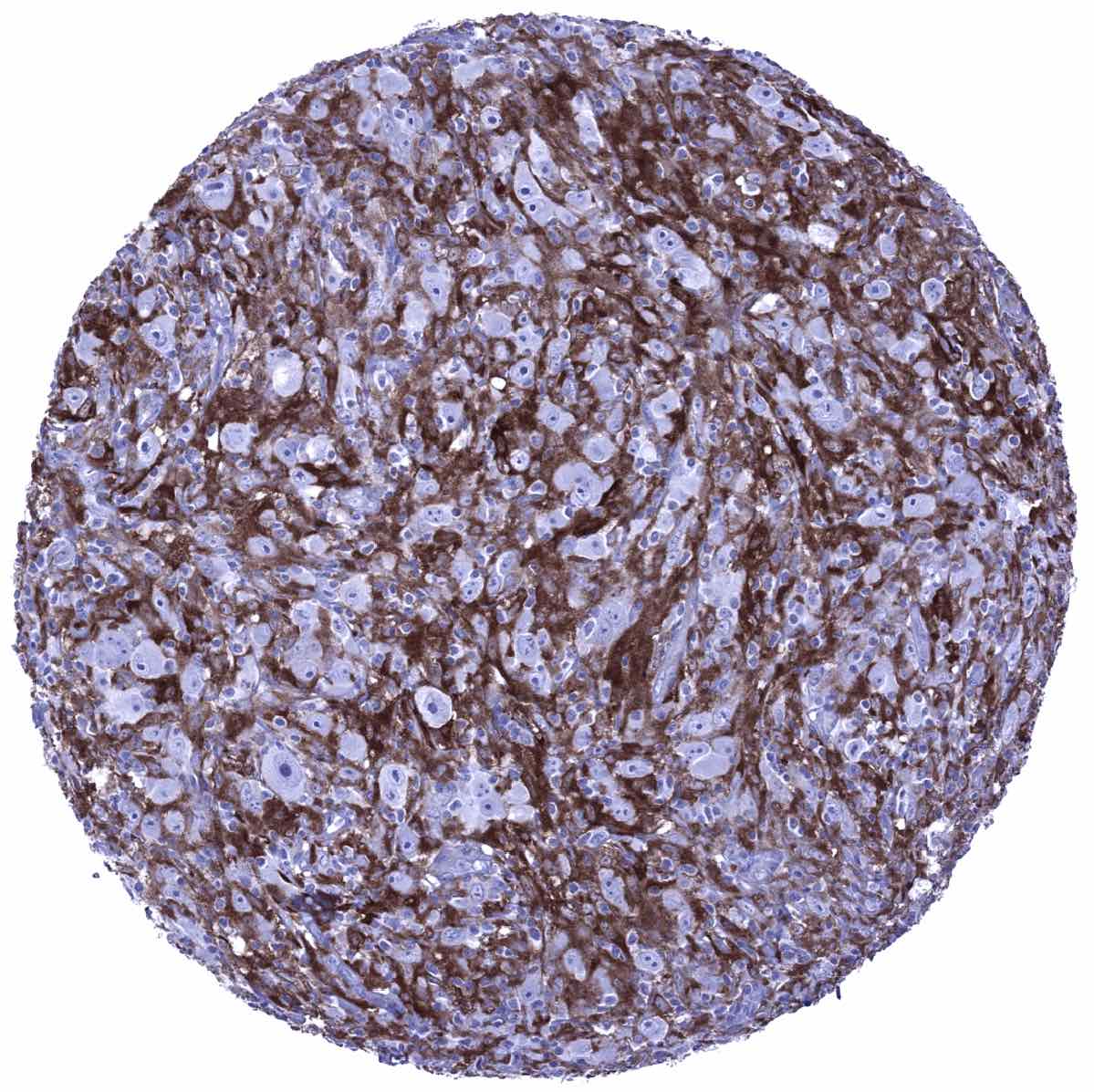
Staining Pattern in Relevant Tumor Types
Most immature and mature B-cell neoplasms express CD22 at a variable extent. CD22 immunostaining can be particularly strong in hairy cell leukemia and prolymphocytic leukemia. T cells and their malignant counterparts, except for rare cases, do not express CD22.
The TCGA findings on Glutamine Synthetase RNA expression in different tumor categories have been summarized in the Human Protein Atlas.

Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-750M at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Agilent / Dako – Autostainer Link 48
Pretreatment in PT-Link for 30 minutes at 95°C (pH high); FLEX peroxidase blocking for 5 minutes (room temperature), MSVA-750M 1:150 for 20 minutes (room temperature), FLEX+ mouse/rabbit (LINKER) for 15 minutes (room temperature), horseradish peroxidase (HRP) for 20 minutes (room temperature), FLEX DAB+Sub-Chromo for 10 minutes (room temperature), FLEX hematoxylin for 5 minutes (room temperature).

These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, and a longer incubation time of FLEX+LINKER result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Leica – BOND RX
Dewax at 72°C for 30 seconds; Pretreatment in Bond Epitope Retrieval Solution (ER2 – EDTA pH9) for 20 minutes at 100°C; Peroxidase blocking for 5 minutes (room temperature), MSVA-750M 1:150 for 15 minutes (room temperature), Post primary (rabbit anti mouse) for 8 minutes (room temperature), Polymer (goat anti rabbit) for 8 minutes (room temperature), mixed DAB refine for 10 minutes (room temperature), hematoxylin for 5 minutes (room temperature).

These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of Post primary and or the Polymer result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Roche – Ventana Discovery ULTRA
Pretreatment for 64 minutes at 100°C (pH 8,4); CM peroxidase blocking for 12 minutes (room temperature), MSVA-750M 1:150 for 20 minutes at 36°C, secondary antibody (anti-mouse HQ) for 12 minutes at 36°C, anti-HQ HRP for 12 minutes at room temperature, DAB at room temperature, hematoxylin II at room temperature for 8 minutes, bluing reagent at room temperature for 4 minutes.
These images depict staining results obtained by the protocol described above. It is of note, that the Ventana machines generally require higher antibody concentrations than other commonly used autostainers because the antibodies are automatically diluted during the procedure. Various other protocols can result in an identical result as shown above. A longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of secondary antibody and or the anti-HQ HRP result in stronger staining, potentially at the cost of more background staining.
Potential Research Applications
- Glutamine synthetase is a pivotal gene for cell metabolism. Its expression level is variable in many cell types including cancer cells. The clinical significance of an altered expression of glutamine synthetase in cancer and other diseases should be explored in more detail.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For proteins such as Glutamine synthetase which are expressed in virtually all tissues, orthogonal validation is not well suited. However, the RNA data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression Glutamine Synthetase) are consistent with ubiquitous expression of Glutamine synthetase.
Comparison of antibodies: A specific staining of the Glutamine synthetase antibody MSVA-750M is, however, confirmed by an identical staining pattern seen by employing an independent commercial antibody (termed: “Validation Antibody”). Images derived from then antibody comparison are shown below. Note: At the selected experimental conditions staining by the “Validation Antibody” is weaker. Despite this difference, identical cells are stained by both antibodies.
Antibody Comparison: MSVA-022R vs another commercially available CD22 antibody called “Validation Antibody”