
295,00 € – 995,00 €
Product details
Synonyms = BCH, Benign chorea, BHC, Homeobox protein Nkx2.1, NK2 homeobox 1, NKX2.1, NKX2A, TEBP, Thyroid nuclear factor-1, Thyroid specific enhancer binding protein, Thyroid transcription factor-1 (TTF-1), Tin man, TITF1, TTF-1
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = MSVA-312R
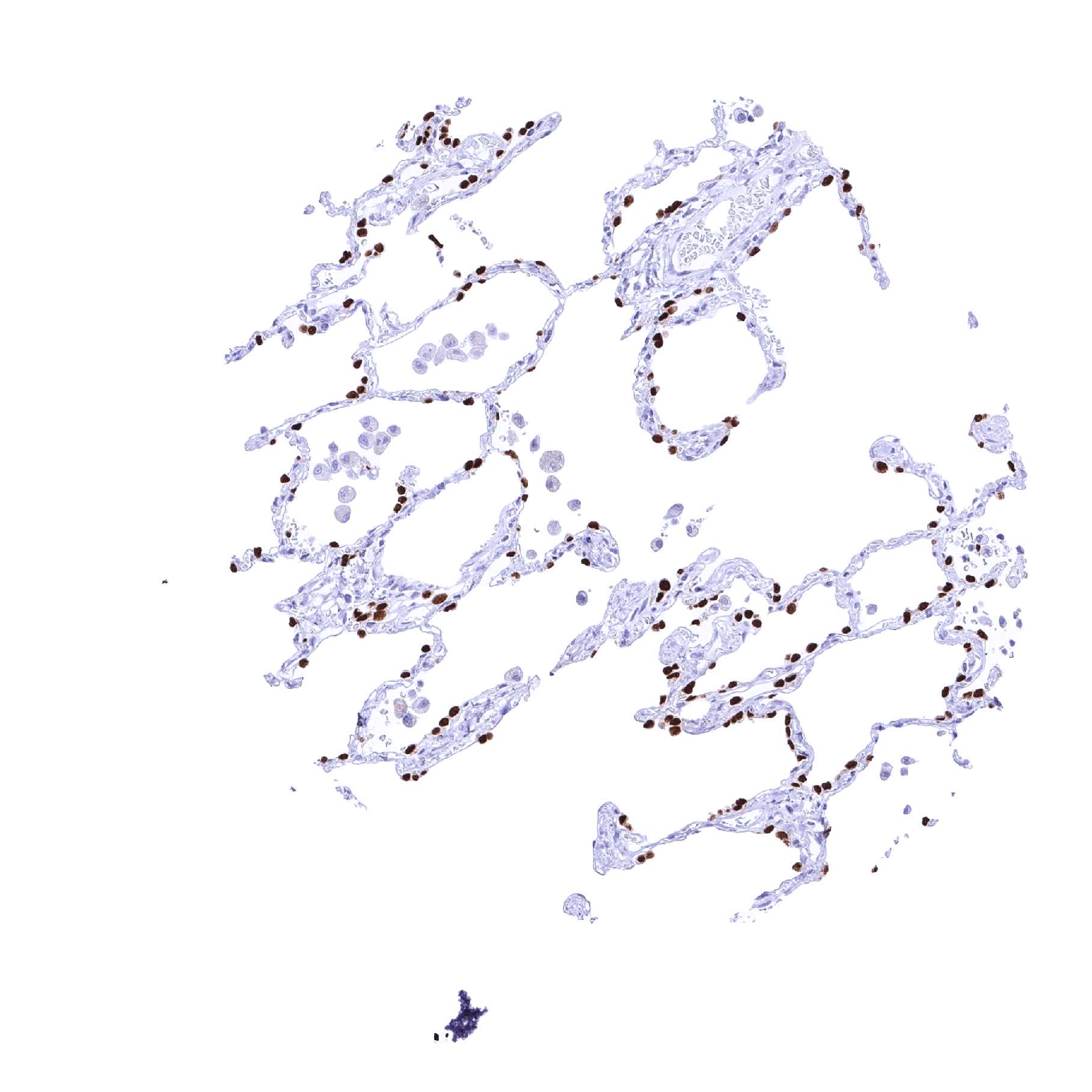
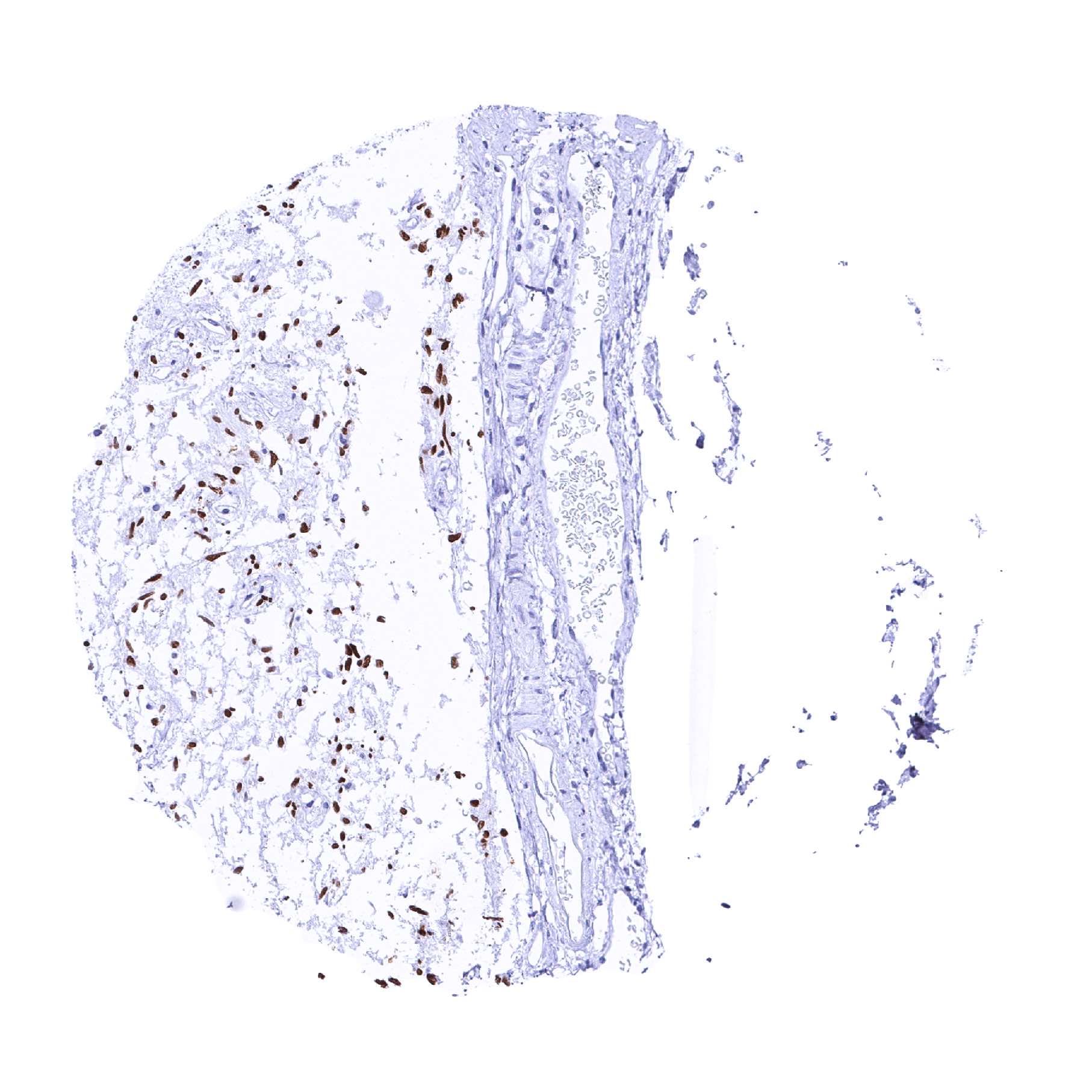
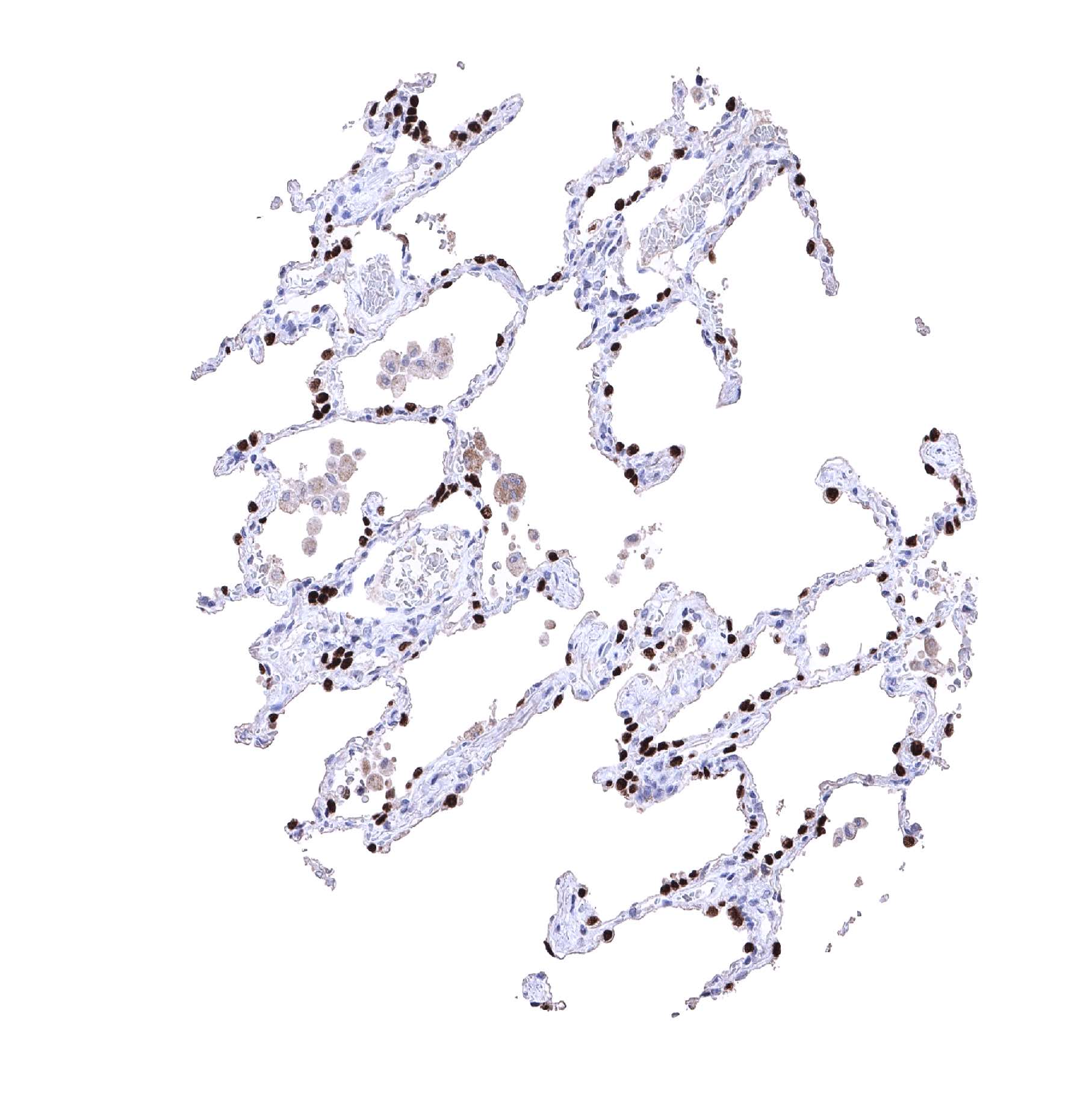
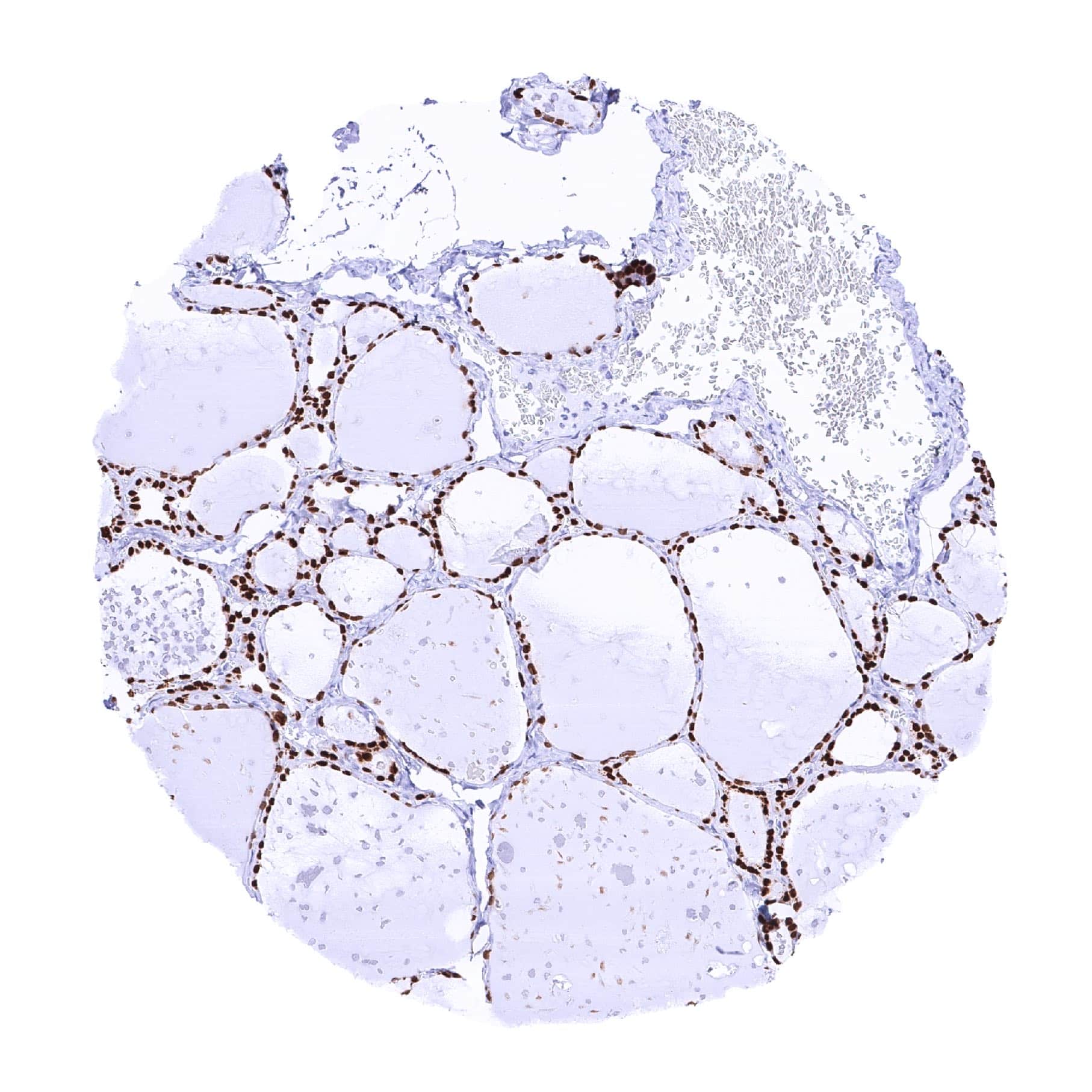
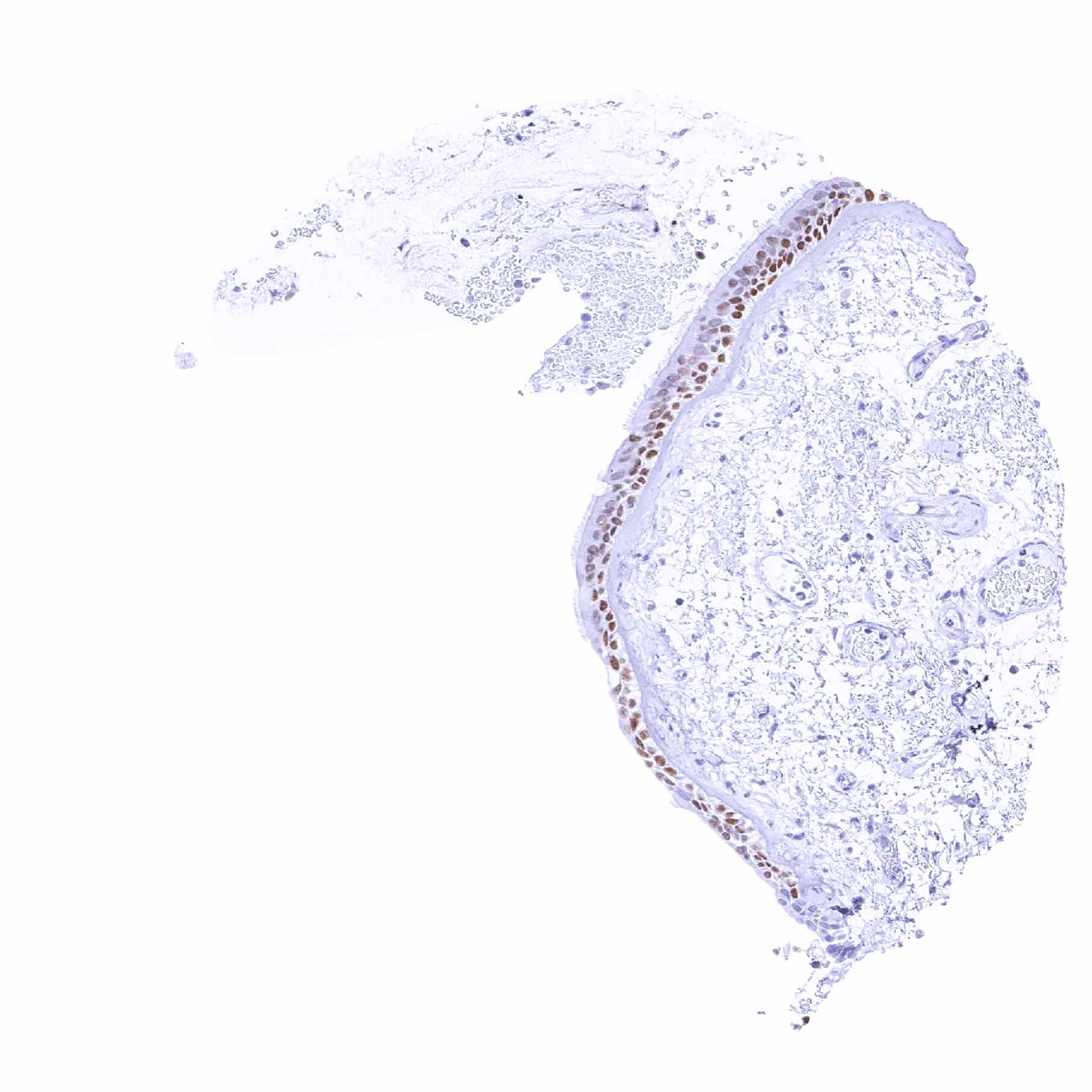
Positive control = Lung: Nuclear TTF1 staining should be strong in pneumocytes and in basal cells of the terminal bronchioles while a weaker, still moderate to strong staining should be seen in columnar epithelial cells of the terminal bronchioles (low expressor control).
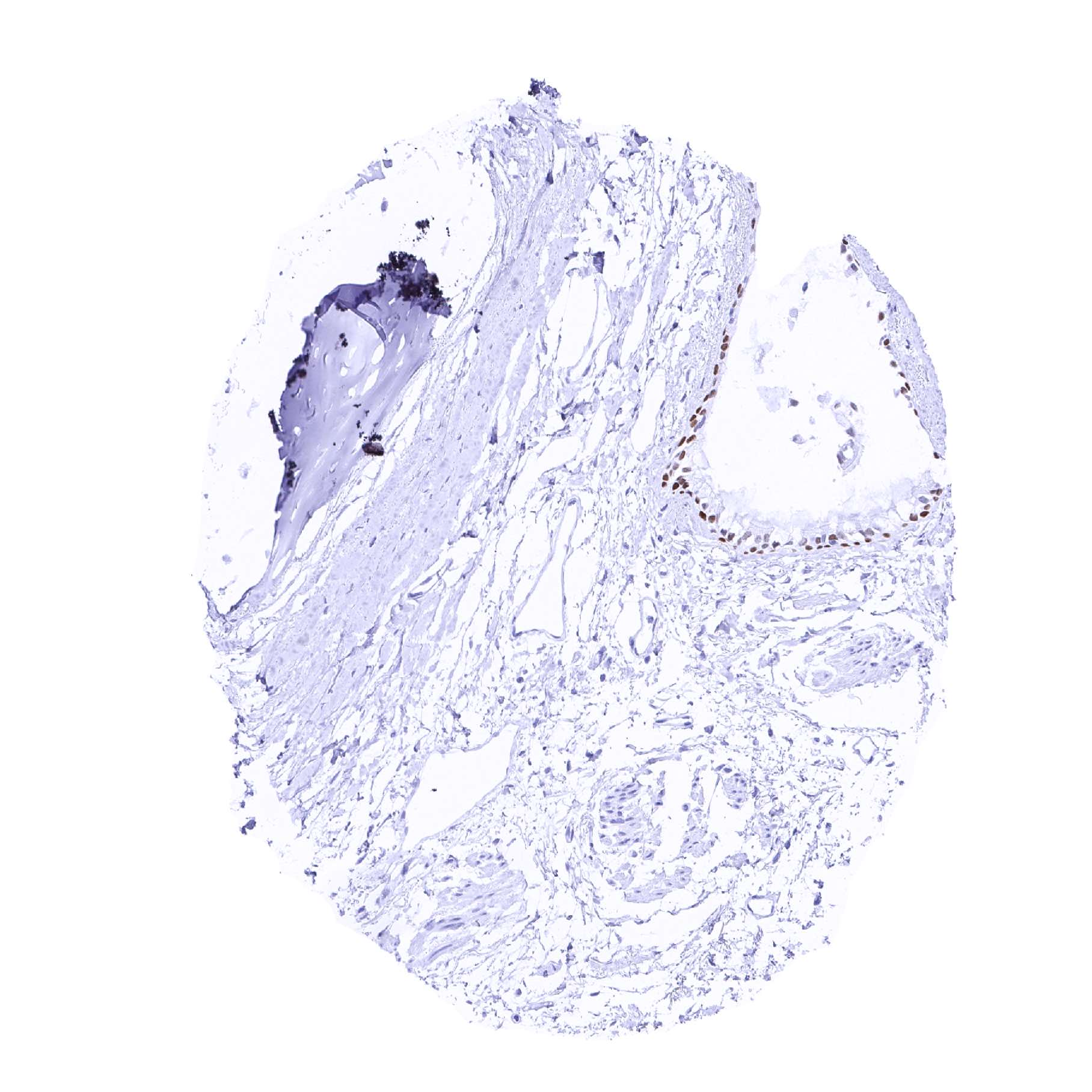
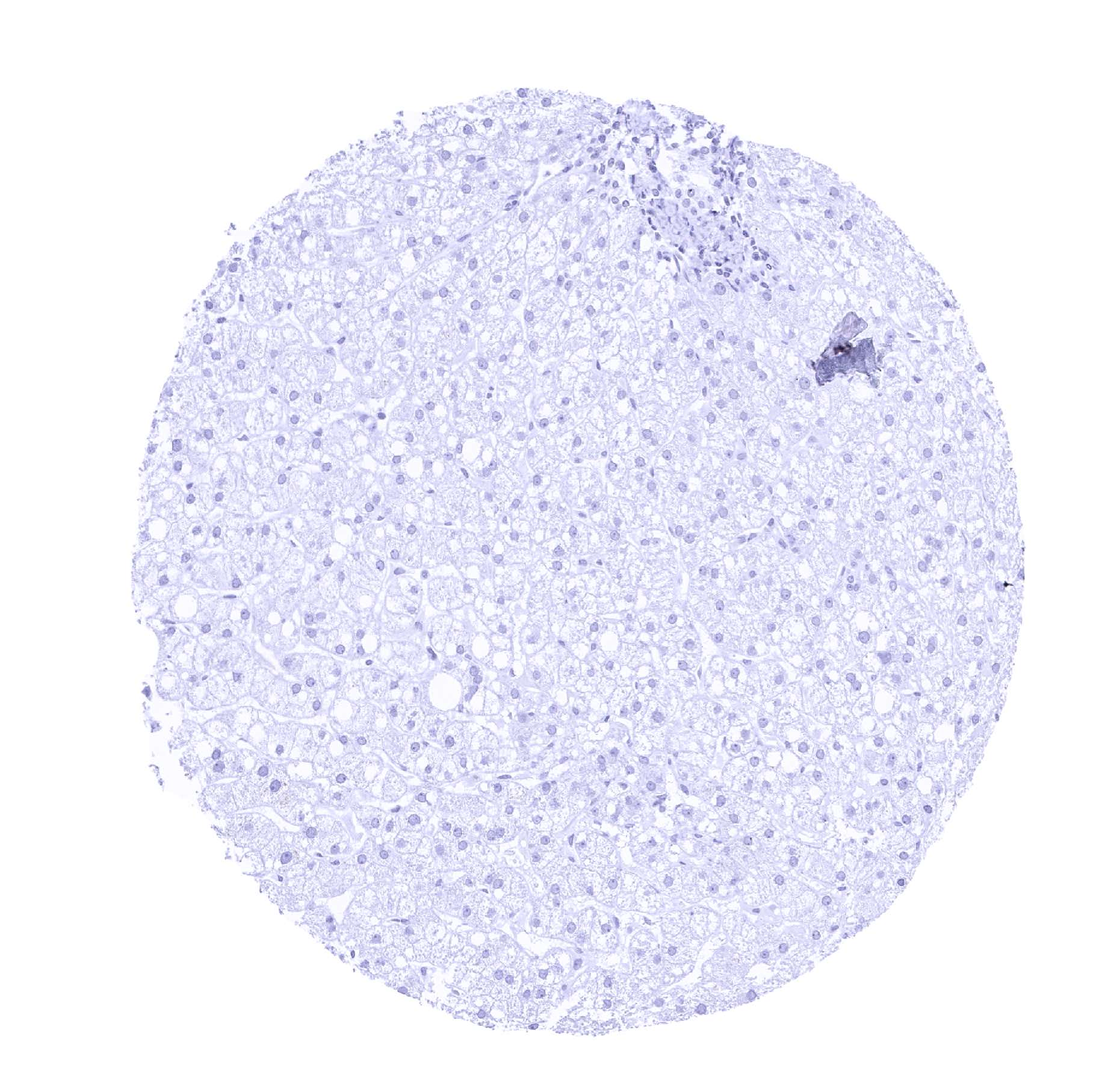
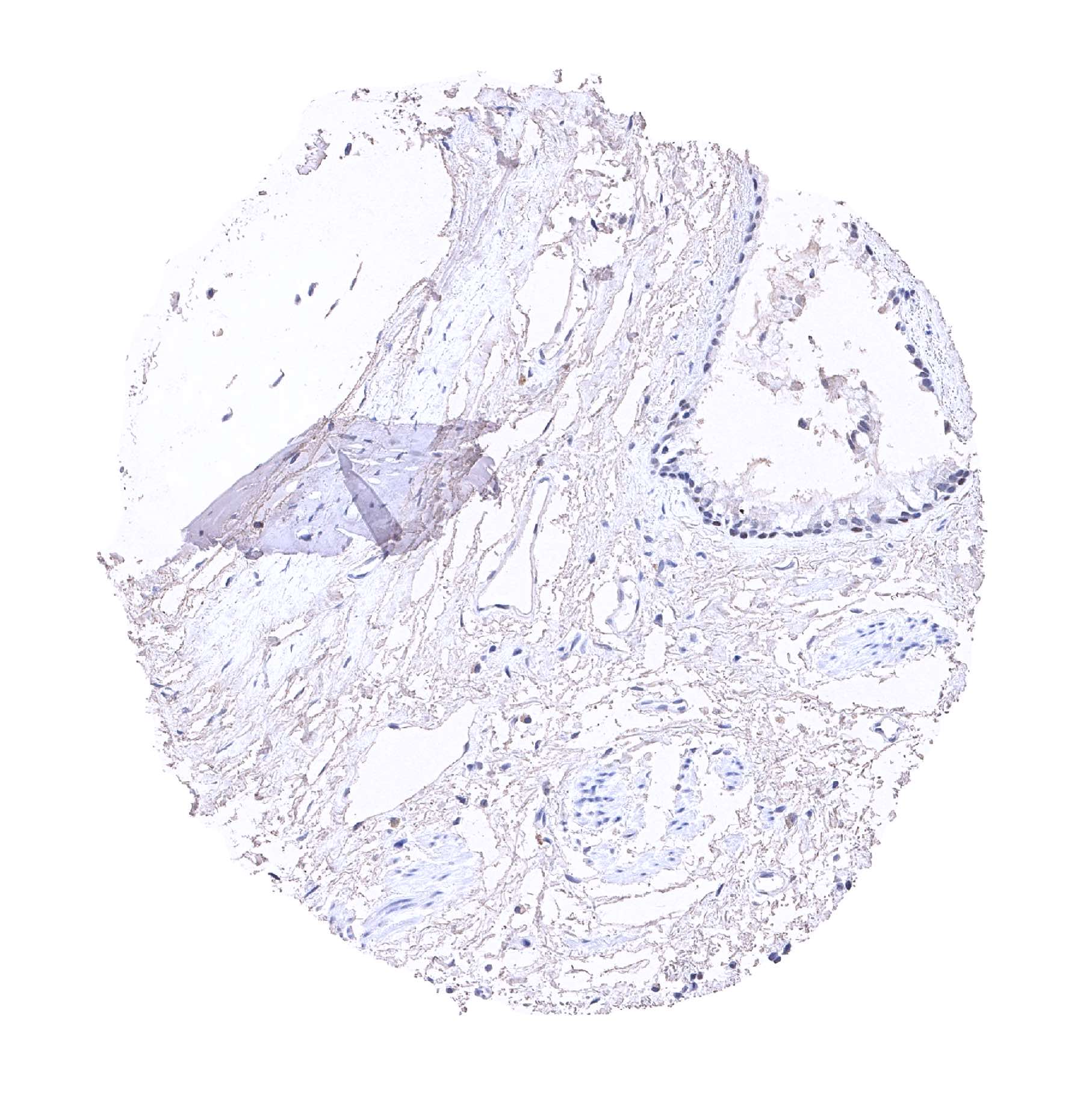
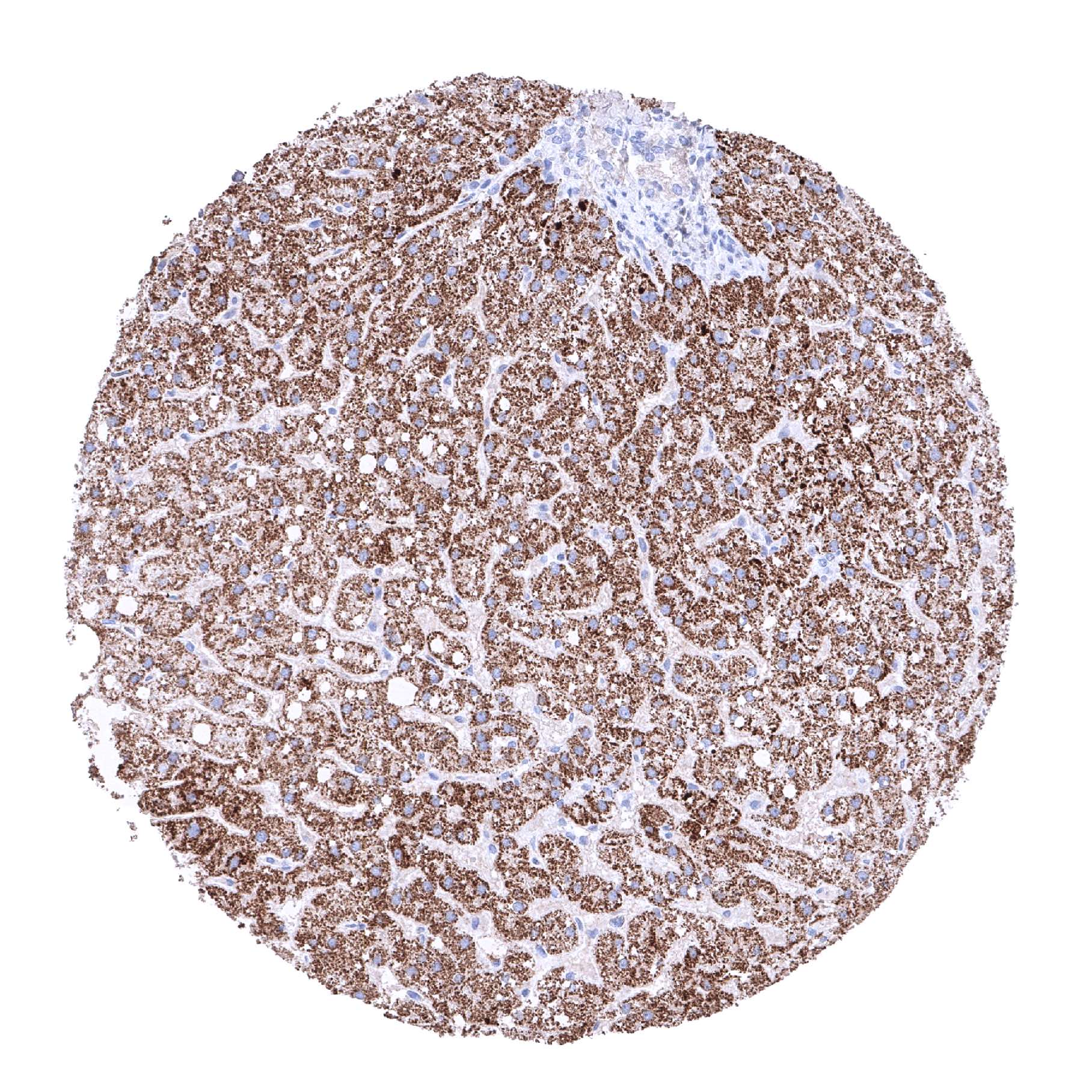
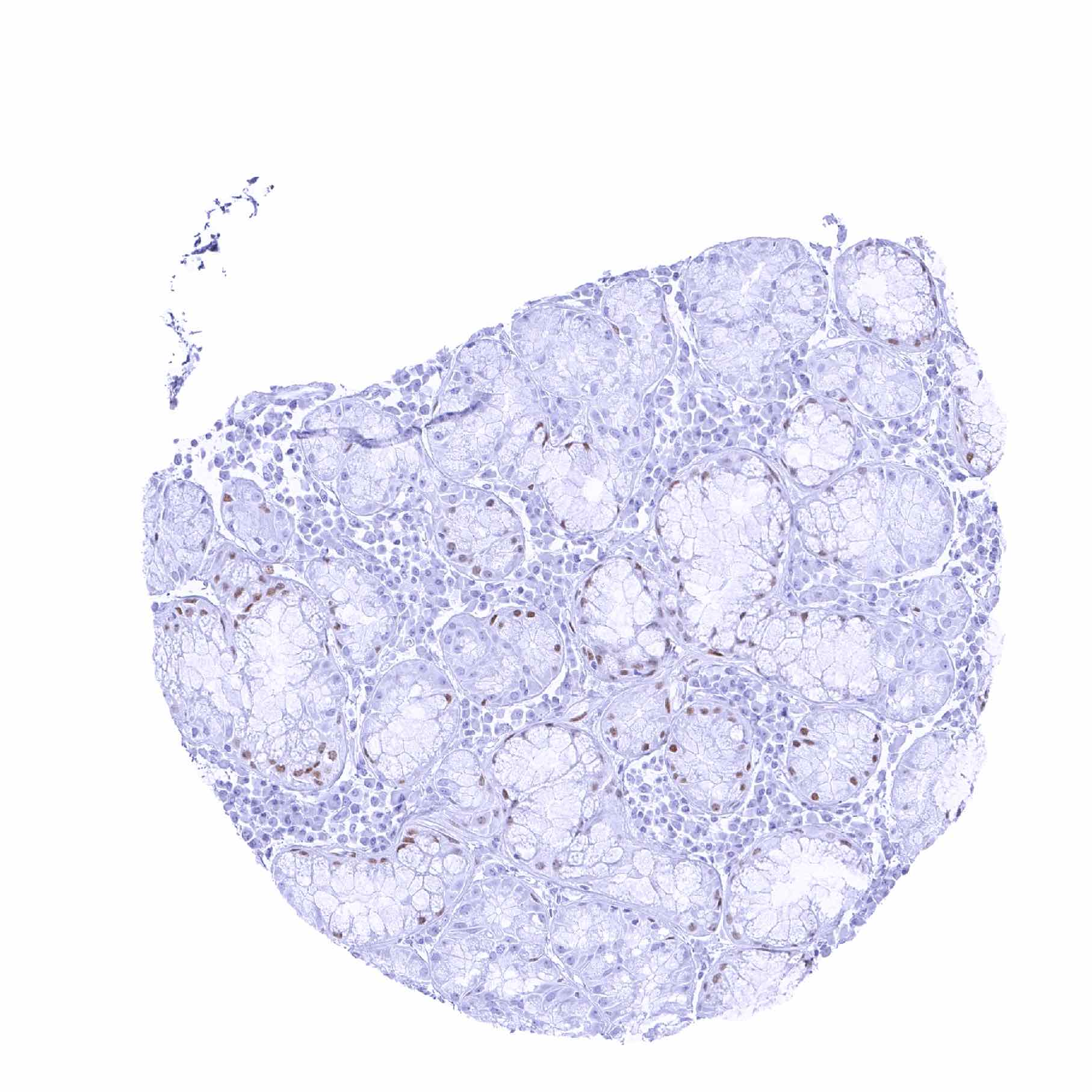
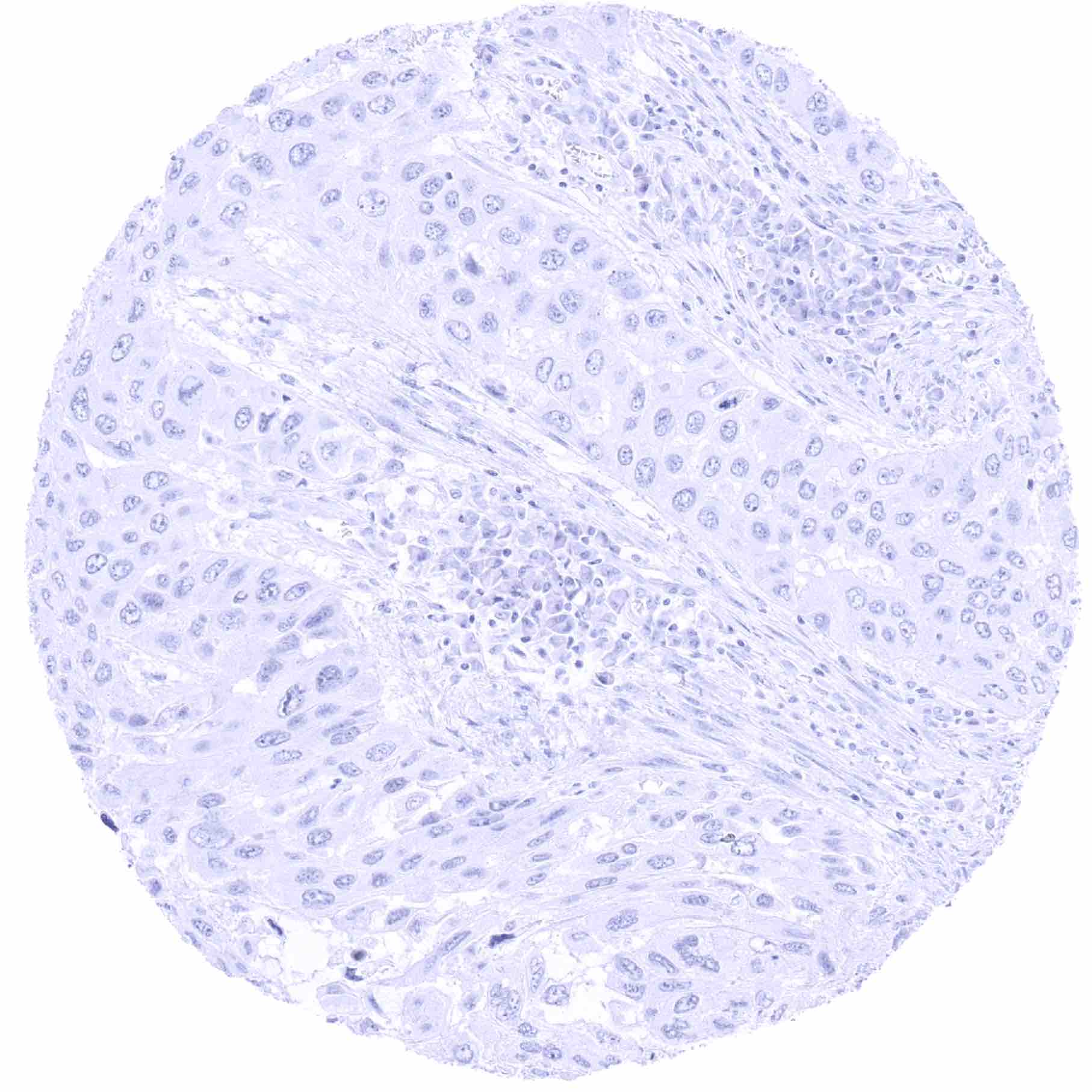
Negative control = Liver: TTF1 staining must not be seen in any cells.
Cellular localization = Nucleus
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
TTF-1 is a protein with high specificity for lung and thyroid.
Biology Behind
Thyroid transcription factor-1 (TTF1), also termed NK2 homeobox 1 (NKX2-1) is a 38 kDa nuclear protein encoded by the NKX2-1 gene at chromosome 14q13. TTF1 has a critical role in morphogenesis of the thyroid, the lung and the diencephalon where it acts as a tissue-specific transcription promoter. Blocking TTF1 gene expression results in developmental defects of thyroid, lung and brain. In the thyroid gland, TTF1 induces the expression of thyroglobulin, thyroperoxidase and thyrotropin receptor. In the lung, TTF1 promotes the transcription of the surfactant proteins A to D, and the Clara cell secretory protein. Among normal tissues, TTF1 expression is restricted to the respiratory system, thyroid, pituitary gland, and the thalamus. Among cancers, TTF1 expression is particularly common in thyroid cancer, pulmonary adenocarcinoma, pulmonary small cell carcinomas, as well as in small cell carcinomas from other sites of origin. Less commonly, TTF1 positivity is also seen in other tumor entities including colorectal, endometrial and stomach cancers.
Staining Pattern in Normal Tissues
Images describing the TTF1 staining pattern in normal tissues obtained by the antibody MSVA-312R are shown in our “Normal Tissue Gallery”.
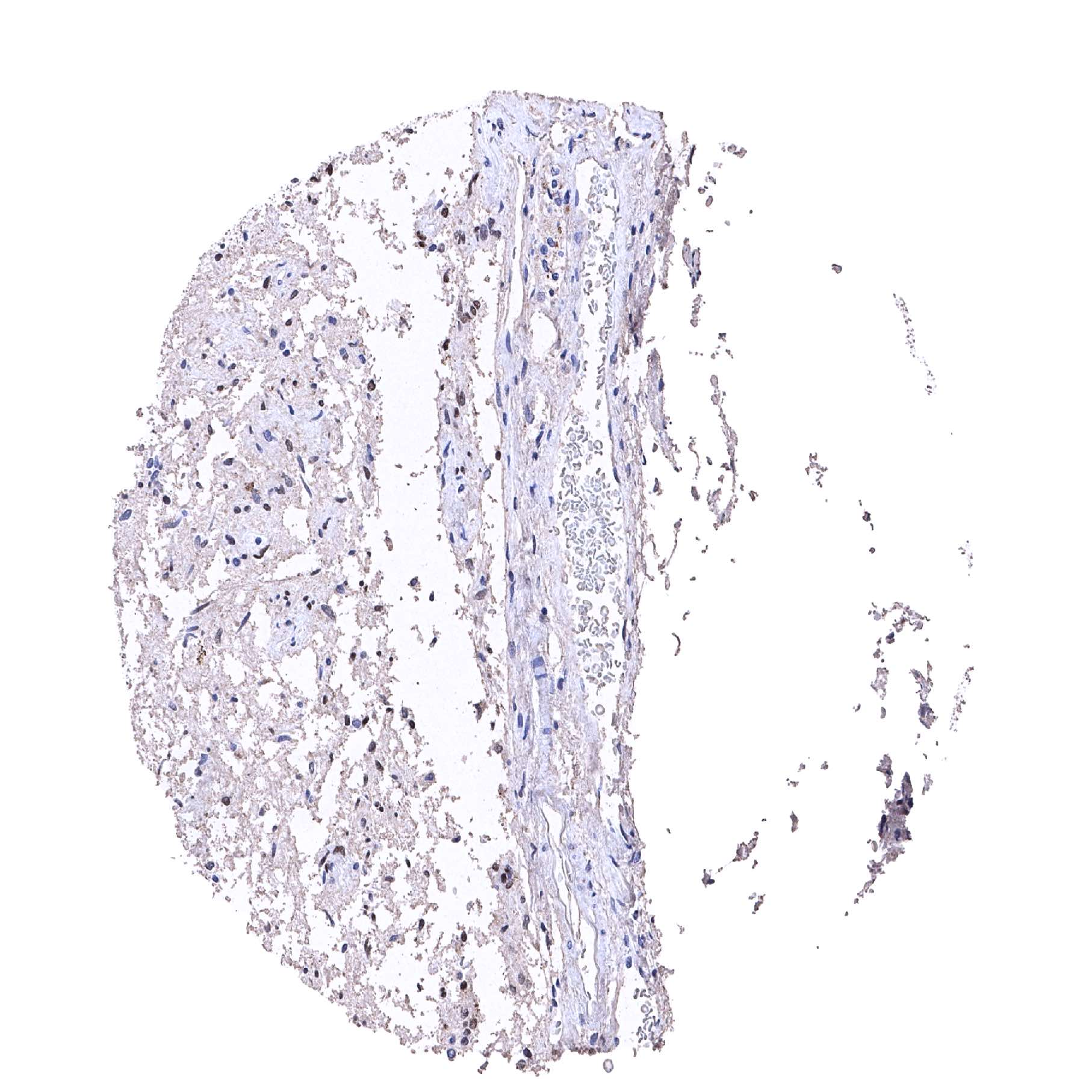
| Brain | Cerebrum | Negative. |
| Cerebellum | Negative. | |
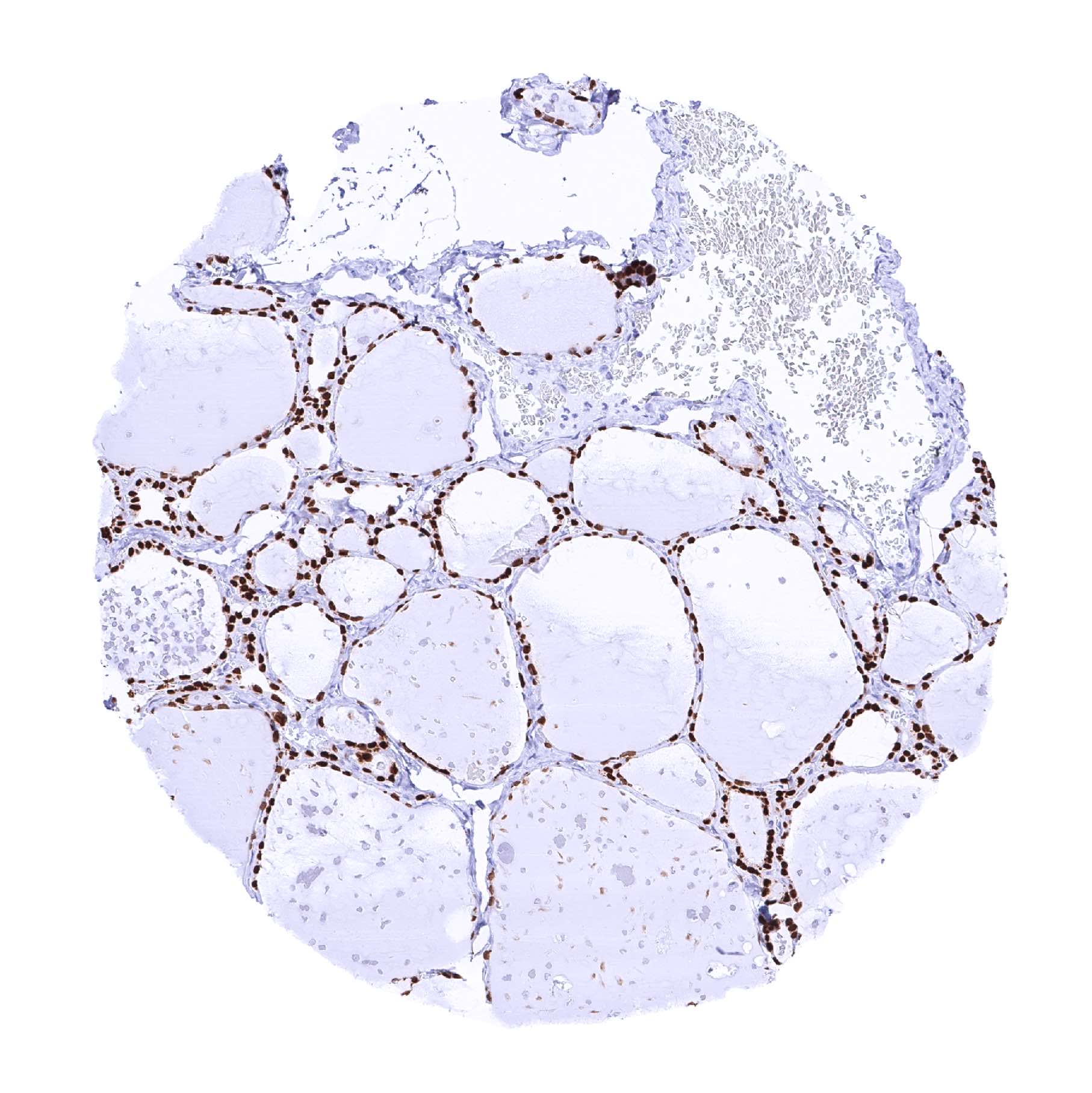
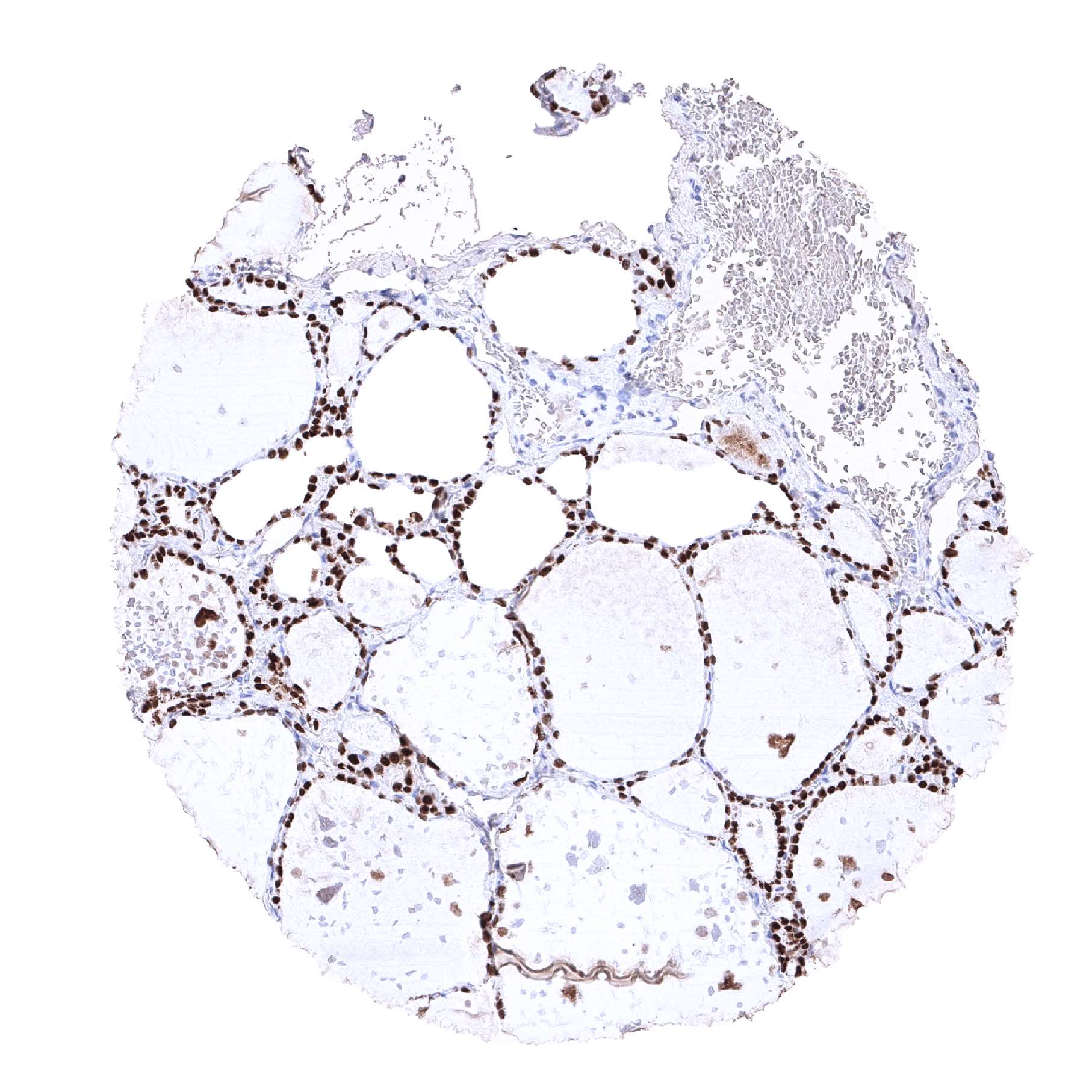
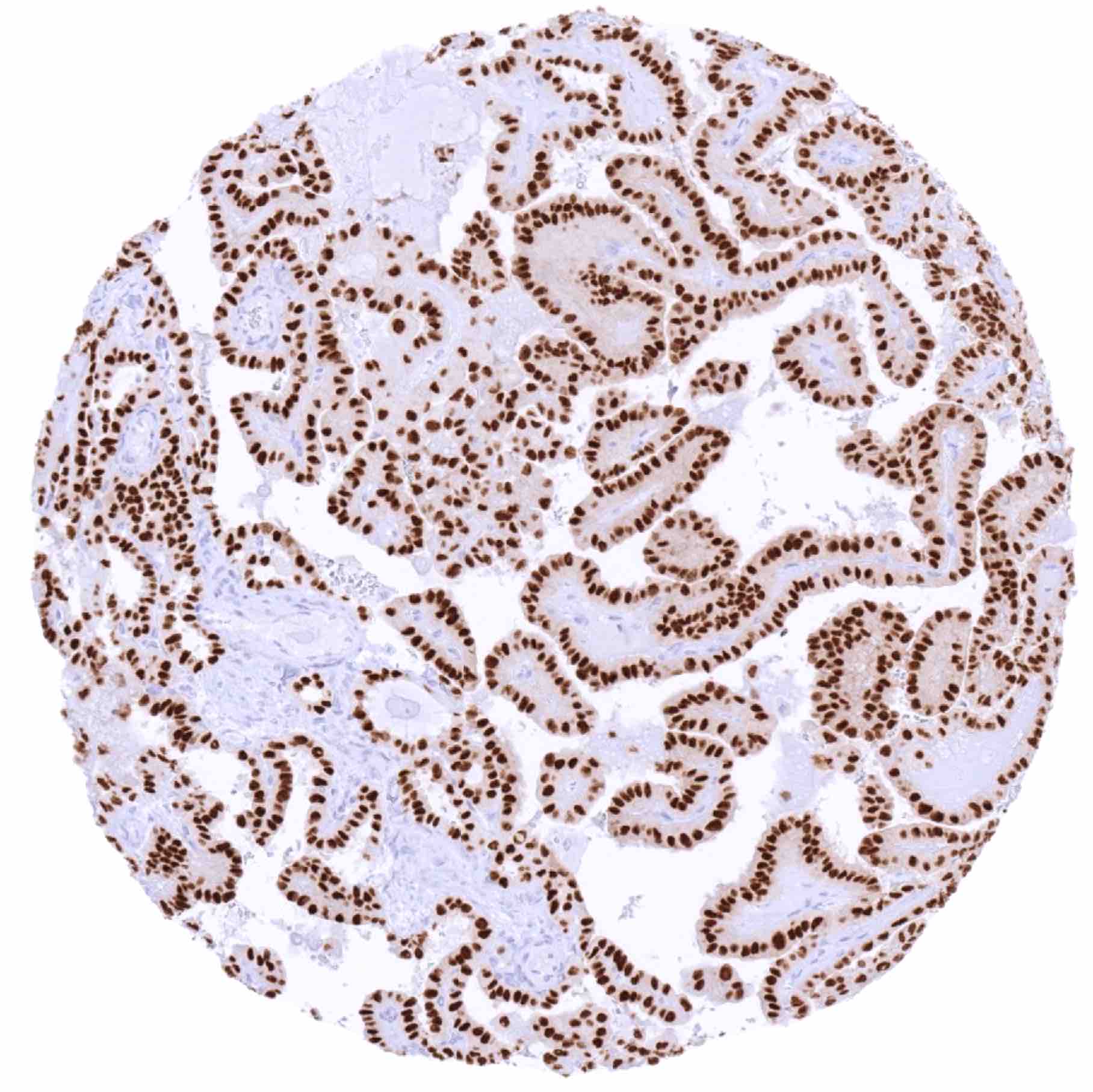
| Endocrine Tissues | Thyroid | StrongTTF1 staining of all follicular epithelial cells. |
| Parathyroid | Negative. | |
| Adrenal gland | Negative. | |
| Pituitary gland | StrongTTF1 staining of pituicytes. | |
| Respiratory system | Respiratory epithelium | Strong TTF1 staining of respiratory epithelial cells, especially of basal cells in bronchial mucosa. TTF1 staining is much weaker or absent in respiratory epithelial cells of paranasal sinus. Weak to moderate TTF1 positivity of mucinous cells in bronchial glands. |
| Lung | Strong TTF1 staining of pneumocytes. | |
| Gastrointestinal Tract | Salivary glands | Negative. |
| Esophagus | Negative. | |
| Stomach | Negative. | |
| Duodenum | Negative. | |
| Small intestine | Negative. | |
| Appendix | Negative. | |
| Colon | Negative. | |
| Rectum | Negative. | |
| Liver | Negative. | |
| Gallbladder | Negative. | |
| Pancreas | Negative. | |
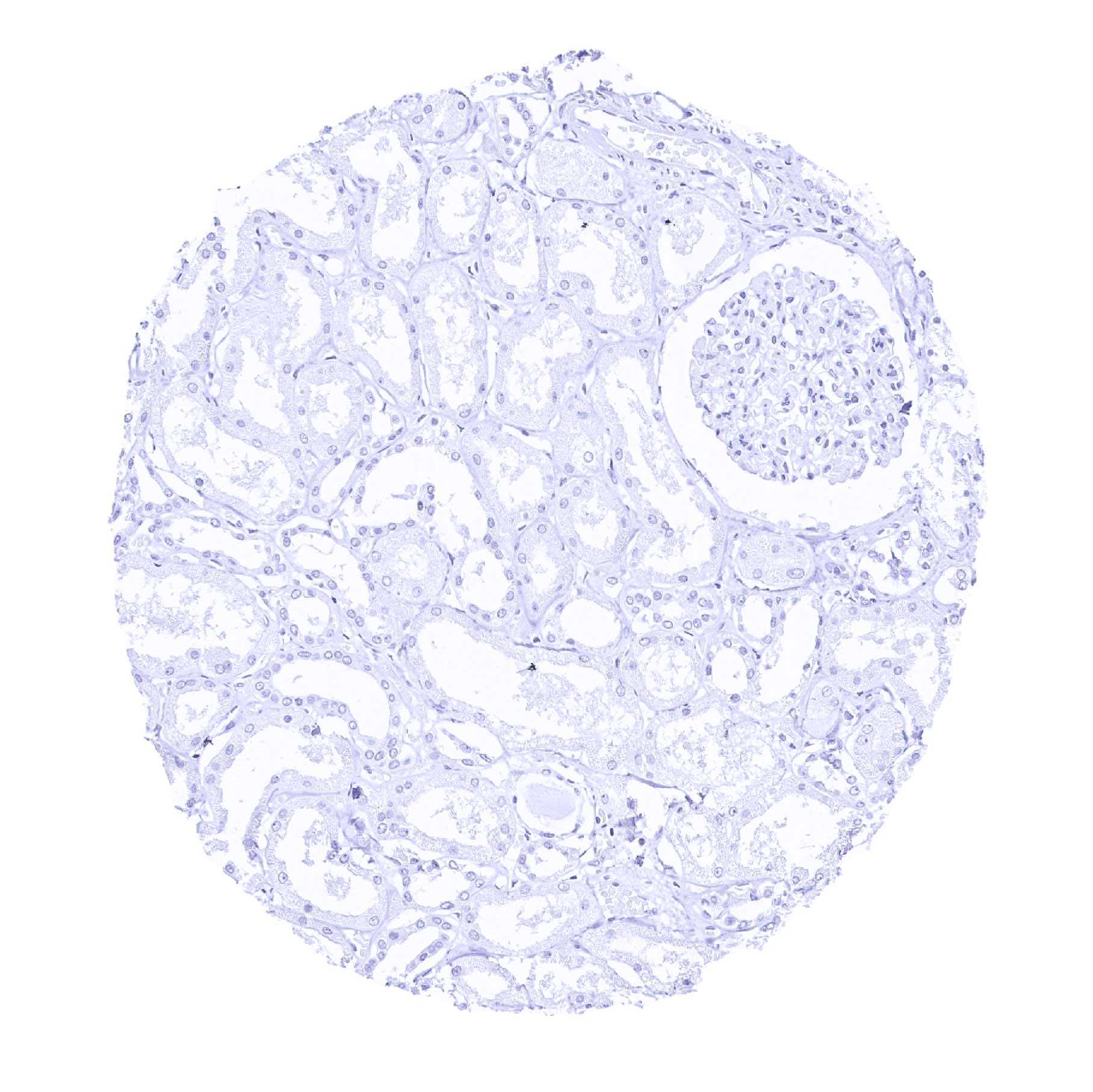
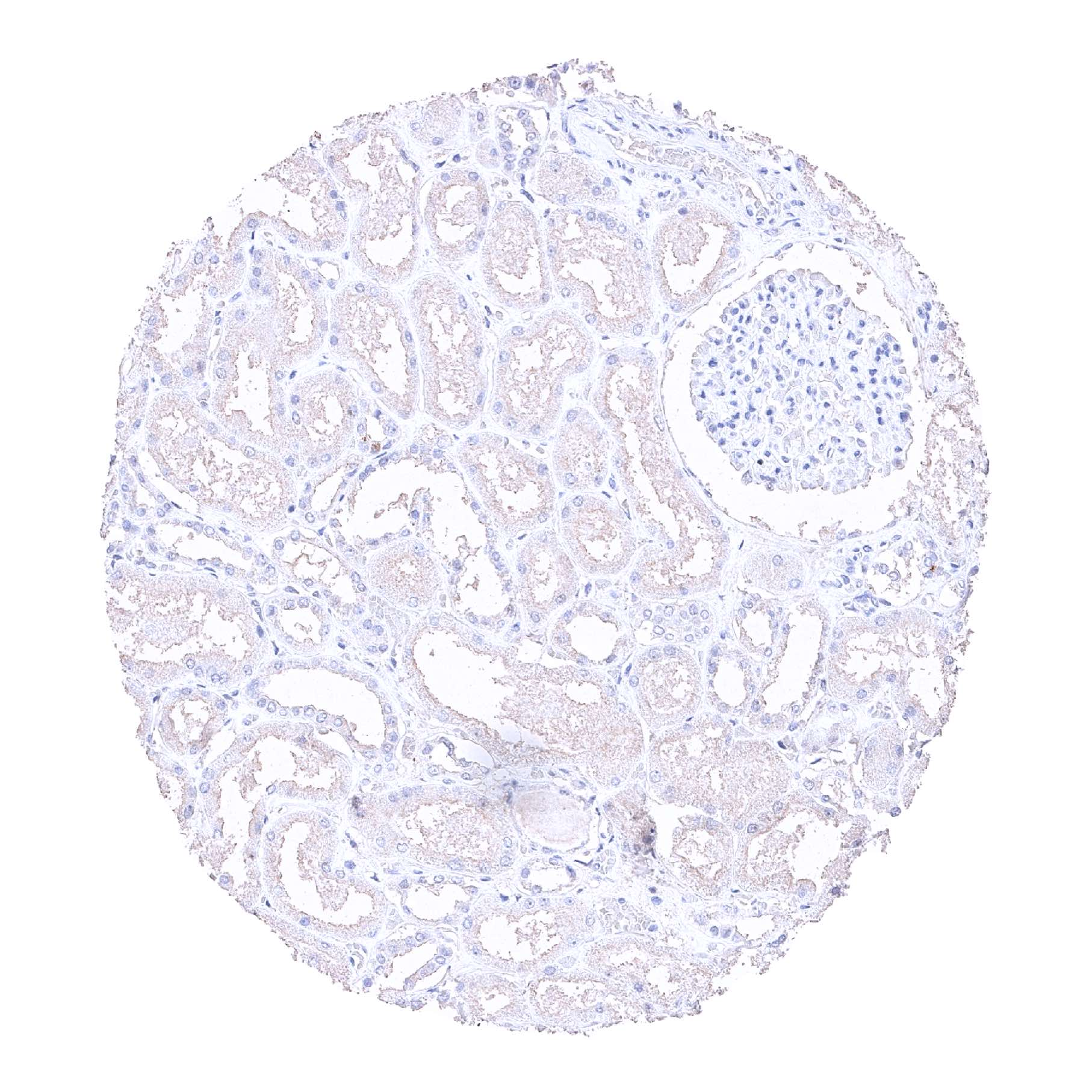
| Genitourinary | Kidney | Negative. |
| Urothelium | Negative. | |
| Male genital | Prostate | Negative. |
| Seminal vesicles | Negative. | |
| Testis | Negative. | |
| Epididymis | Negative. | |
| Female genital | Breast | Negative. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Negative. | |
| Uterus endocervix | Negative. | |
| Uterus, endometrium | Negative. | |
| Fallopian Tube | Negative. | |
| Ovary | Negative. | |
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | Negative. | |
| Chorion | Negative. | |
| Skin | Epidermis | Negative. |
| Sebaceous glands | Negative. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/lymphoid tissue | Bone marrow | Negative. |
| Lymph node | Negative. | |
| Spleen | Negative. | |
| Thymus | Negative. | |
| Tonsil | Negative. | |
| Remarks | TTF1 staining is always nuclear. |
These findings are largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression TTF-1) All organs with documented TTF1 RNA expression (respiratory system, thyroid, pituitary gland) are IHC positive for MSVA-312R. Moreover, immunostaining by MSVA-312R is also limited to these organs.
Positive control = Lung: Nuclear TTF1 staining should be strong in pneumocytes and in basal cells of the terminal bronchioles while a weaker, still moderate to strong staining should be seen in columnar epithelial cells of the terminal bronchioles (low expressor control).
Negative control = Liver: TTF1 staining must not be seen in any cells.
Staining Pattern in Relevant Tumor Types
Among thyroid cancers, TTF1 is seen in virtually all tumors derived from follicular cells (i.e. follicular adenoma, follicular and papillary carcinoma). C-cell derived medullary carcinomas are mostly TTF1 positive while anaplastic thyroid carcinomas are usually negative. Among lung cancers, adenocarcinomas are positive in 60-85% but mucinous adenocarcinomas are more often negative. Small cell carcinomas of the lung are TTF1 positive in >90% of cases but extrapulmonary small cell carcinomas are also often positive (>40%). TTF1 positivity is (rarely) also seen in other tumor entities including colorectal, endometrial and stomach cancers.
The TCGA findings on TTF-1 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.

Compatibility of Antibodies
TTF‐1 (MSVA-312R ) publication summary
Relevant publication: Möller et al. “TTF‐1 is a highly sensitive but not fully specific marker for pulmonary and thyroidal cancer: a tissue microarray study evaluating more than 17,000 tumors from 152 different tumor entities.” Published in Virchows Archive 2024 Oct 8. Epub ahead of print. PMID: 39377914.
A total of 15’564 tumors from 152 different tumor categories were successfully analyzed by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in a pH 9 Target Retrieval Solution buffer. MSVA-312R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
Overall, 82 of 152 tumor categories showed detectable TTF1 expression in at least one case and 42 tumor categories included at least one case with strong TTF1 positivity. By far the highest positivity rates were seen in various subtypes of thyroidal cancers (up to 100%), adenocarcinomas of the lung (94.3%), neuroendocrine tumors (NET) of the lung (66.7%), small cell neuroendocrine carcinomas (NEC) from multiple organs organs (71.4–80.0%), several types of mesenchymal tumors (up to 41.9%), and in thymomas (39.1%). TTF-1 expression in less than 15% of cases and often at lower intensity was also seen in various other cancer types including several adenocarcinomas and other tumor entities that can metastasize to the lung such as gallbladder adenocarcinoma (14.3%), pancreatic NET (5.4%), high-grade endometrial carcinoma (12.5%), urothelial carcinoma (up to 11.5%), adenocarcinoma of the prostate (up to 11.5%, mostly weak positivity), carcinosarcoma of the uterus (9.3%), endometrial serous carcinoma (8.1%), pancreatic/ampullary adenocarcinoma (7.3%), squamous cell carcinomas (up to 6.8%), adenocarcinoma of the stomach (up to 5.9%), colorectal adenocarcinoma (5.2%), and cholangiocarcinoma (3.5%). The distribution of positive staining results is shown in “organ-systematic” and in “ranking order” figures below (images based on data from Möller et al).
Authors conclusions on diagnostic utility of TTF1 IHC with respect to the distinction of benign versus malignant (Möller et al.):
- not applicable.
Authors conclusions on diagnostic utility of TTF1 IHC with respect to the distinction of different tumor entities (Möller et al.):
- TTF-1 is a marker of high sensitivity but insufficient specificity for the distinction of pulmonary adenocarcinomas.
- TTF-1 positivity in a small fraction of gastrointestinal adenocarcinomas represents a significant pitfall mimicking enteric-type pulmonary adenocarcinoma.
- The combined analysis of TTF-1 and Napsin-A significantly improves the specificity for the distinction of pulmonary from extrapulmonary adenocarcinomas.
- The rare occurrence of TTF1 positivity in Merkel cell carcinoma of the skin (differential diagnosis: metastatic pulmonary small cell carcinoma), Ewing sarcoma (differential diagnosis: bone metastasis of a pulmonary small cell carcinoma), and in lymphoma (differential diagnosis: lymph node metastasis of a pulmonary small cell carcinoma) represent important potential diagnostic pitfalls.
Authors conclusions on the prognostic role of TTF1 IHC results (Möller et al.):
- not applicable.
Data from the publication: Möller et al. “TTF‐1 is a highly sensitive but not fully specific marker for pulmonary and thyroidal cancer: a tissue microarray study evaluating more than 17,000 tumors from 152 different tumor entities.” Published in Virchows Archive 2024 Oct 8. Epub ahead of print. PMID: 39377914.
Summarized in own graphics:
Figure 1. TTF-1 staining in tumors (“organ specific” ; according to Möller et al.”) with antibody MSVA-312R

Figure 2. TTF-1 staining in tumors (“ranking order” ; according to Möller et al.”) with antibody MSVA-312R

Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-312R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- Distinction of lung adenocarcinoma (usually positive) from metastasis to the lung (usually negative) and pleural mesothelioma (negative).
- Distinction of Merkel cell carcinoma (usually negative) from metastatic small cell carcinoma of the lung (mostly positive)
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody MSVA-312R specificity is suggested by the complete concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression TTF-1). TTF1 immunostaining by MSVA-312R was only seen in the three tissues, for which RNA expression had been described (respiratory system, thyroid, pituitary gland).
Comparison of antibodies: True TTF1 staining by MSVA-312R was also corroborated by a staining of all cell types detected by MSVA-312R by a commercially available independent second antibody (termed “validation antibody”).
Independence of the two antibodies used for validation is documented by a multitude of non-specific/cross-reactive stainings that were seen for the validation antibody but not for MSVA-312R. These for example included staining of the brain, intense cytoplasmic staining of the liver as well as less intense cytoplasmic stainings of several other structures such as tubuli of the kidney.