195,00 € – 695,00 €
Product details
Synonyms = Campomelic Dysplasia Autosomal Sex Reversal (CMD1); SRA1; SRXX2; SRY (sex determining region Y) box 9; SRY related HMG box gene 9; Transcription factor SOX9
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = MSVA-709R
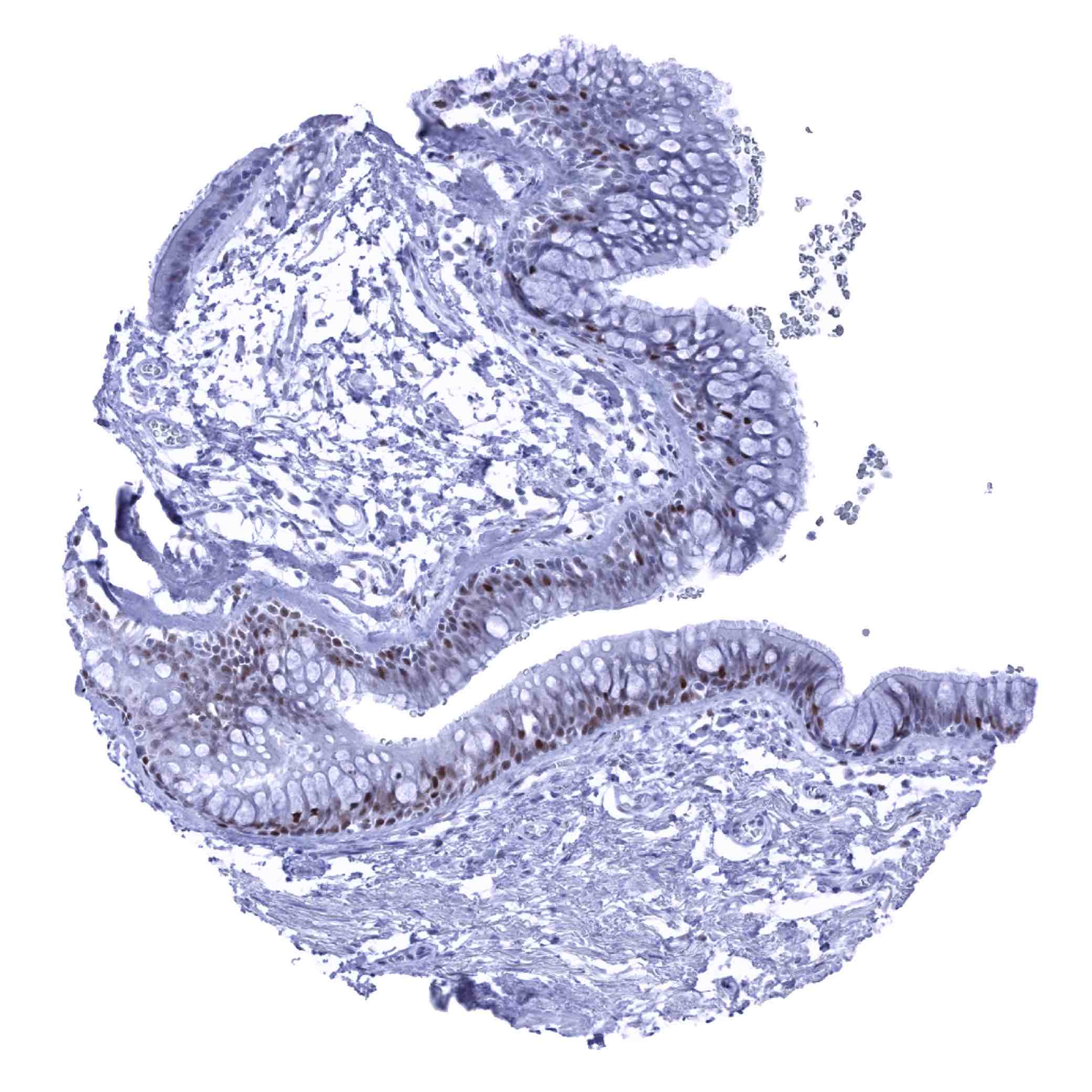
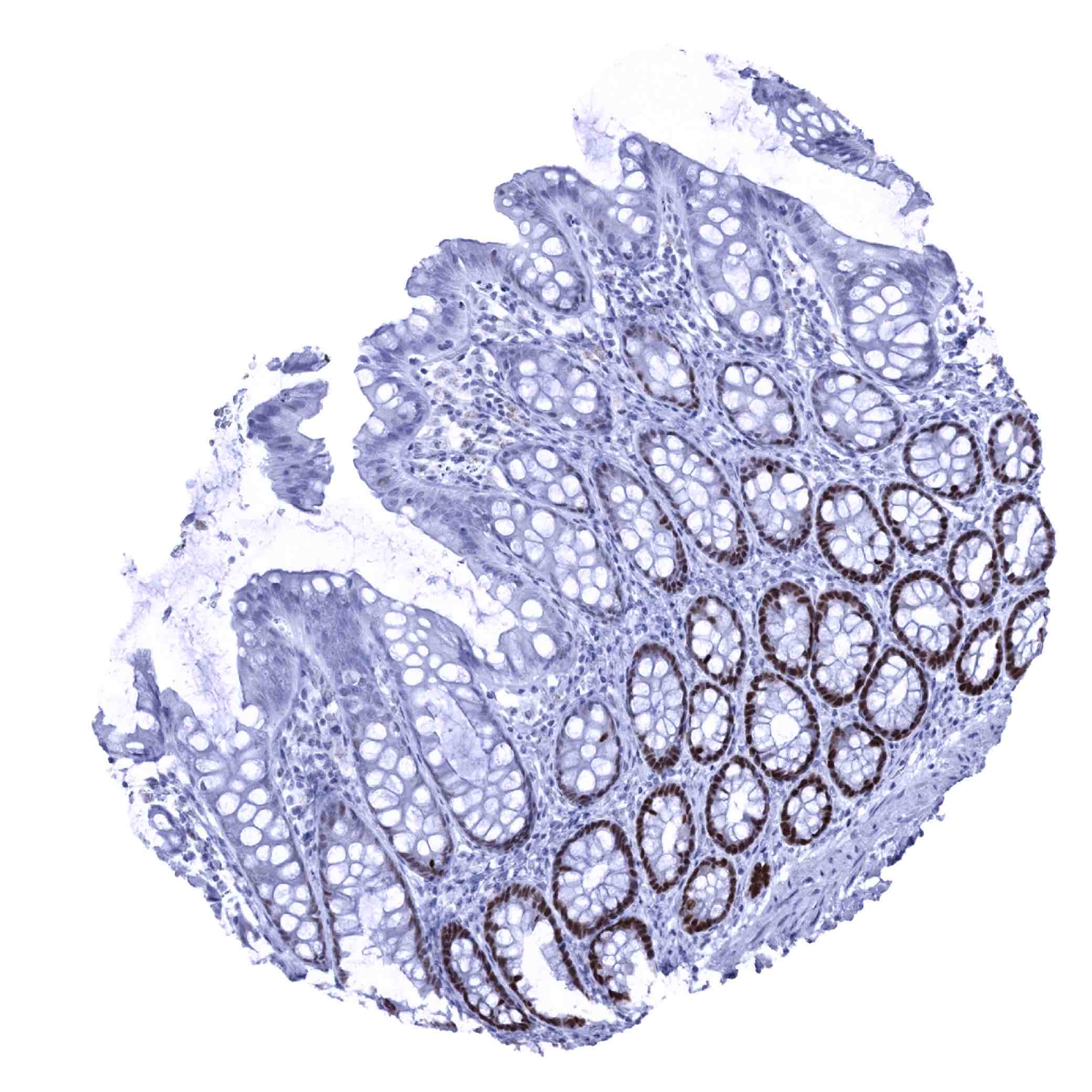
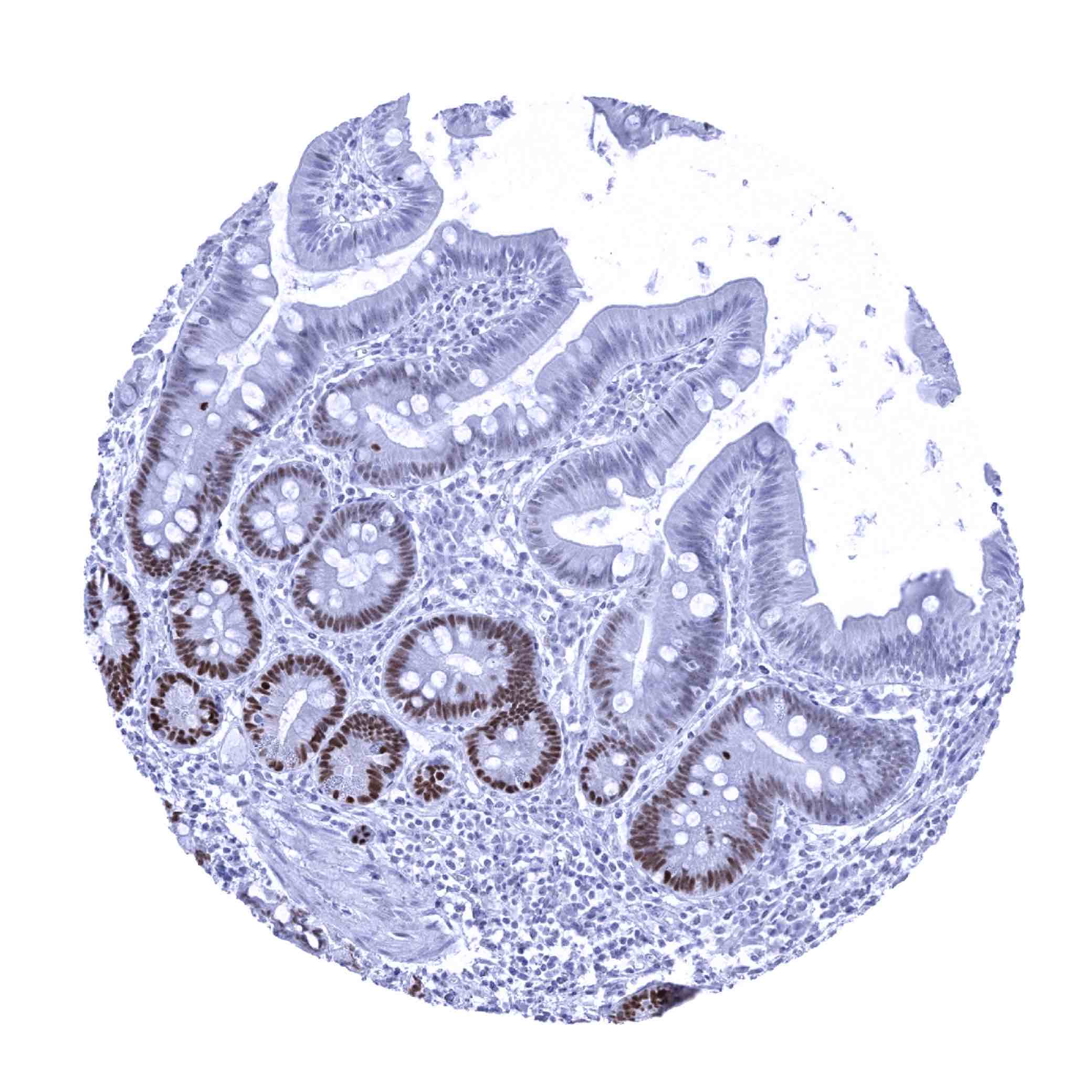
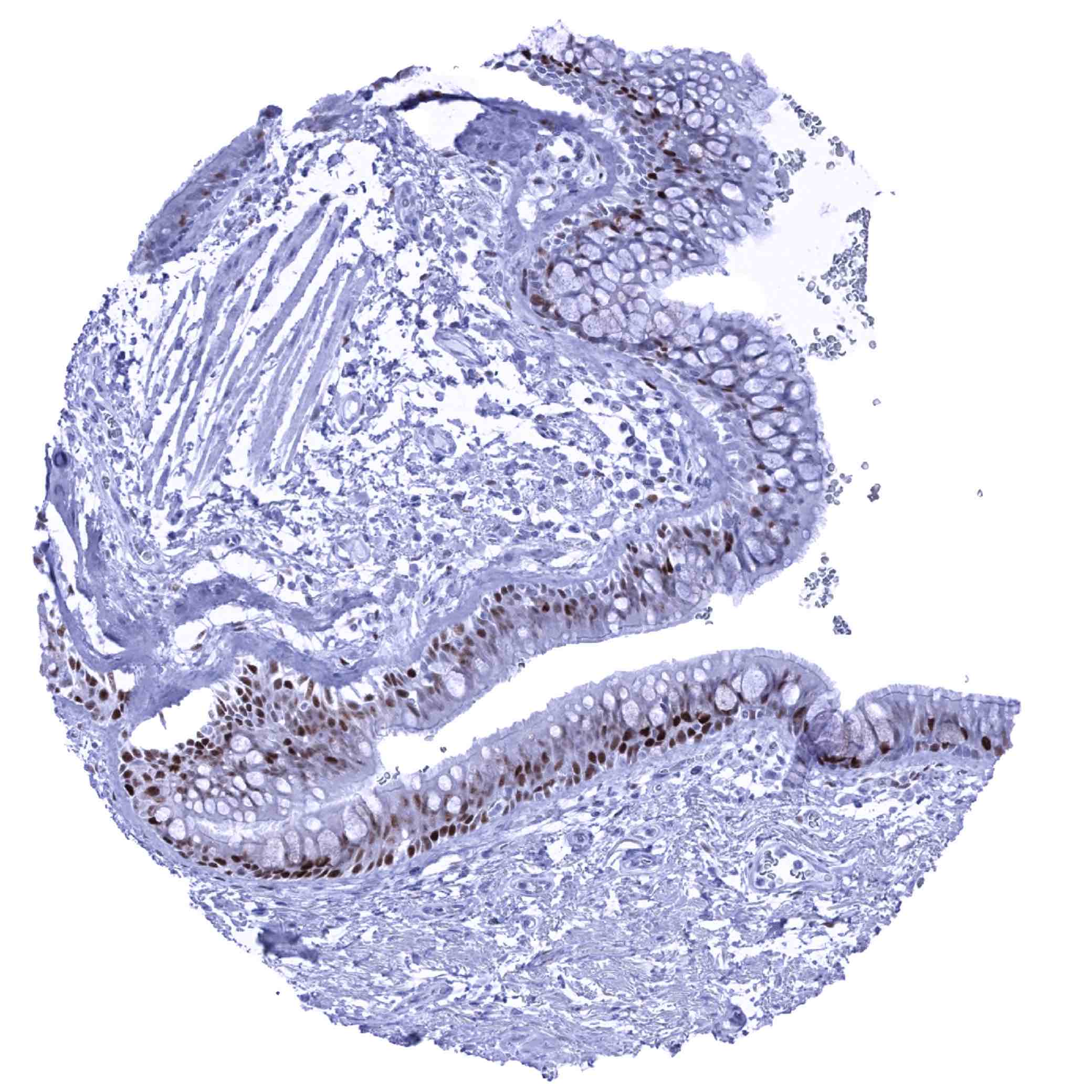
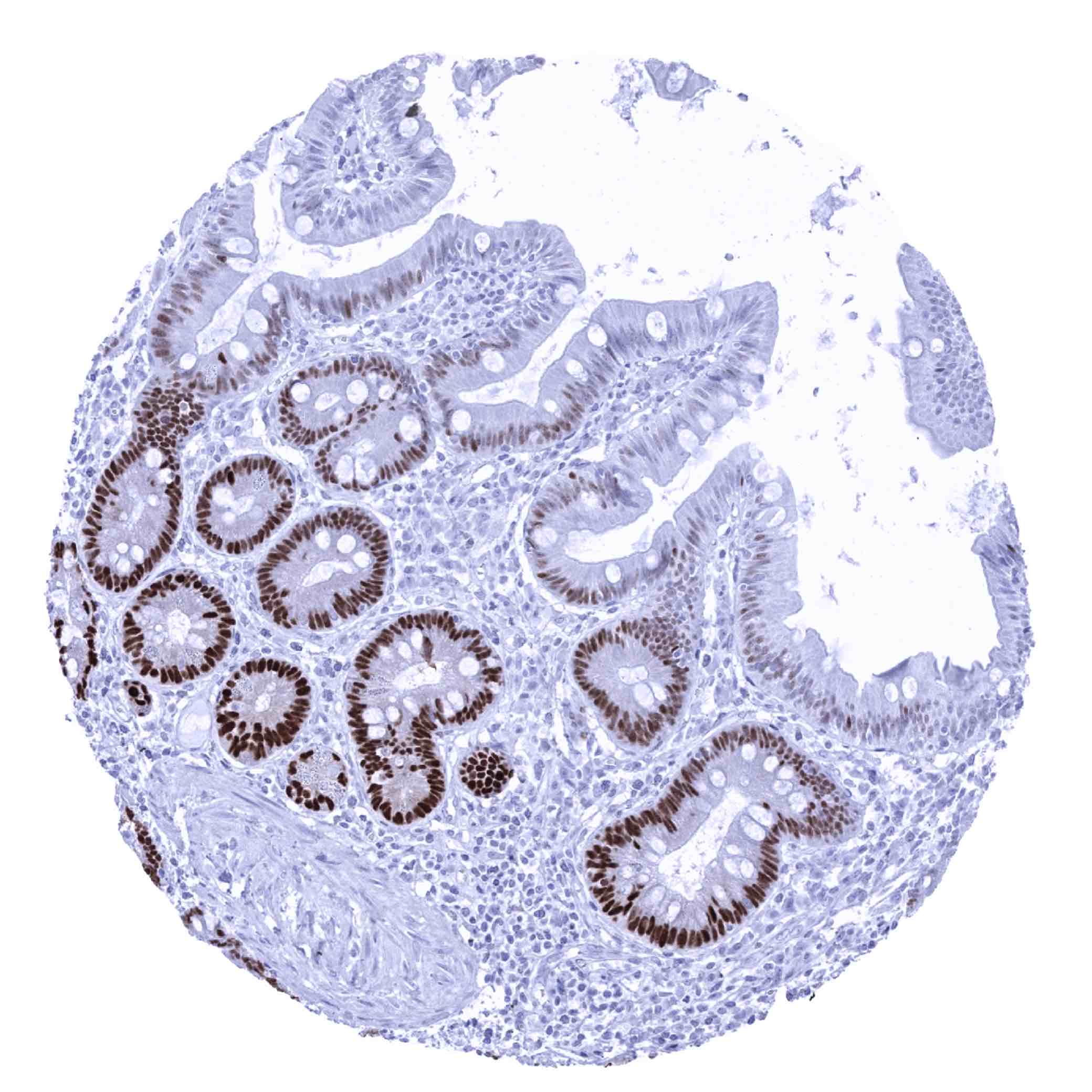
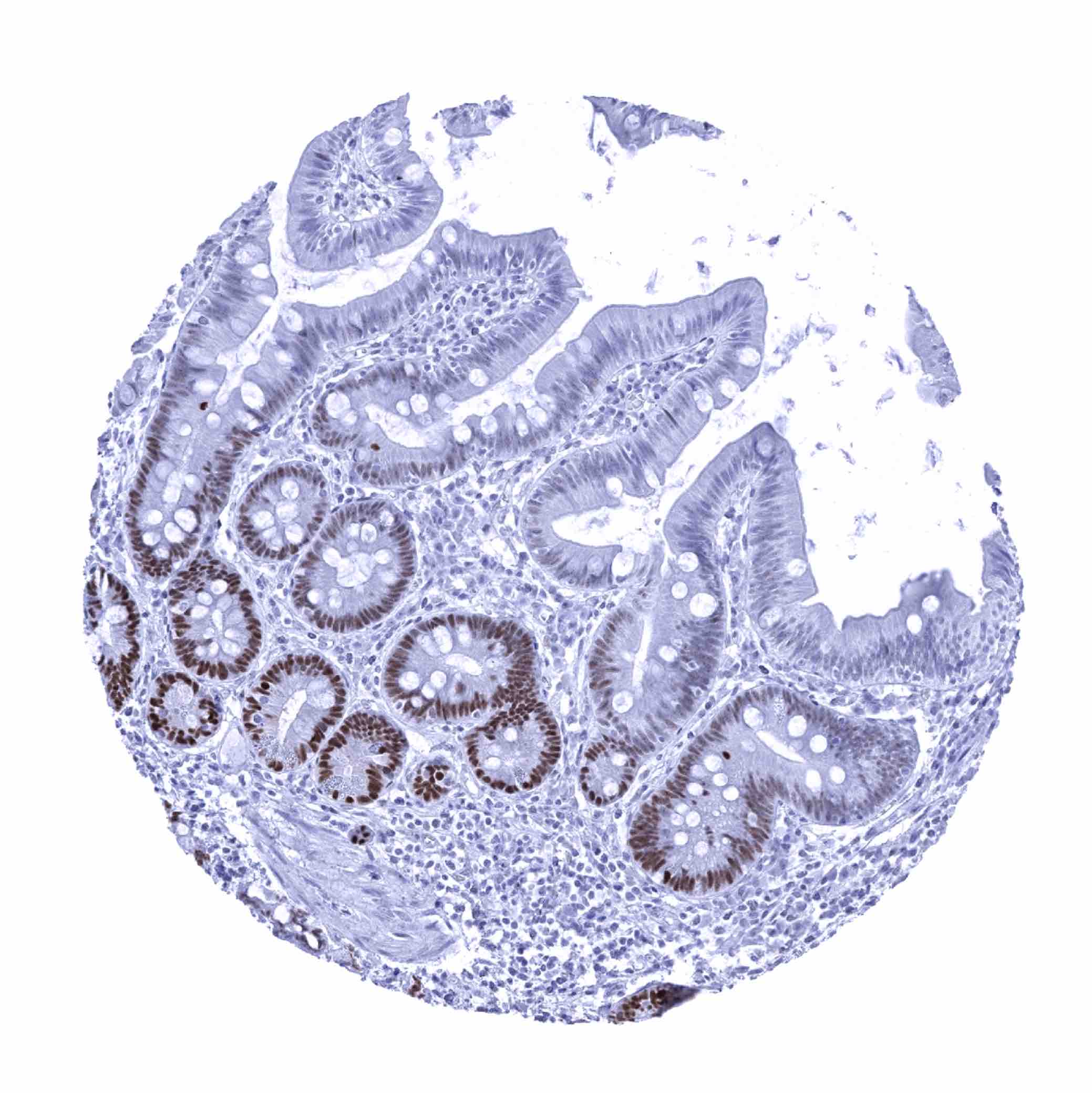
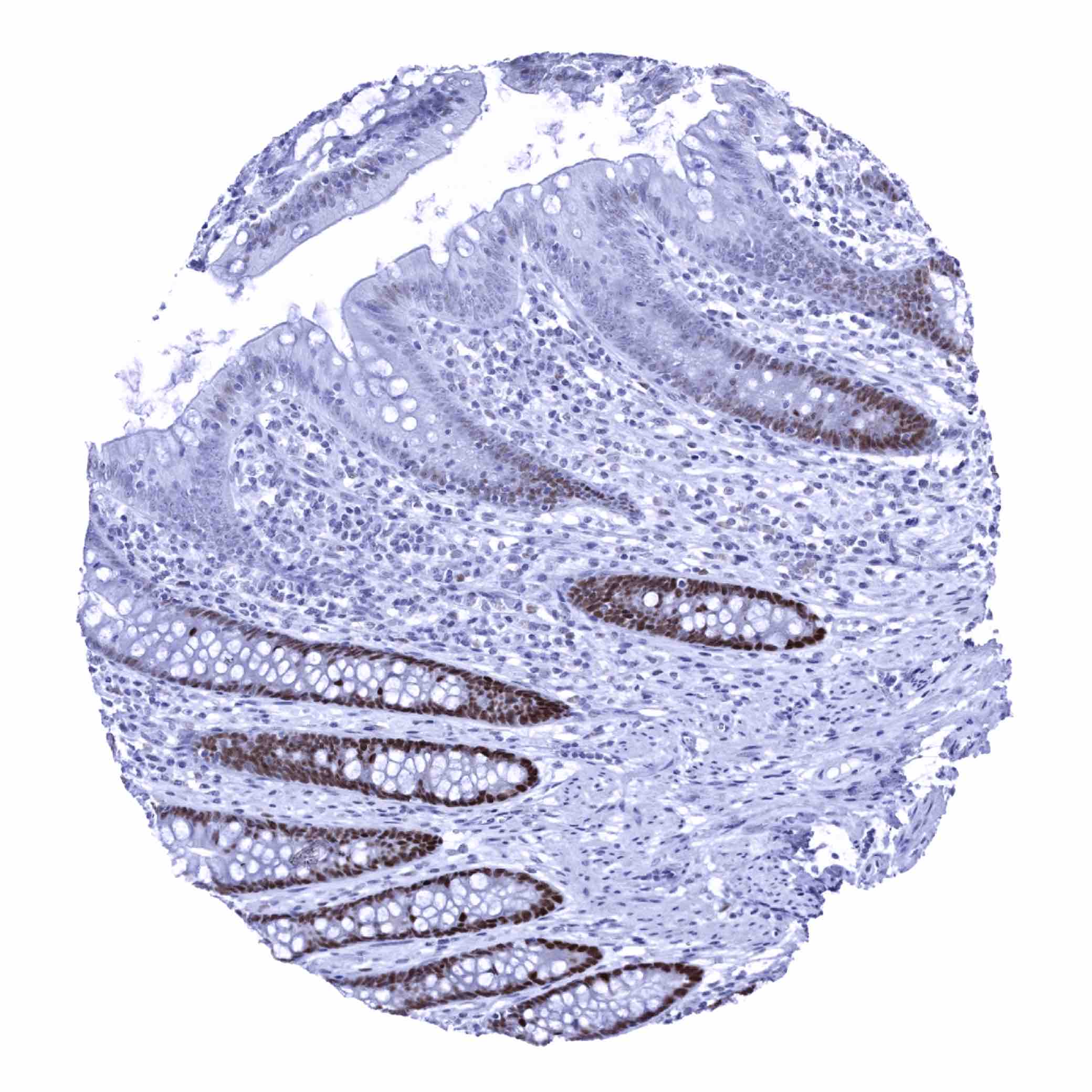
Positive control = Colon: A strong SOX9 immunostaining should be seen in epithelial cells of the crypt base.
Negative control = Colon: SOX9 immunostaining should be absent in all non-epithelial cell types (except few cells in lymphoid germinal centres – if present).
Cellular localization = Nucleus
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:50 – 1:75
Intended Use = Research Use Only
Relevance of Antibody
Biology Behind
SOX-9 is an kDa transcription factor protein coded by the SOX-9 gene on chromosome 17q24.
SOX-9 specifically recognizes the sequence CCTTGAG. SOX-9 is a regulatory element for the development of cells and tissues. It shows well-defined temporal and spatial expression patterns that differ between particular cell types and tissues and thus exerts a role in cell lineage restriction and terminal differentiation. For example, SOX-9 plays a pivotal role in differentiation of chondrocytes and in male sexual development. By interacting with multiple other genes, SOX-9 inhibits the creation of a female reproductive system. In several adult ectoderm- and endoderm-derived tissues, SOX-9 expression is retained in stem cell pools. SOX-9 is also believed to play a role in cancer stem cells.
Staining Pattern in Normal Tissues
SOX9 staining pattern in Normal Tissues with antibody MSVA-709R (Images shown in our “Normal Tissue Gallery”)
| Brain | Cerebrum | Negative*. |
| Cerebellum | Negative*. | |
| Endocrine Tissues | Thyroid | Moderate to strong SOX9 positivity of follicular cells. |
| Parathyroid | Negative. | |
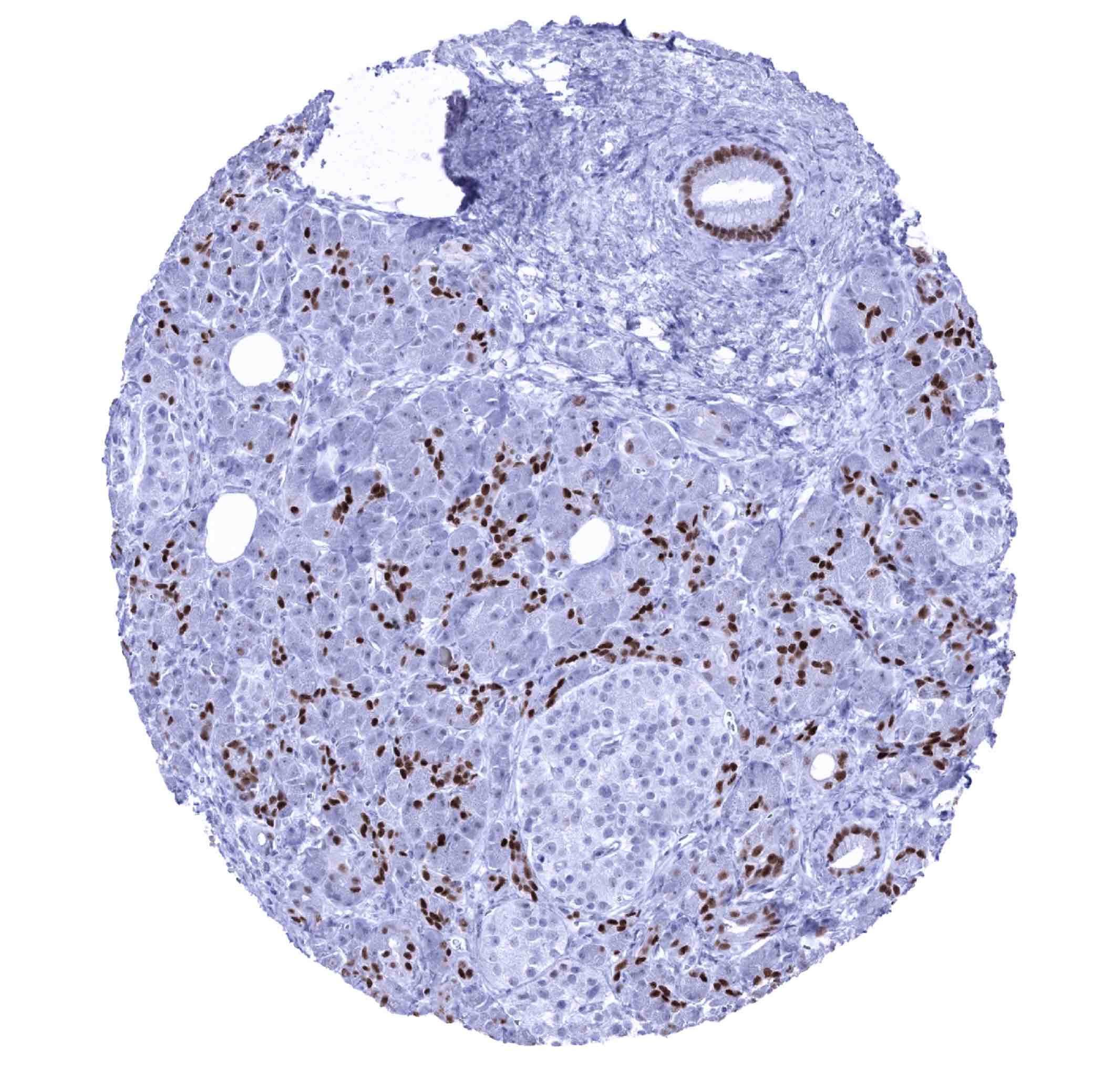
| Adrenal gland | Few interspersed cells in the cortex showing weak to moderate SOX9 positivity. | |
| Pituitary gland | ||
| Respiratory system | Respiratory epithelium | Moderate to strong SOX9 positivity of most epithelial cells. |
| Lung | Pneumocytes and alveolar cells are SOX9 negative. | |
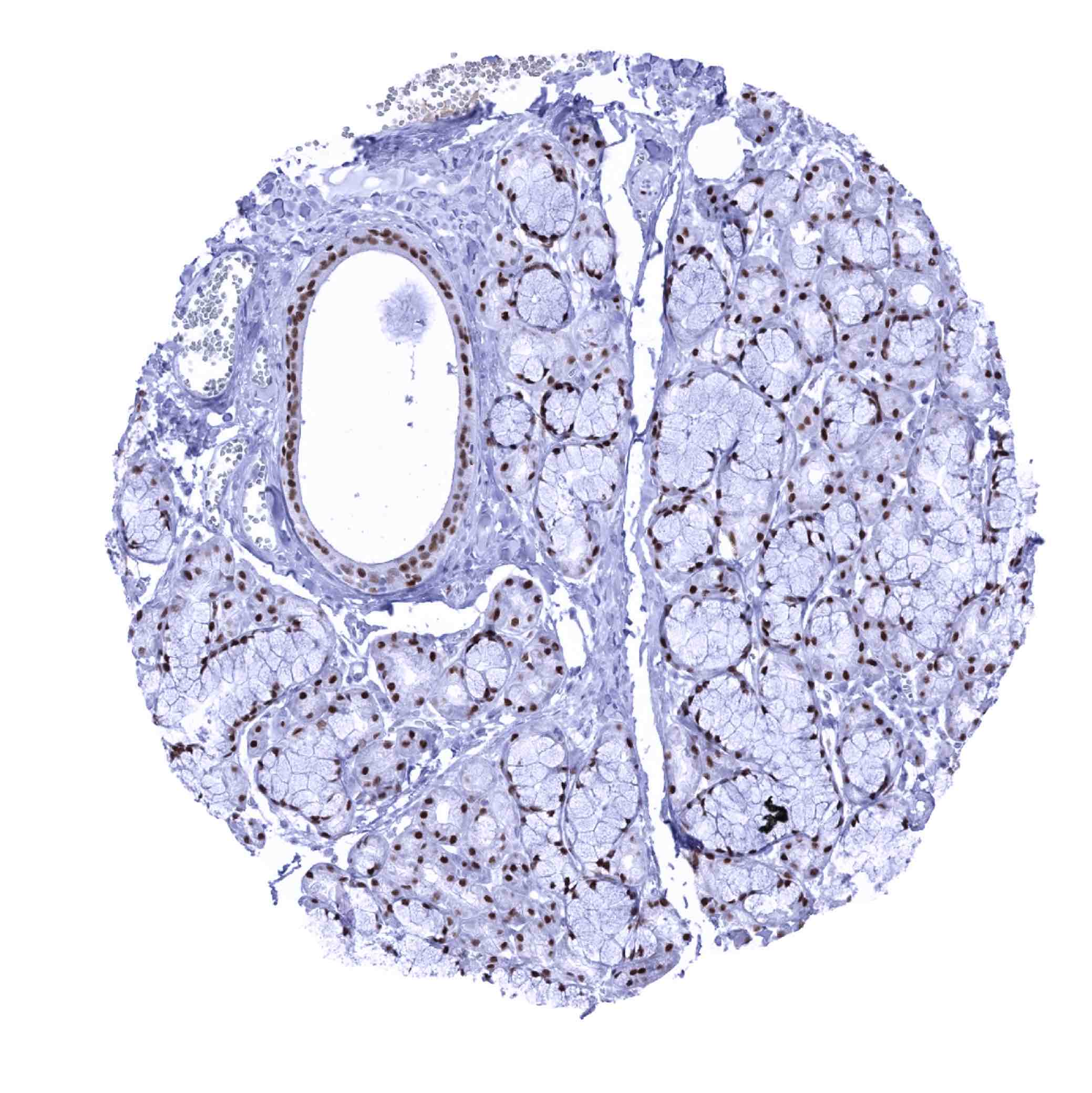
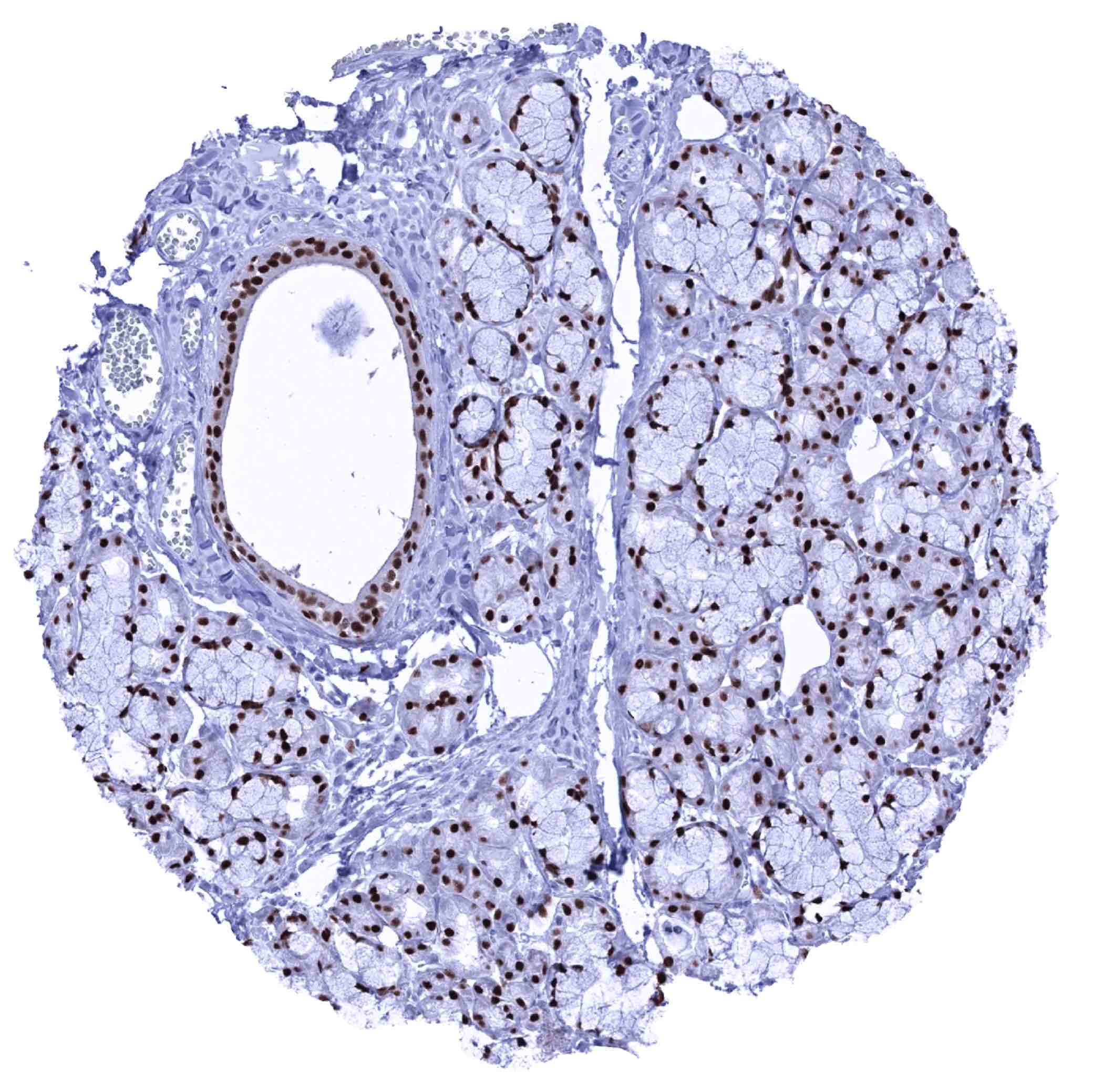
| Gastrointestinal Tract | Salivary glands | Moderate to strong nuclear SOX9 staining of all epithelial cell types. |
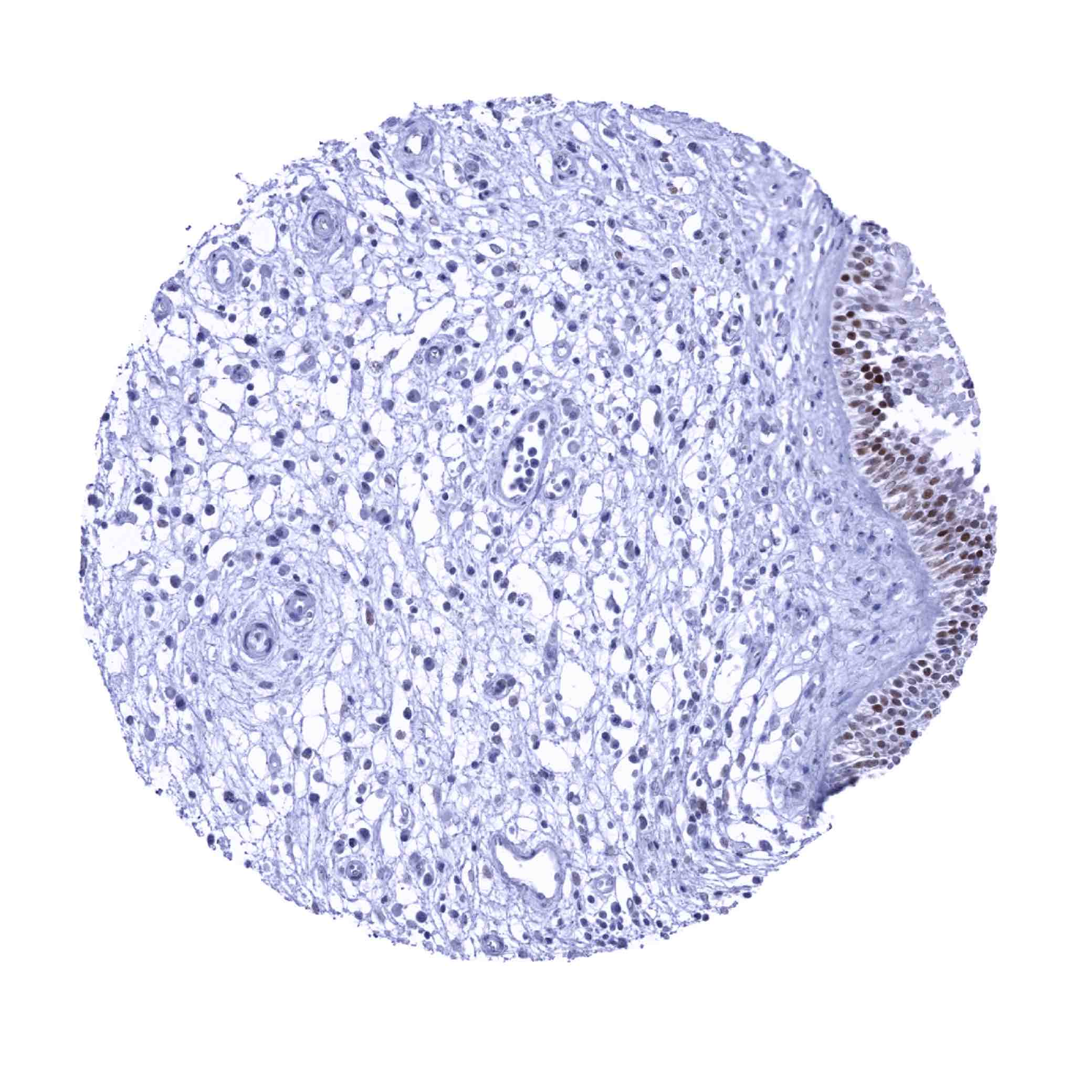
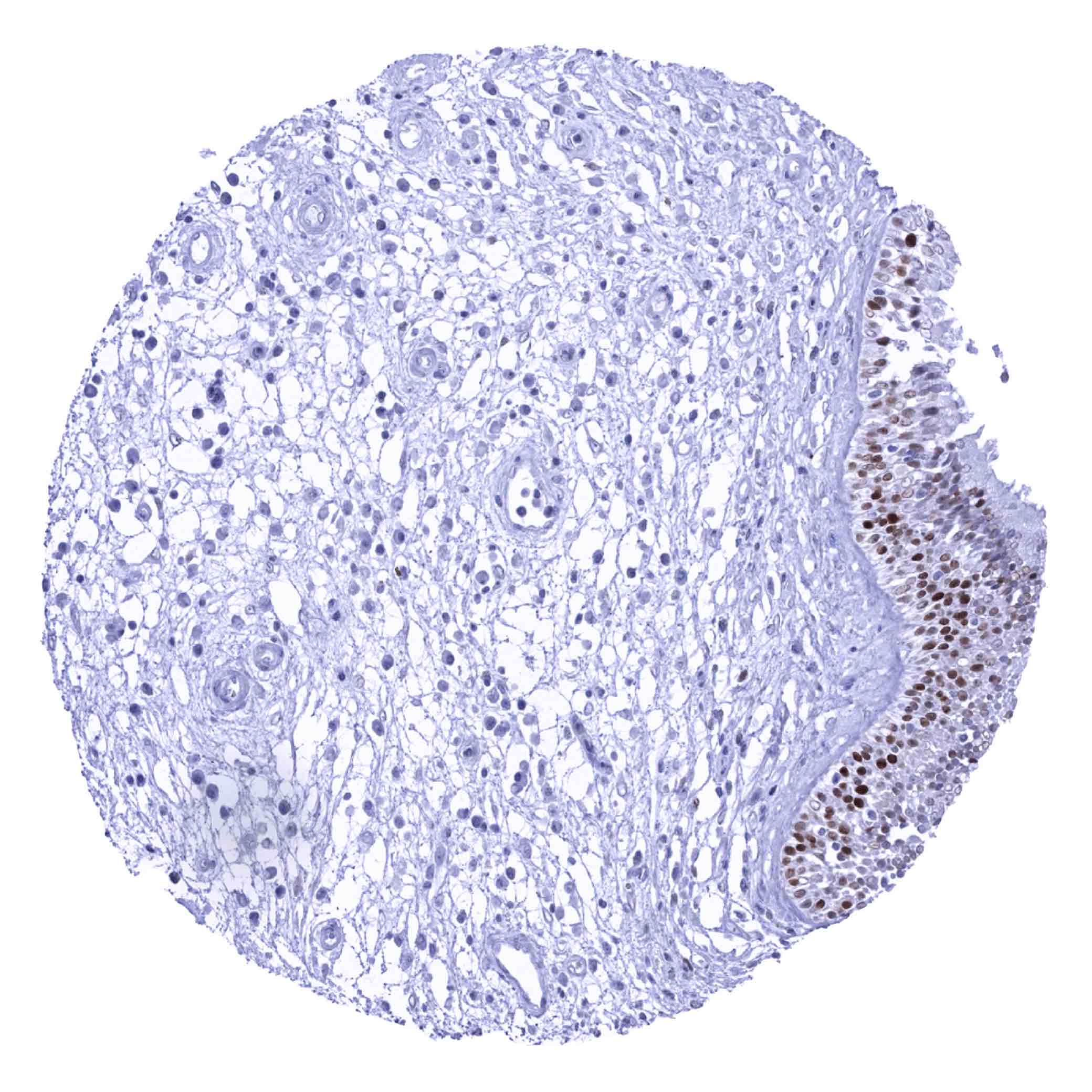
| Esophagus | Weak to moderate nuclear SOX9 staining of the bottom 2/3 of squamous epithelium. | |
| Stomach | Moderate to strong nuclear SOX9 staining of surface epithelial cells, while the glandular cells are either SOX9 negative or only show weak positivity. | |
| Duodenum | Strong nuclear SOX9 staining of crypt epithelial cells. The SOX9 staining intensity markedly decreases towards the surface epithelium and the tips of the villosities remain SOX9 negative. Strong SOX9 staining of Brunner gland cells. | |
| Small intestine | Strong nuclear SOX9 staining of crypt epithelial cells. The SOX9 staining intensity markedly decreases towards the surface epithelium and the tips of the villosities remain SOX9 negative. | |
| Appendix | Strong nuclear SOX9 staining of crypt epithelial cells, especially at the base. SOX9 staining intensity gradually decreases towards the surface. The surface epithelium remains SOX9 negative (or shows only a very weak staining). | |
| Colon | Strong nuclear SOX9 staining of crypt epithelial cells, especially at the base. SOX9 staining intensity gradually decreases towards the surface. The surface epithelium remains SOX9 negative (or shows only a very weak staining). | |
| Rectum | Strong nuclear SOX9 staining of crypt epithelial cells, especially at the base. SOX9 staining intensity gradually decreases towards the surface. The surface epithelium remains SOX9 negative (or shows only a very weak staining). | |
| Liver | Moderate to strong nuclear SOX9 staining of intrahepatic bile ducts. | |
| Gallbladder | Strong nuclear SOX9 staining of epithelial cells. | |
| Pancreas | Strong nuclear SOX9 staining of intercalated ducts and of excretory ducts, while acinar cells are negative or weakly positive and islet cells are SOX9 negative.
|
|
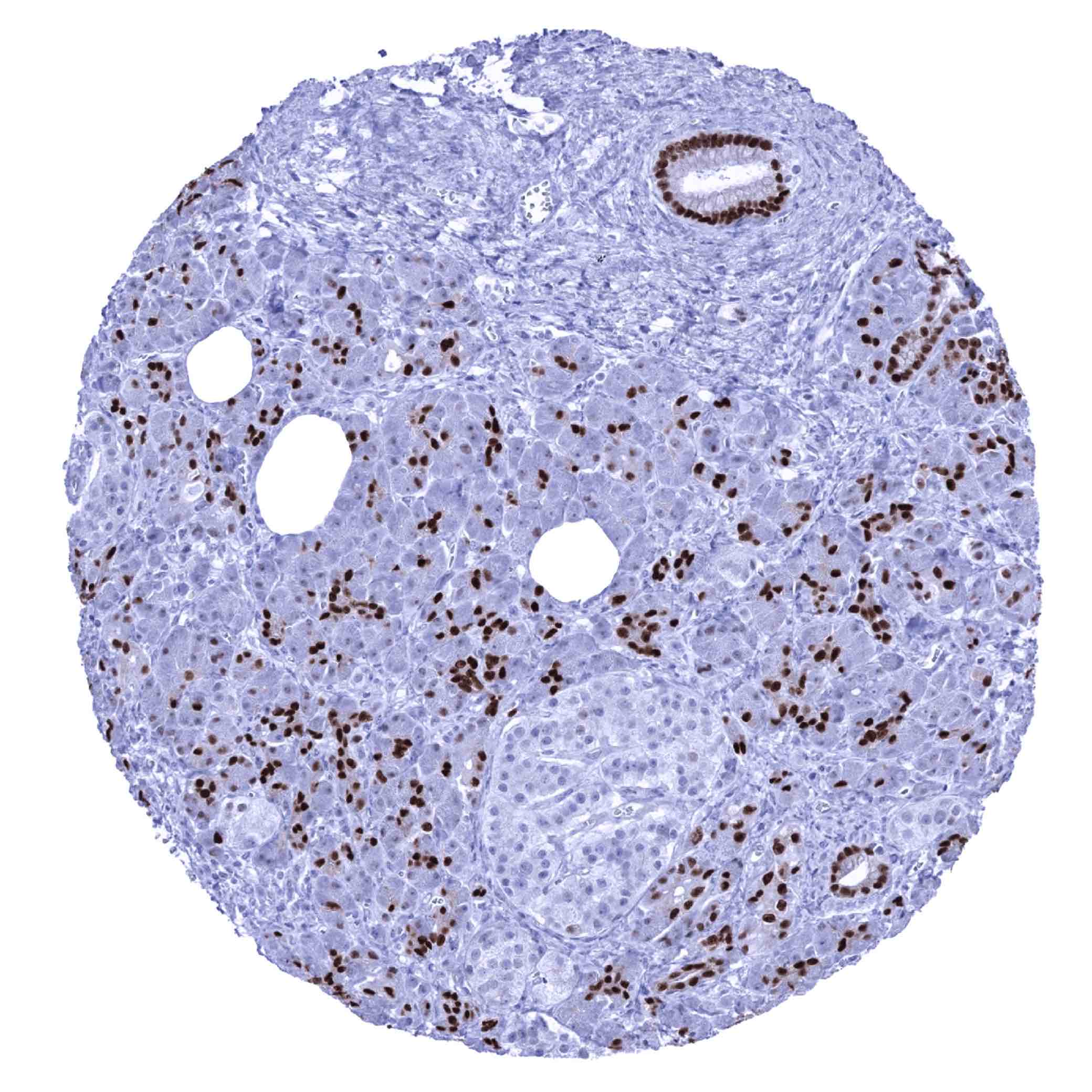
| Genitourinary | Kidney | The strongest SOX9 staining is seen in the collecting ducts (moderate to strong staining of a subset of cells) while only few cells of the tubuli may show a weak to moderate SOX9 staining. |
| Urothelium | A weak SOX9 staining can occur in the superficial cell layers (umbrella cells) of the urothelium. | |
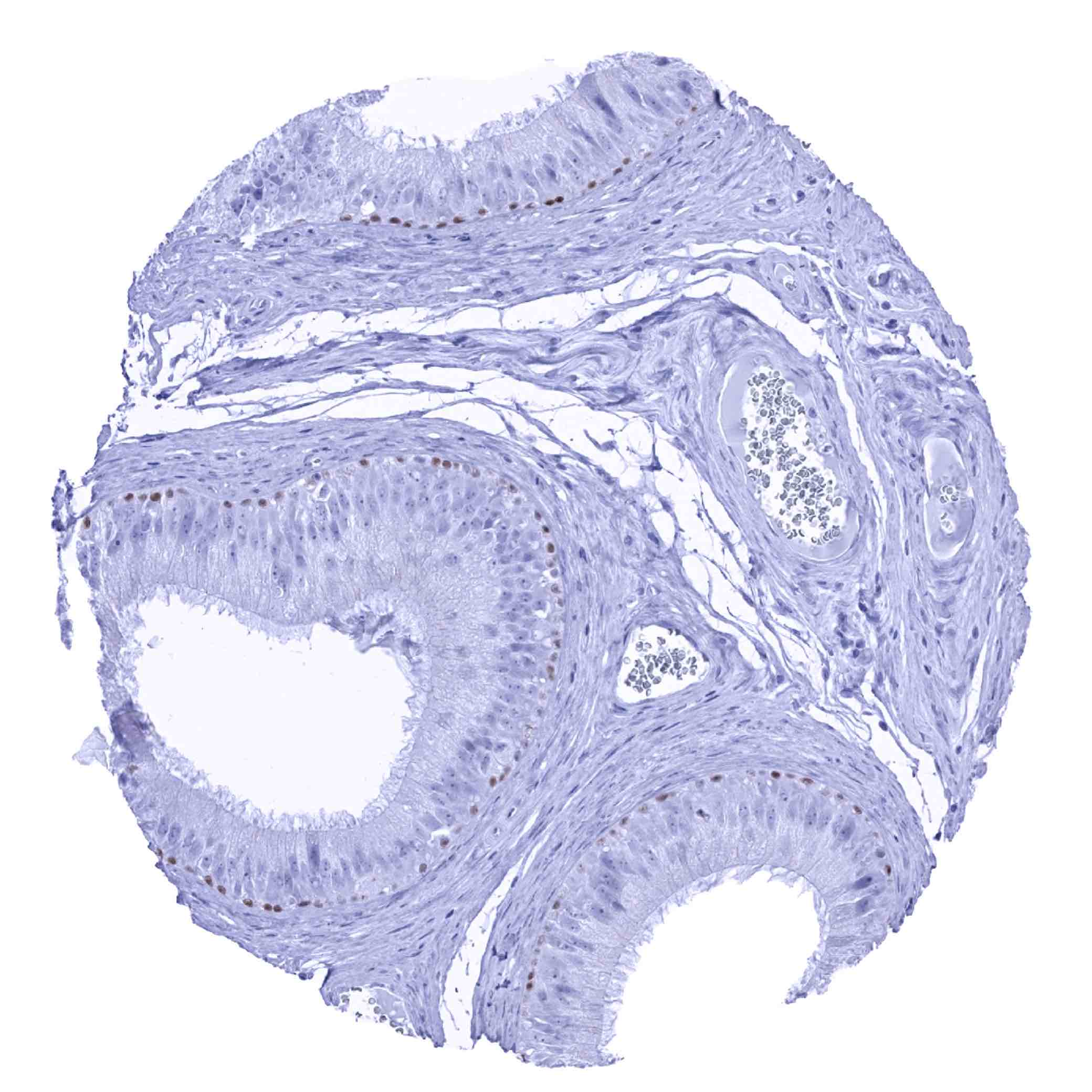
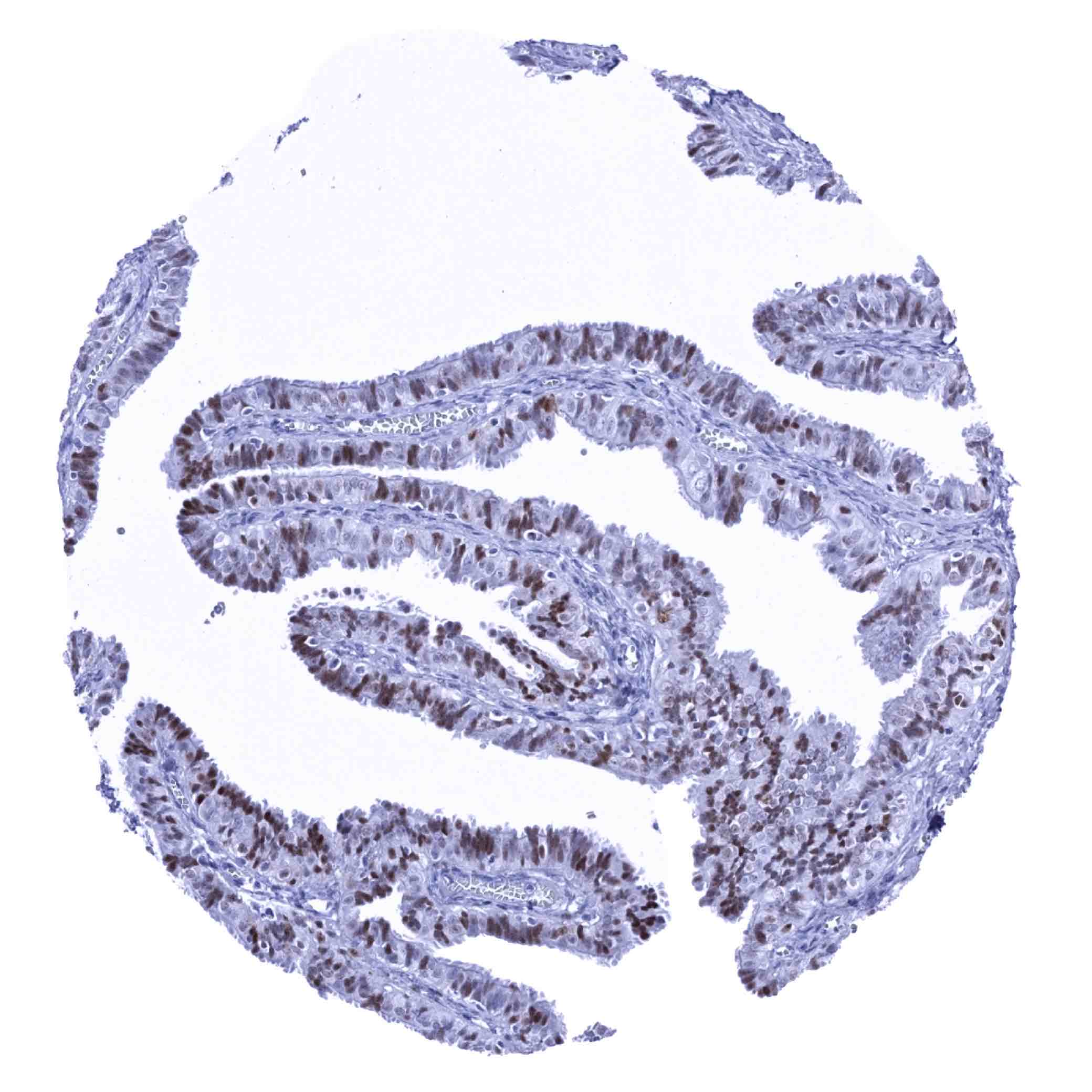
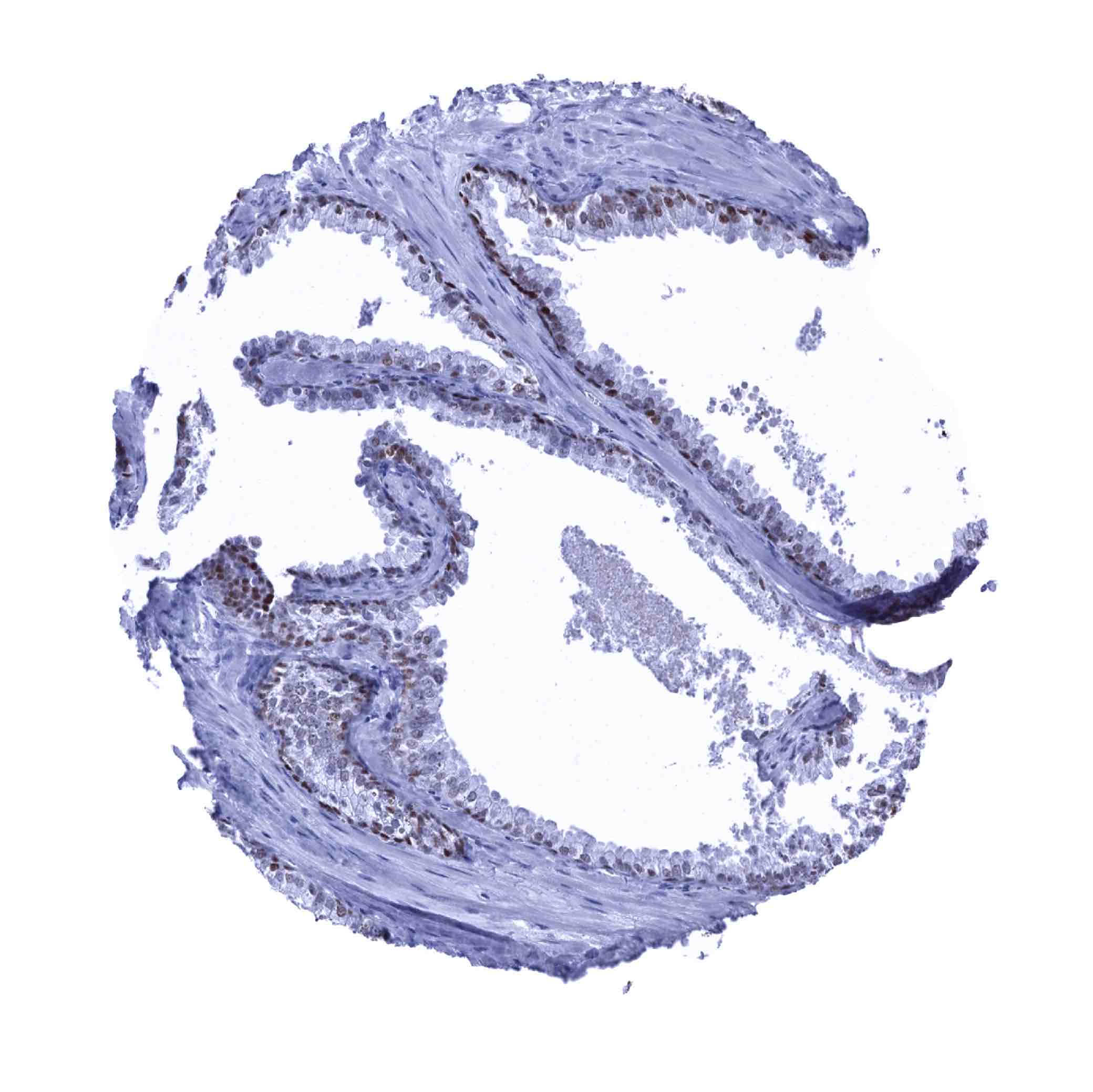
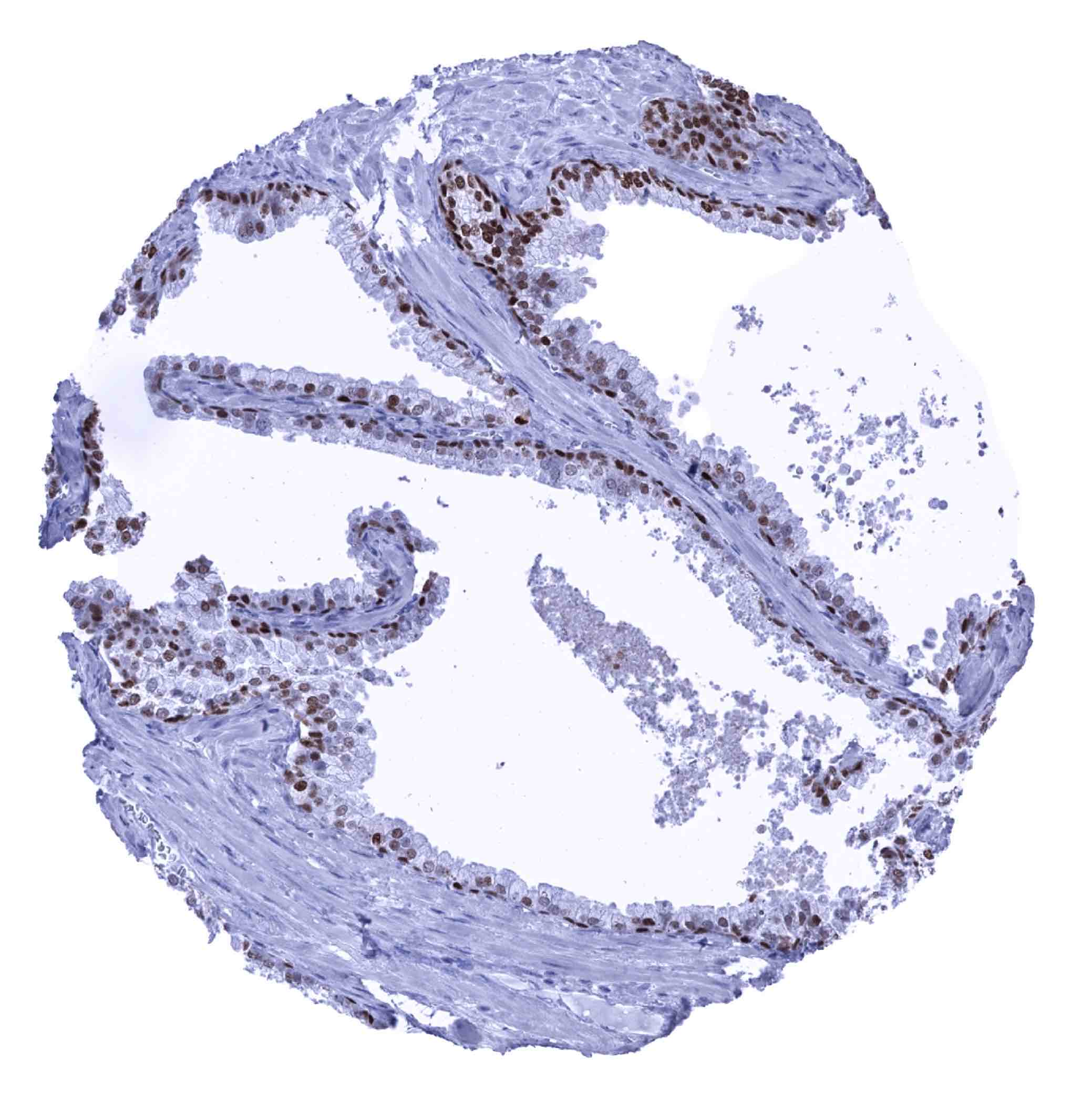
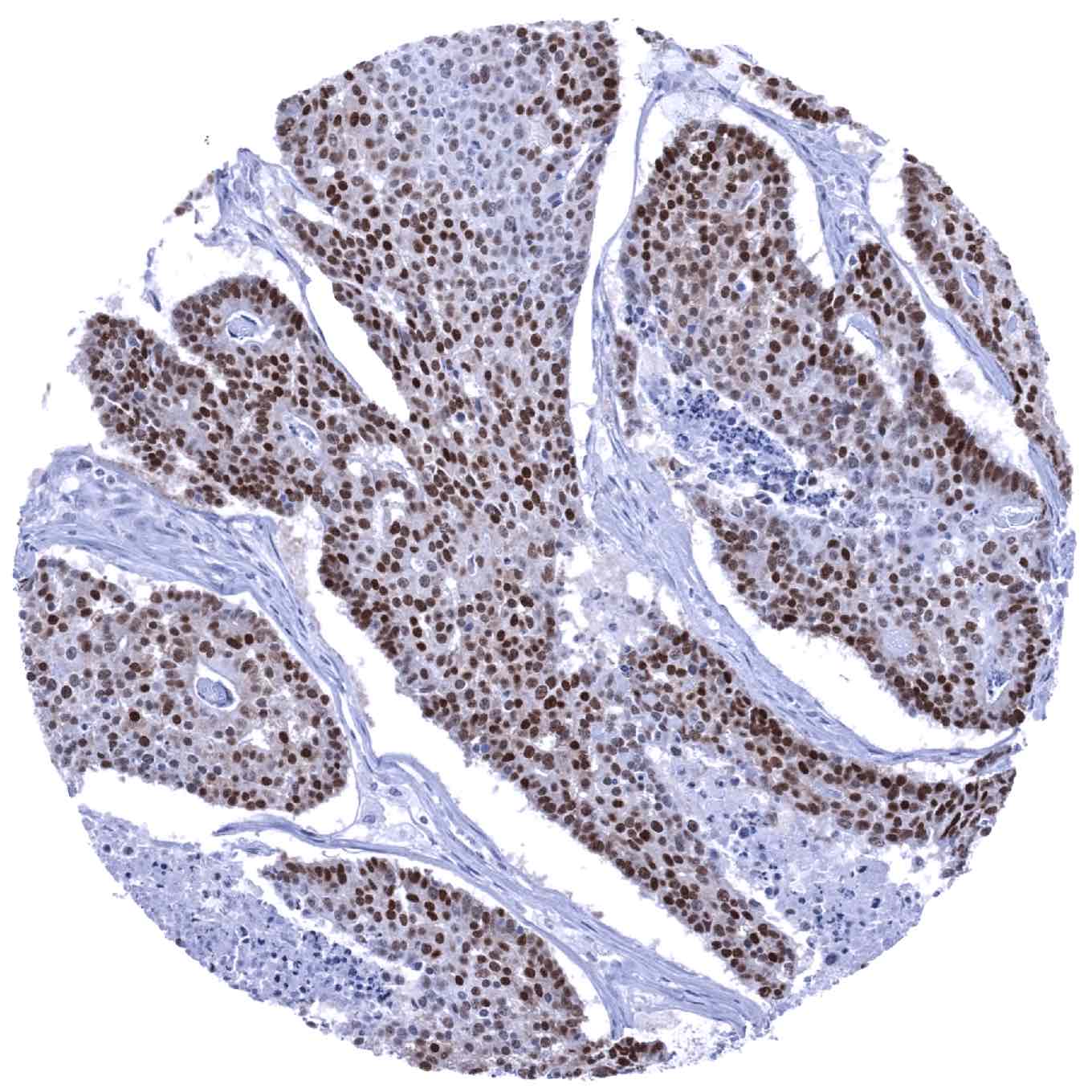
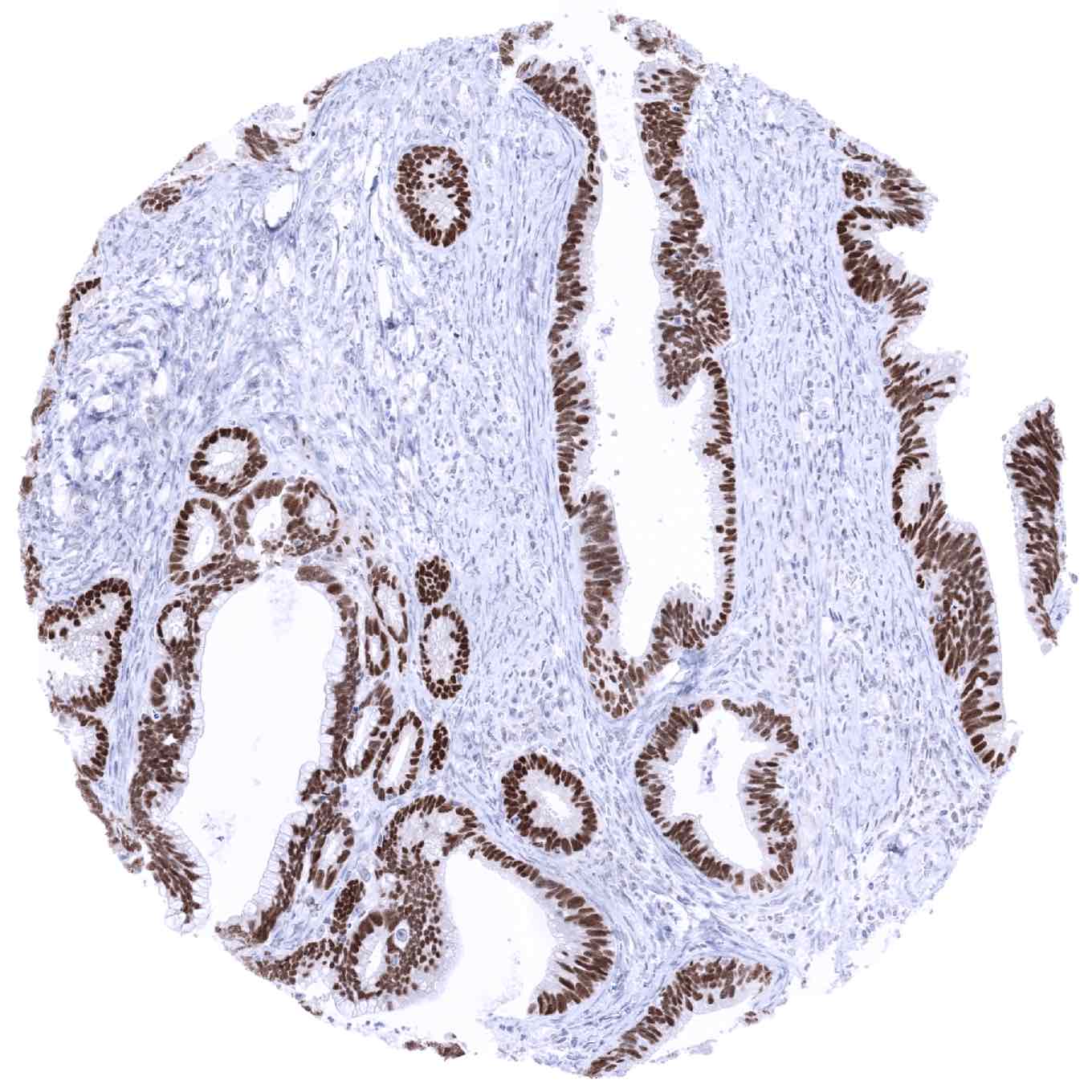
| Male genital | Prostate | Strong SOX9 positivity of basal cells while luminal cells show only a markedly weaker staining. |
| Seminal vesicles | Moderate to strong SOX9 positivity of epithelial cells. | |
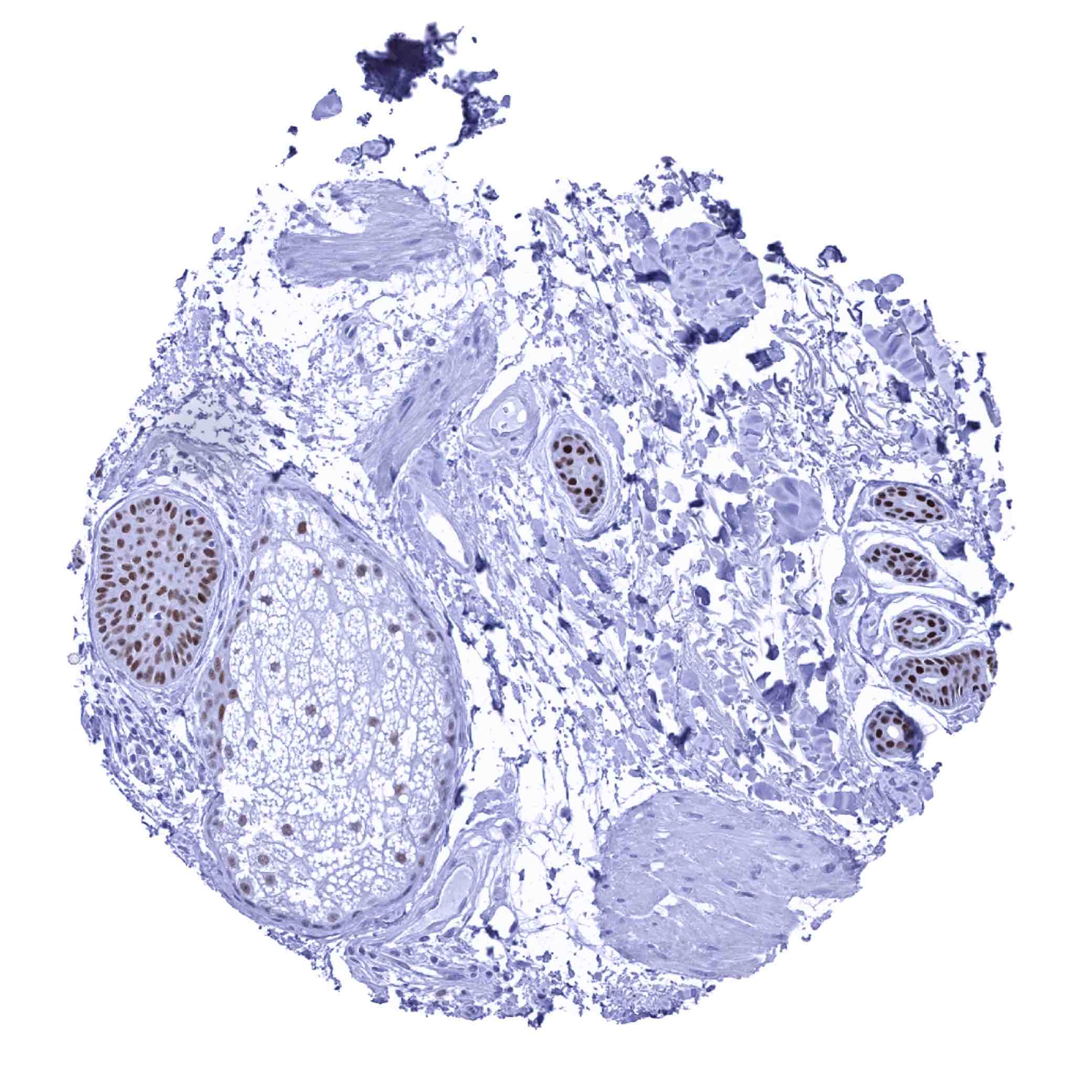
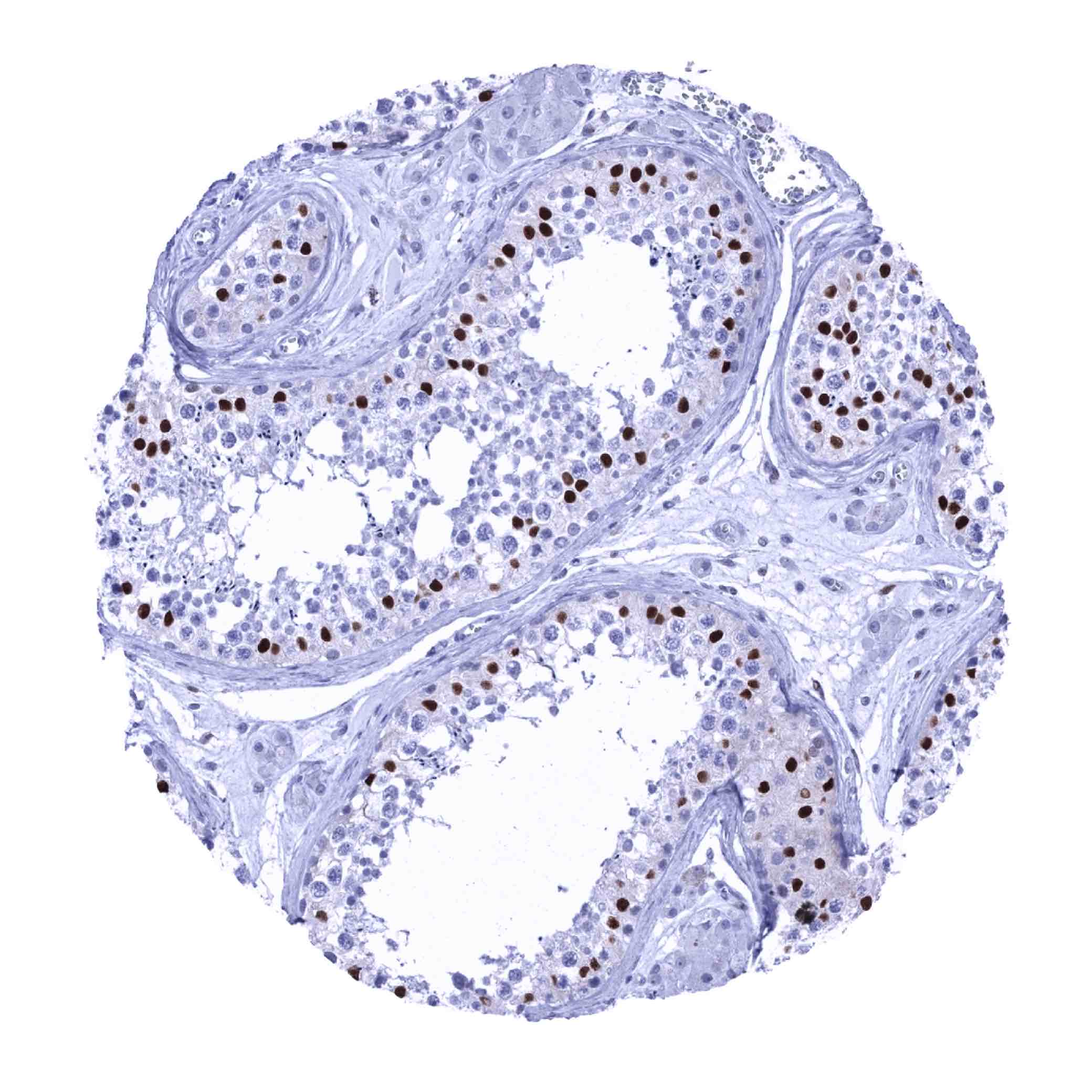
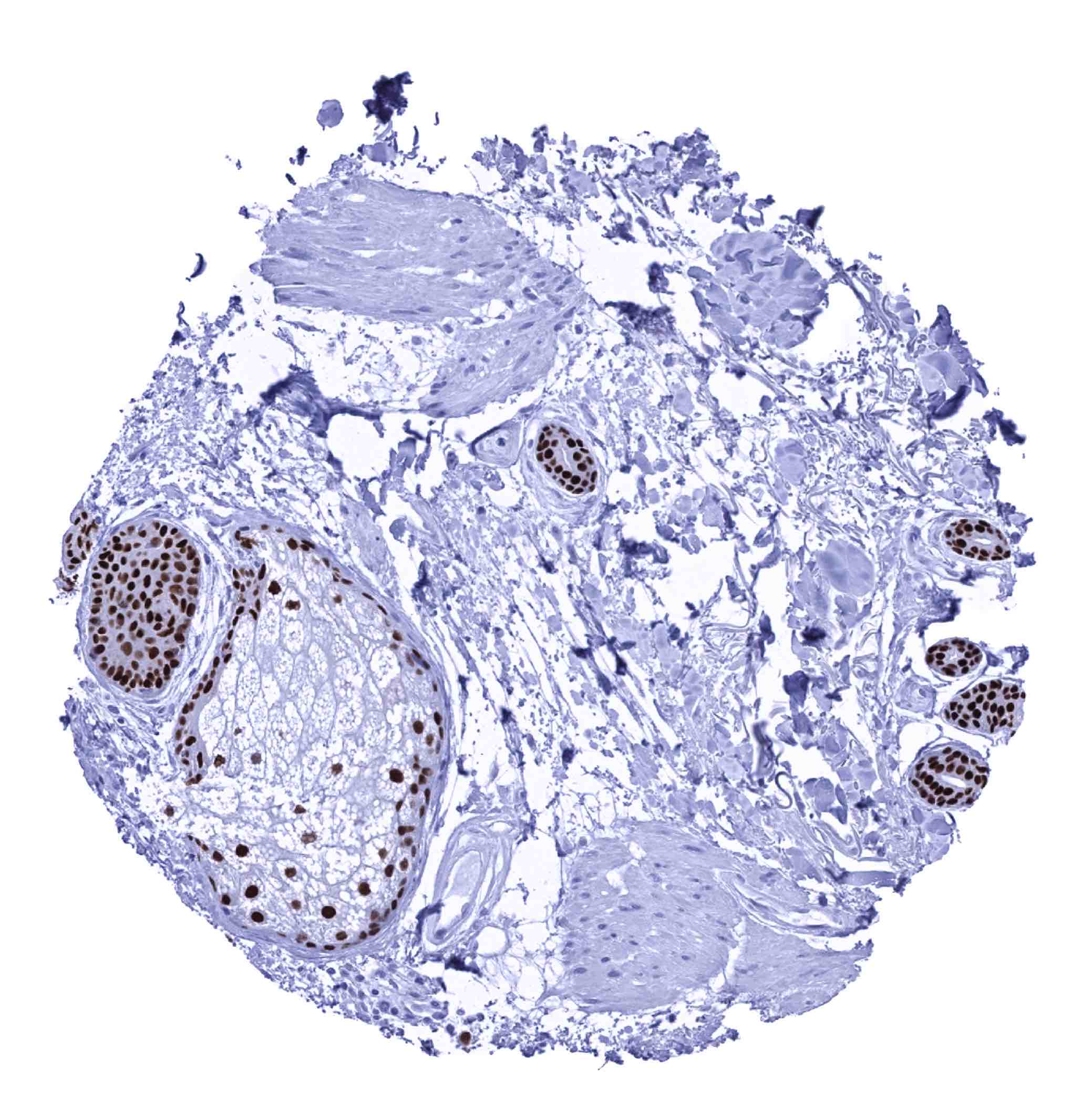
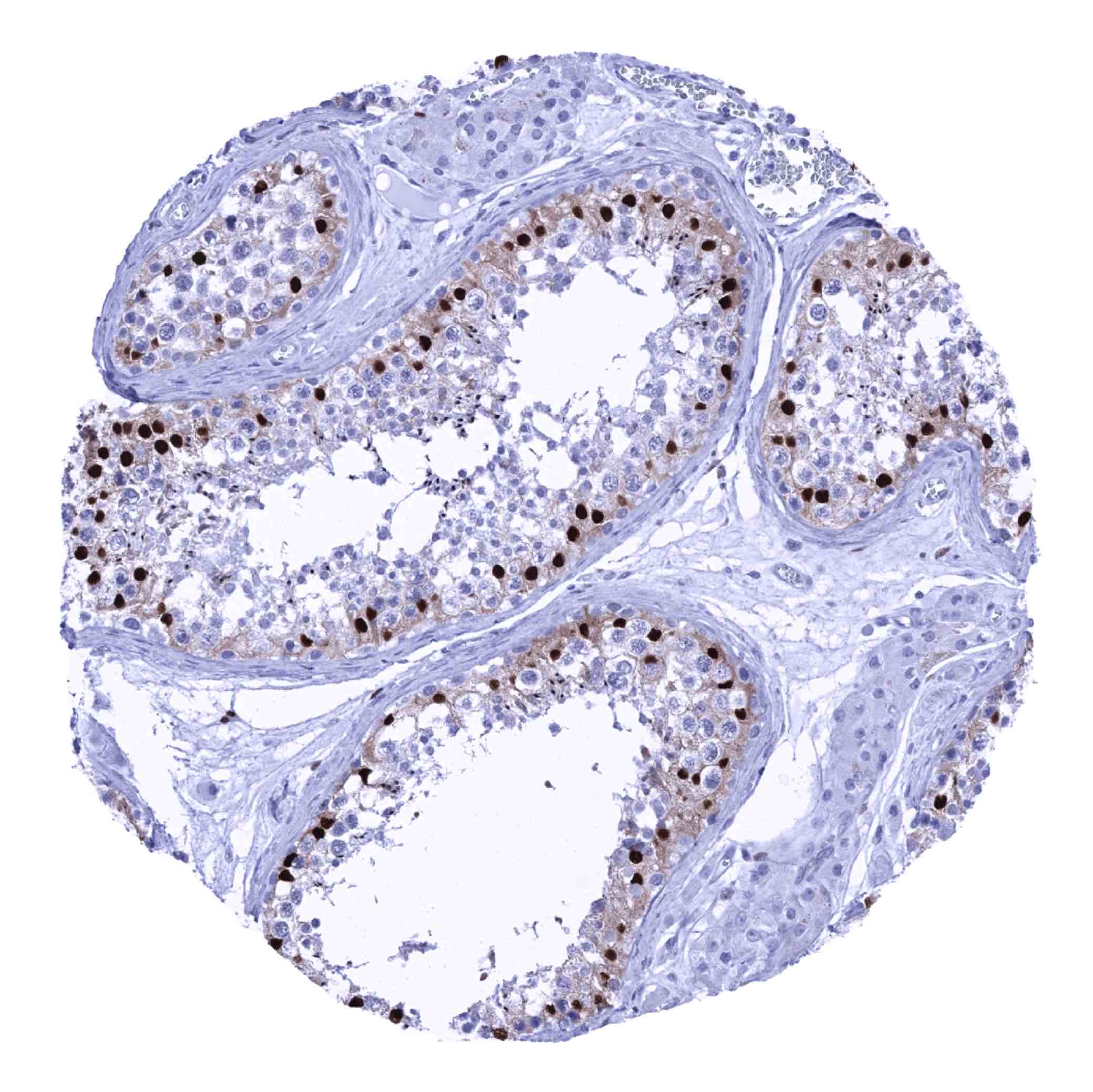
| Testis | Strong SOX9 staining of Sertoli cells. | |
| Epididymis | Weak to moderate nuclear SOX9 staining of basal cells in the caput. | |
| Female genital | Breast | Epithelial cells are largely SOX9 negative or may show faint staining. |
| Uterus, myometrium | Negative. | |
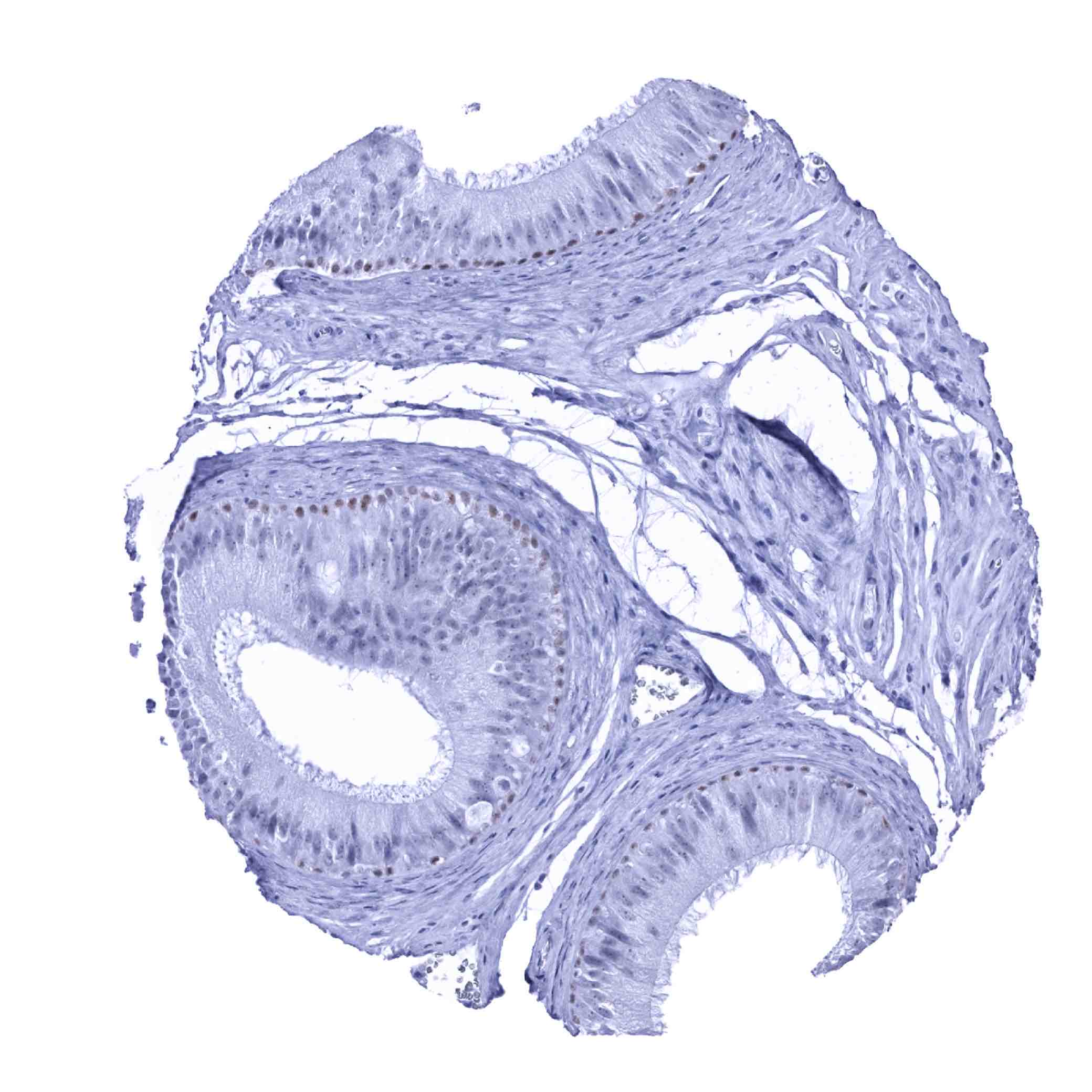
| Uterus, ectocervix | Weak to moderate nuclear SOX9 staining of the bottom 2/3 of squamous epithelium. | |
| Uterus endocervix | Weak nuclear SOX9 staining of epithelial cells. | |
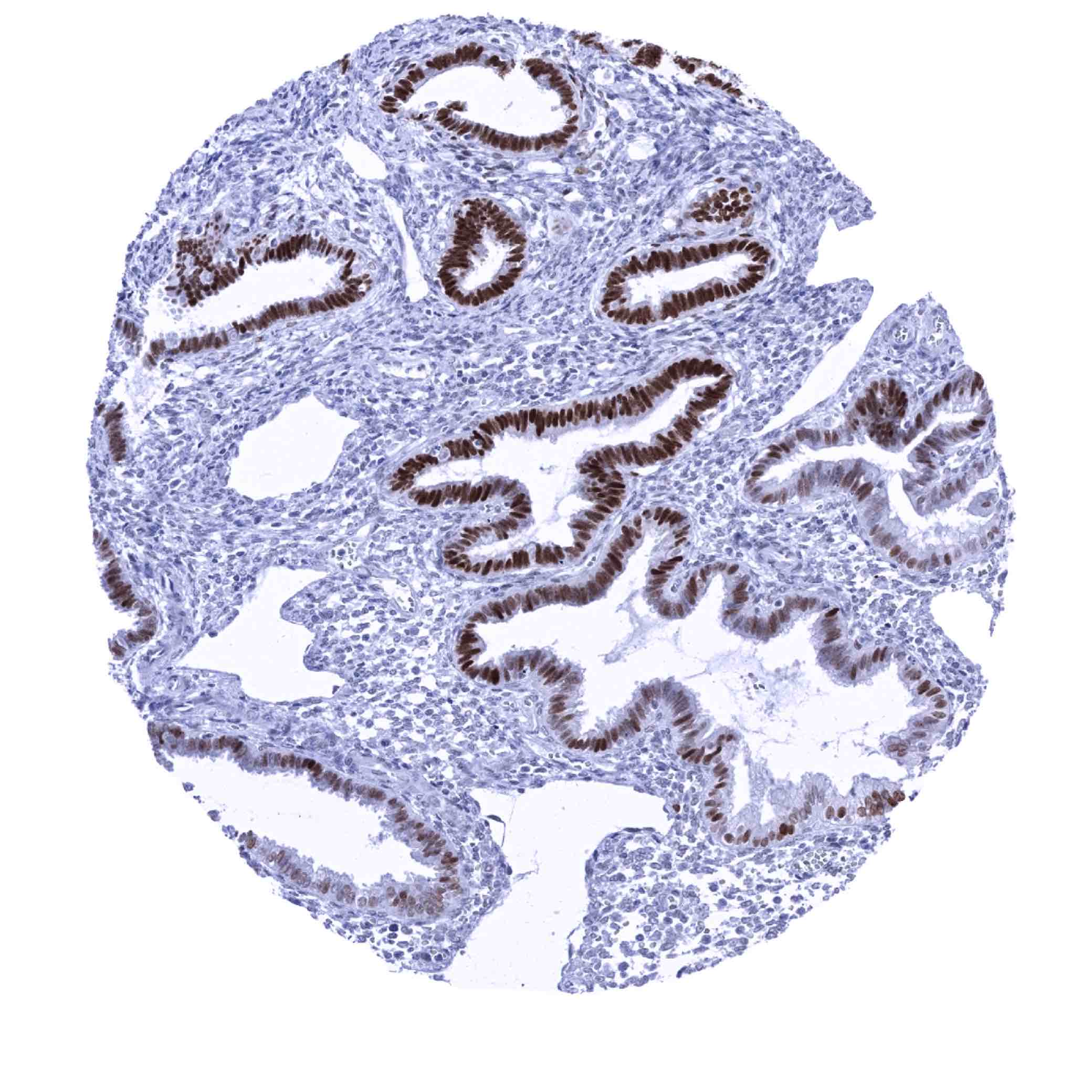
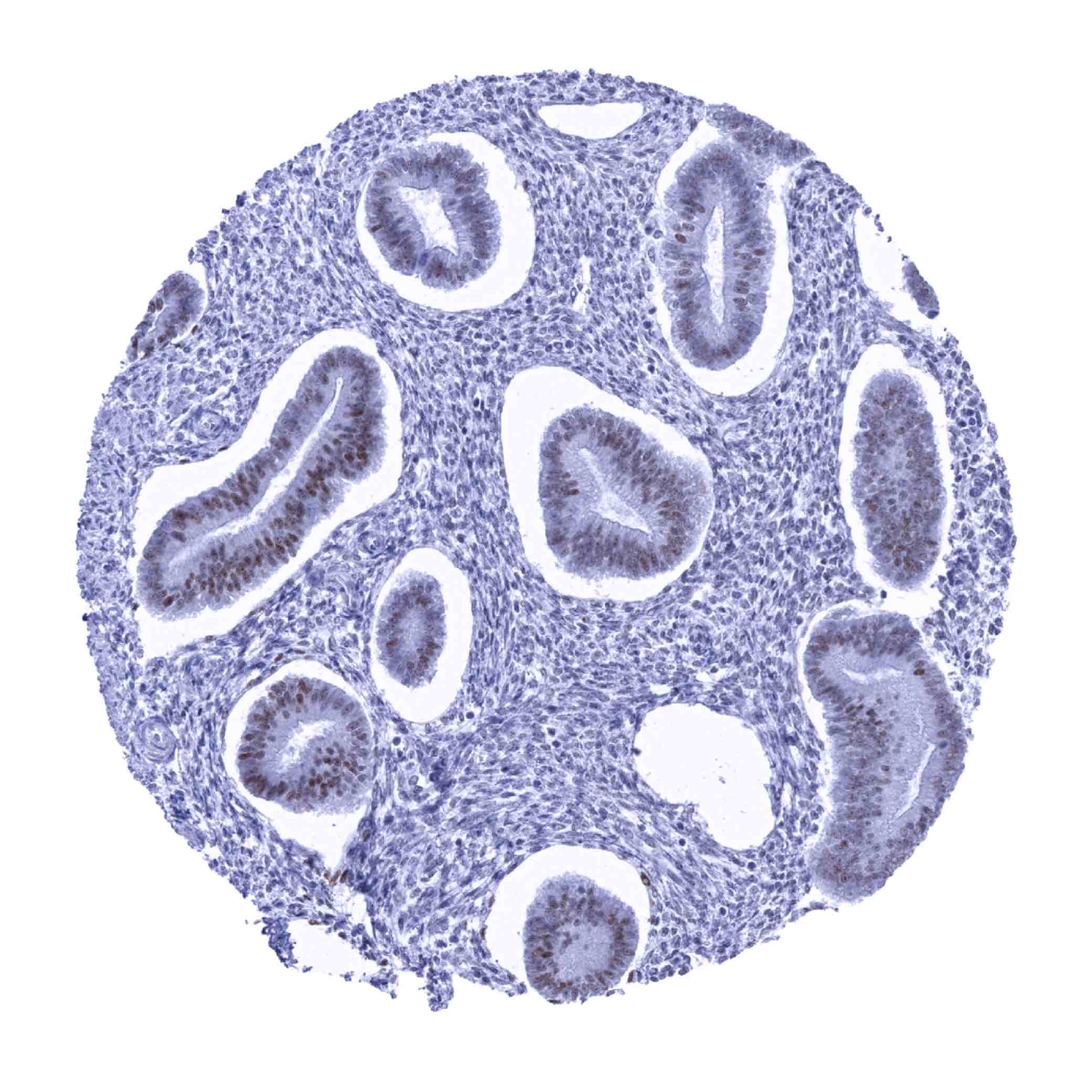
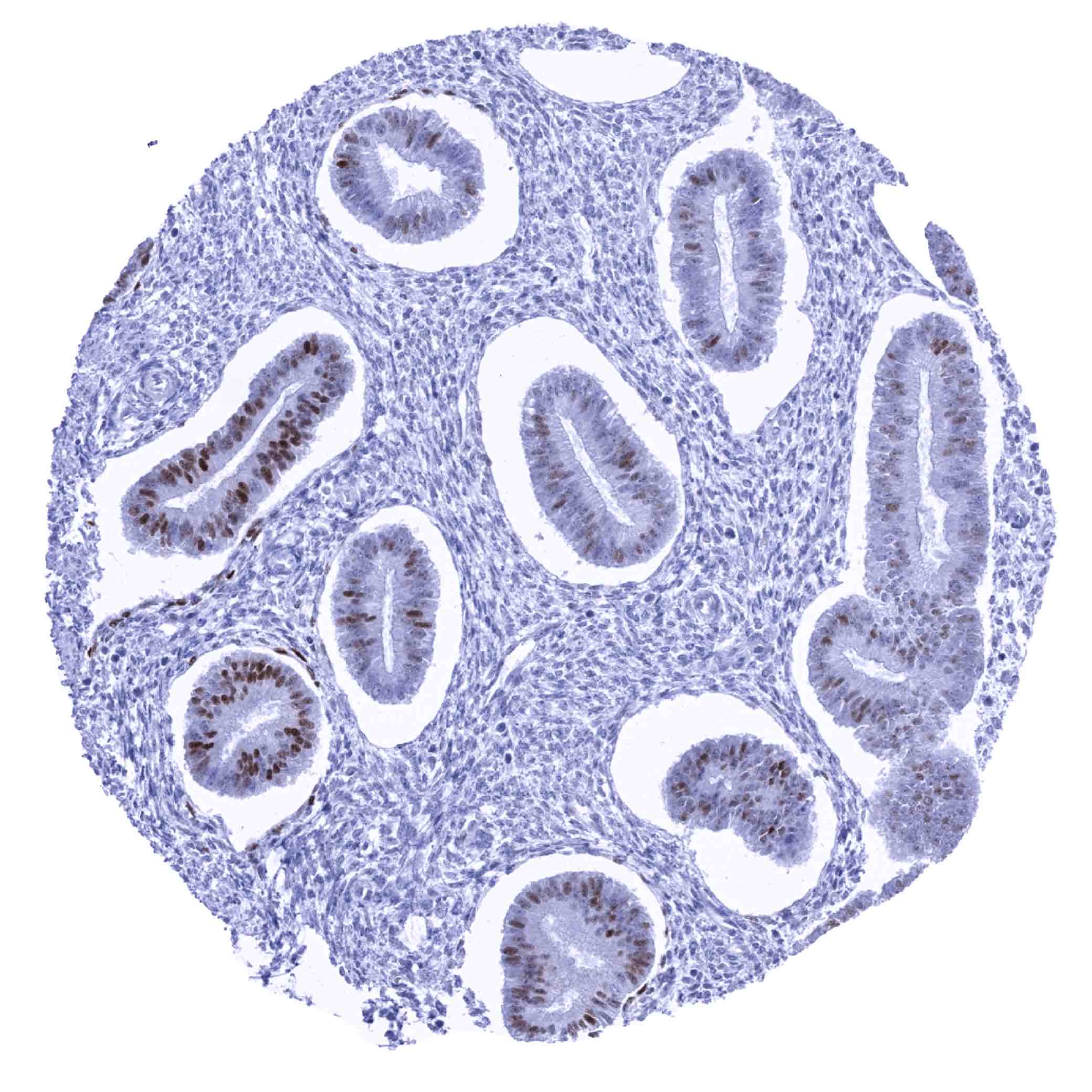
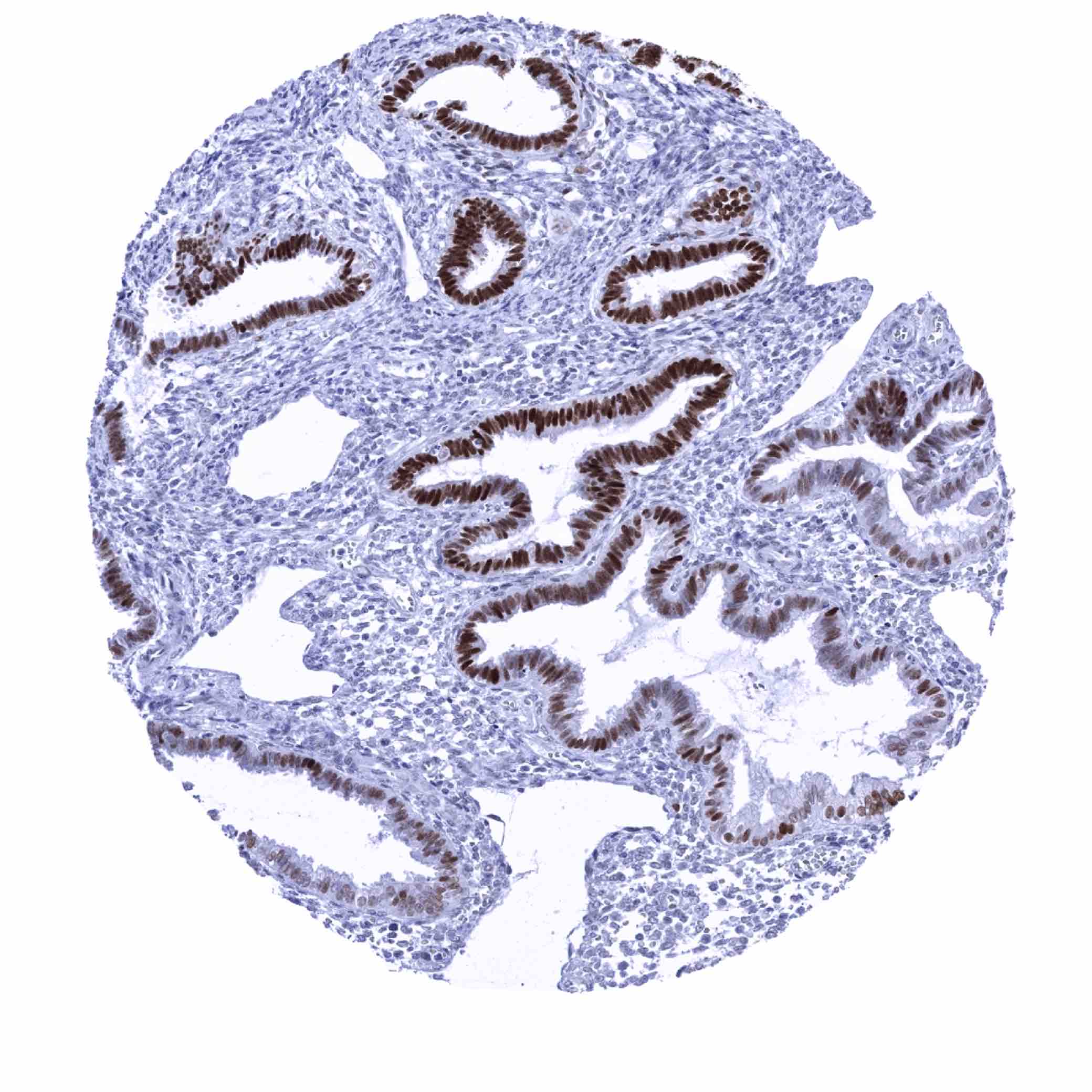
| Uterus, endometrium | Moderate to strong SOX9 positivity of epithelial cells. Stroma cells are SOX9 negative. | |
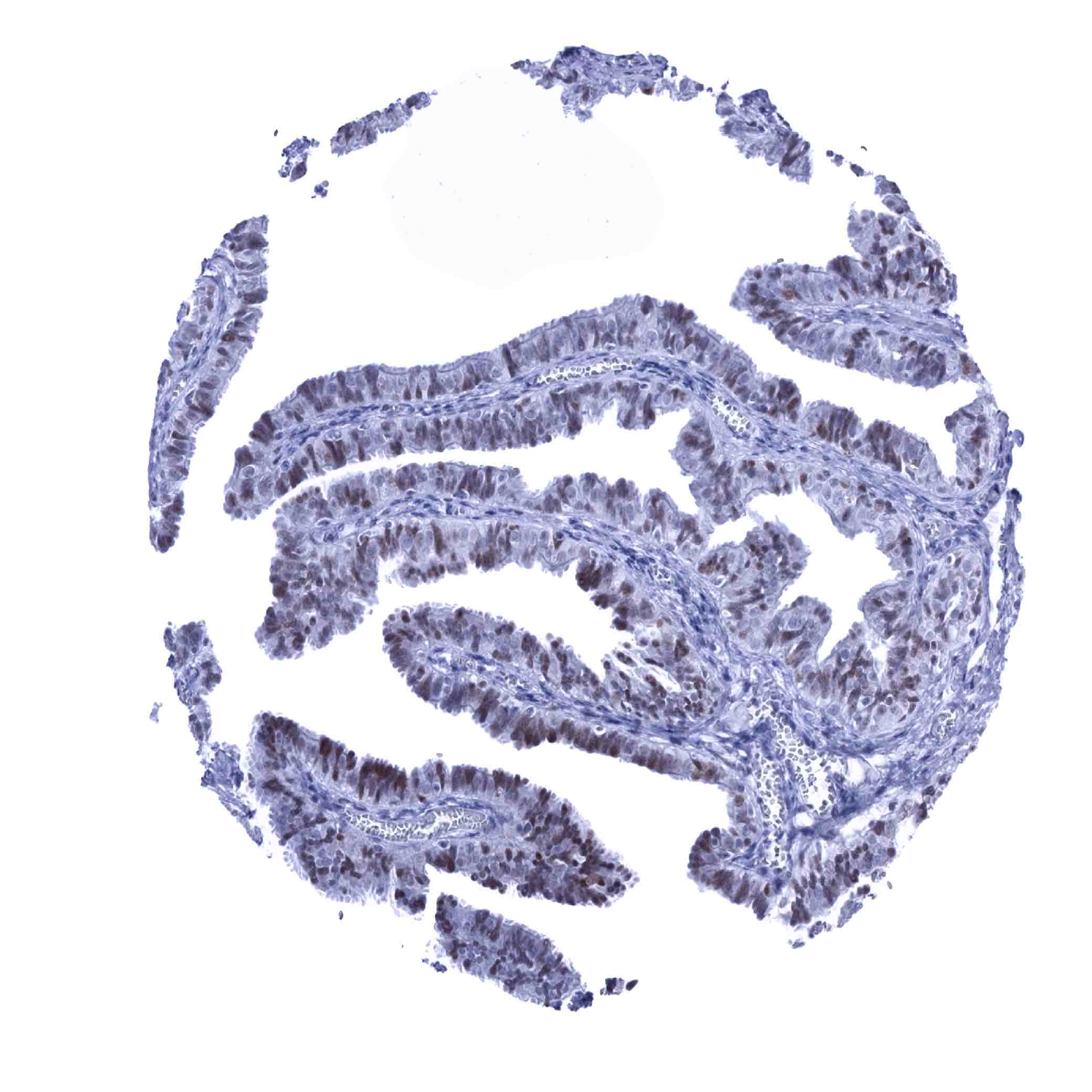
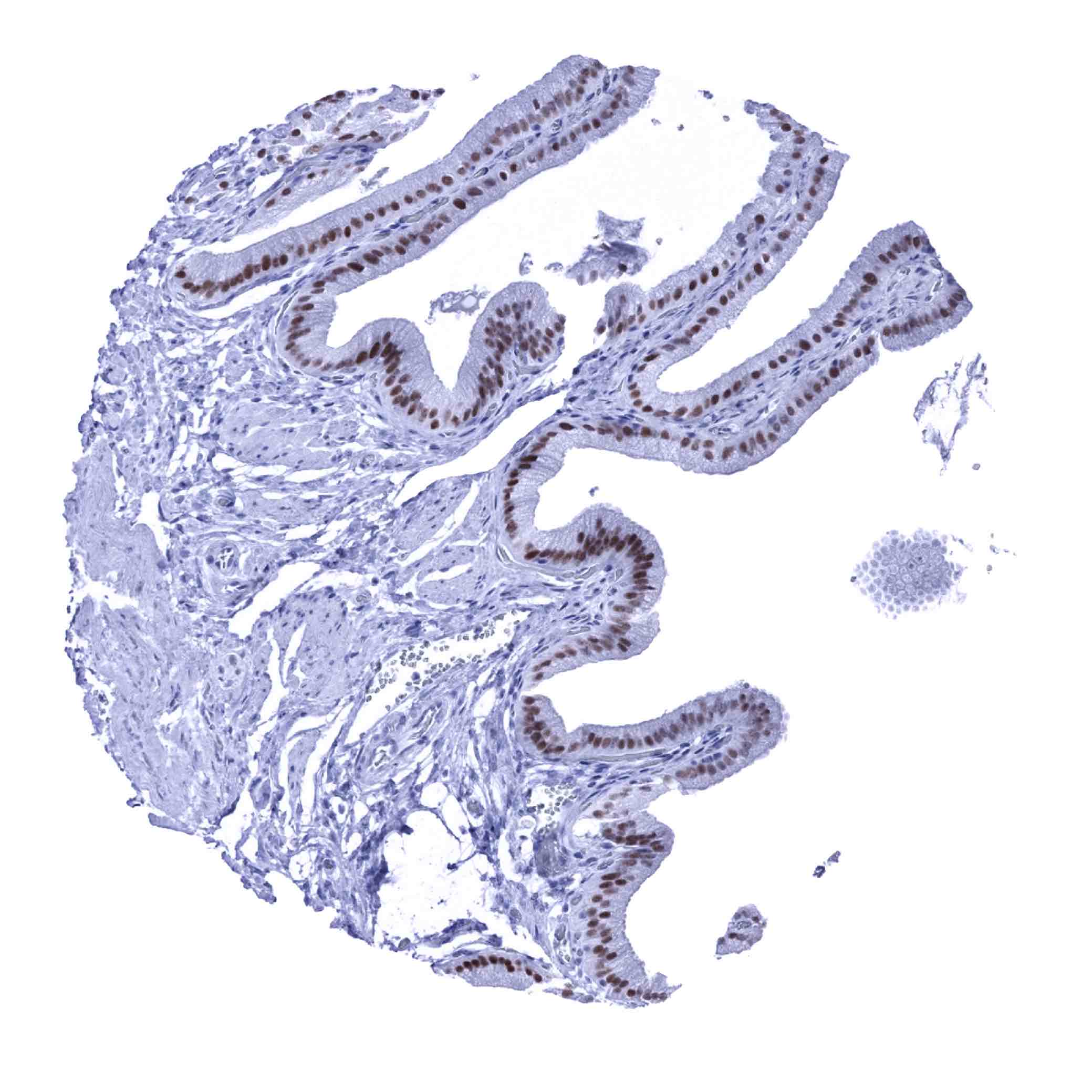
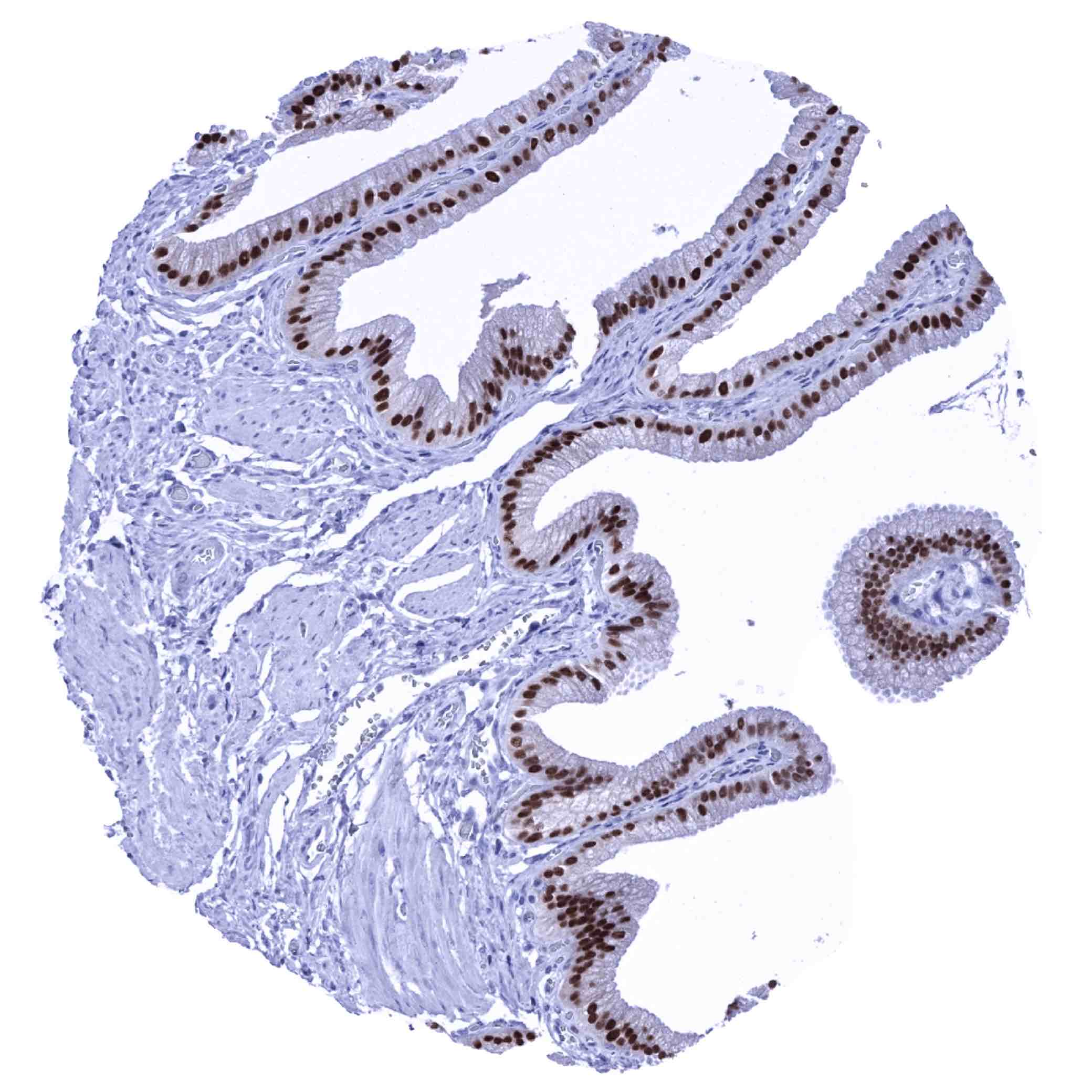
| Fallopian Tube | Moderate to strong SOX9 staining of a large subset of epithelial cells. | |
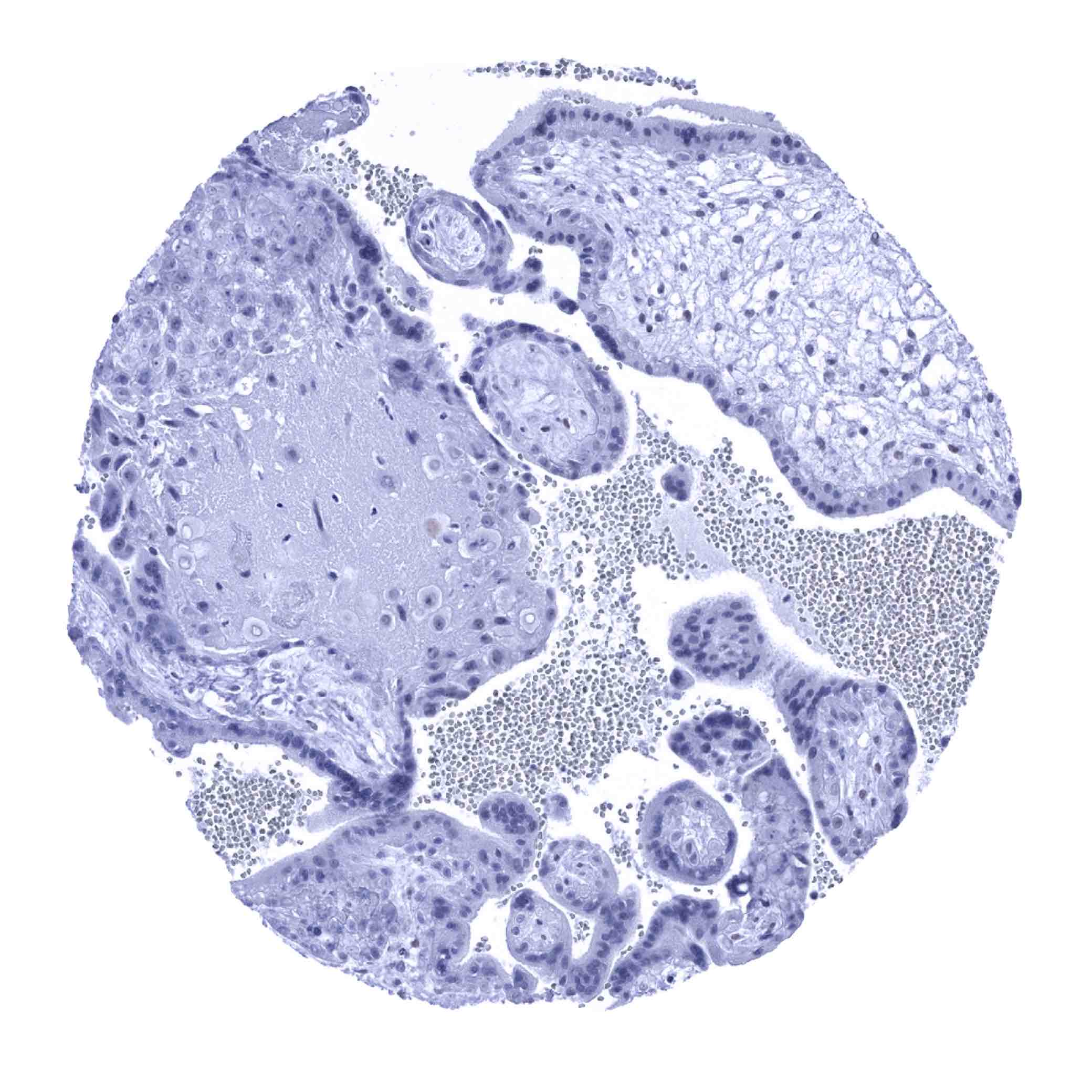
| Ovary | Negative. | |
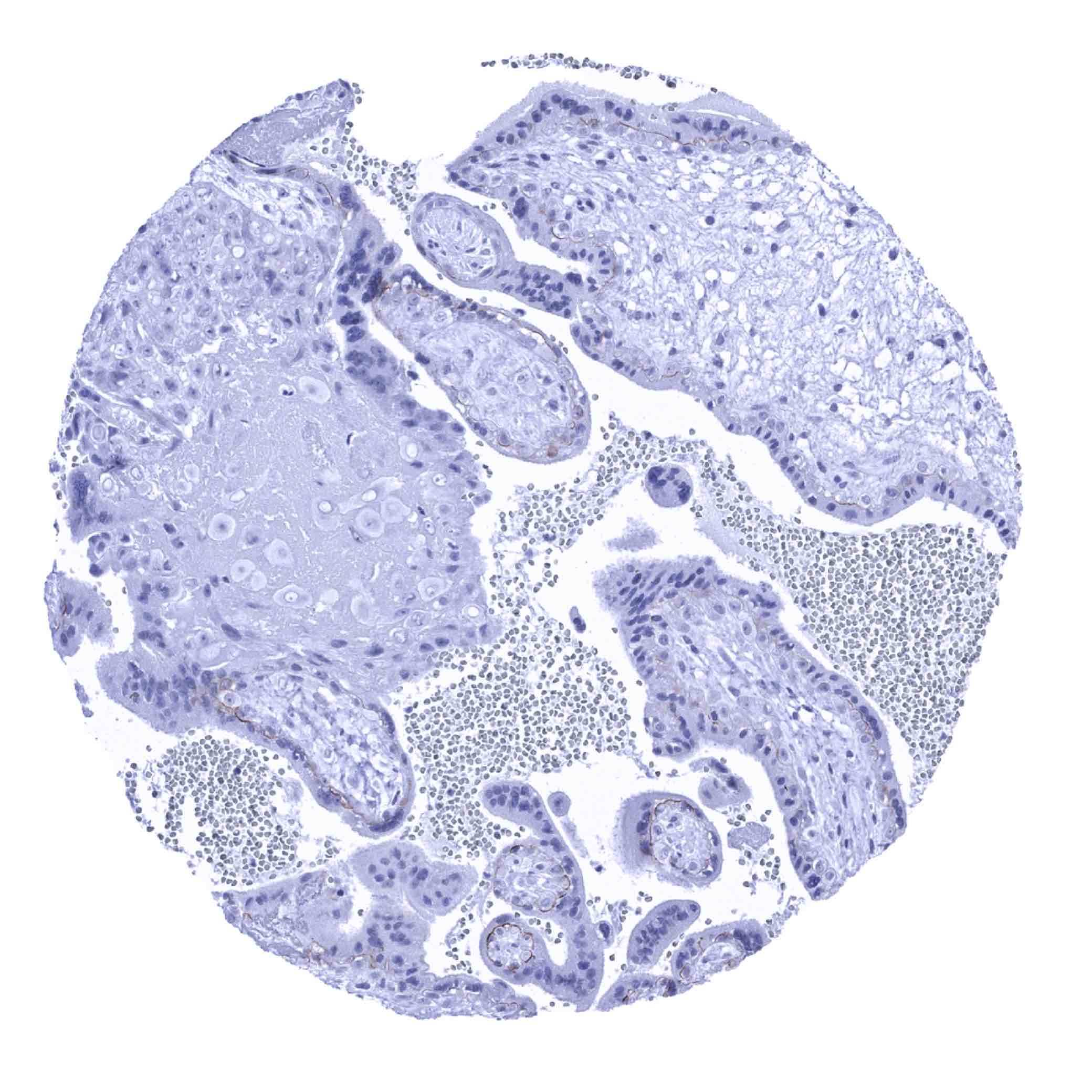
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | Weak nuclear SOX9 staining of amnion cells. | |
| Chorion | Negative. | |
| Skin | Epidermis | Weak to moderate nuclear SOX9 staining of the bottom 2/3 of squamous epithelium. Strong SOX9 staining of ekkrine glands. |
| Sebaceous glands | Weak to moderate nuclear SOX9 staining. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/lymphoid tissue | Bone marrow | Negative. |
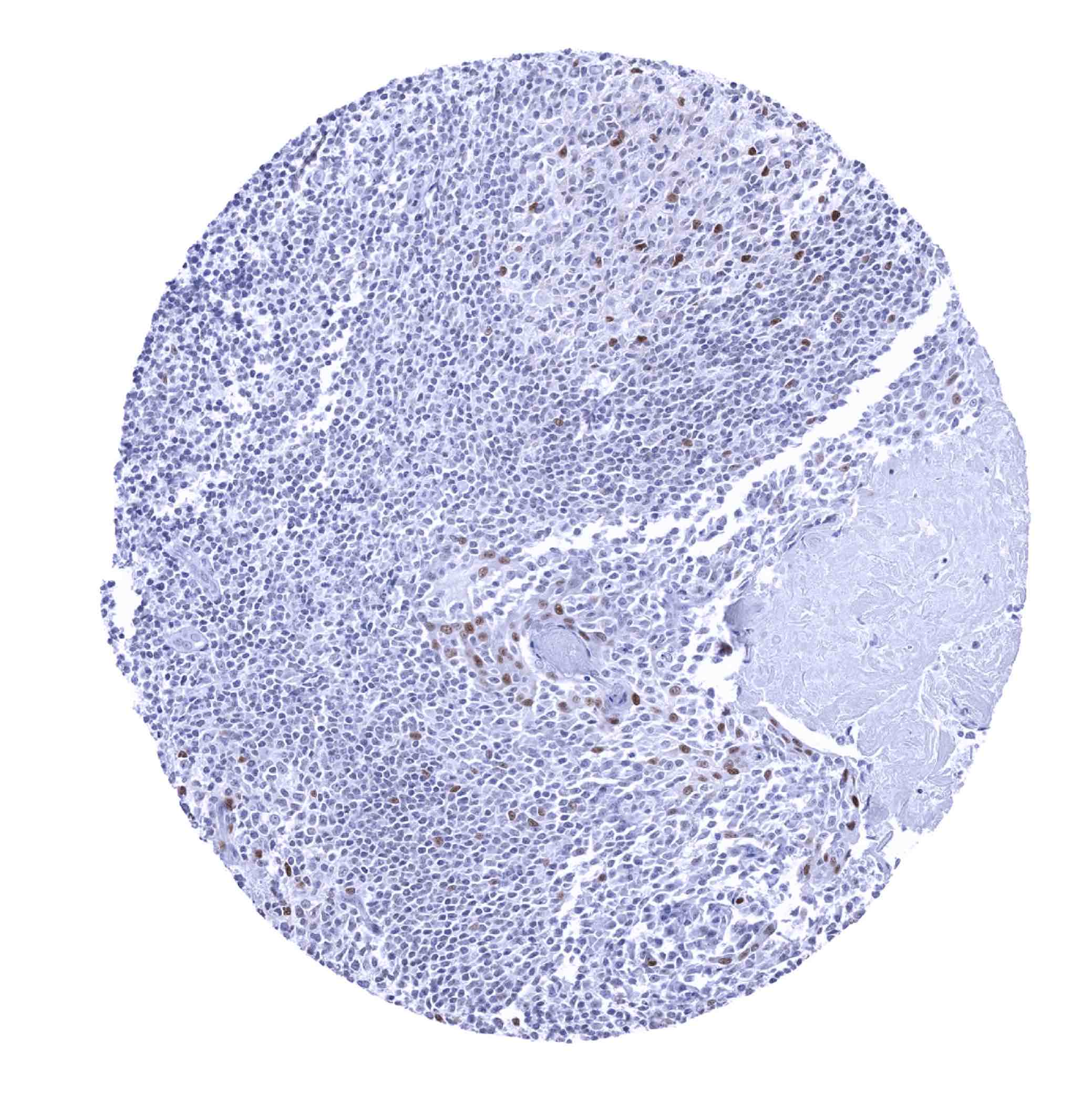
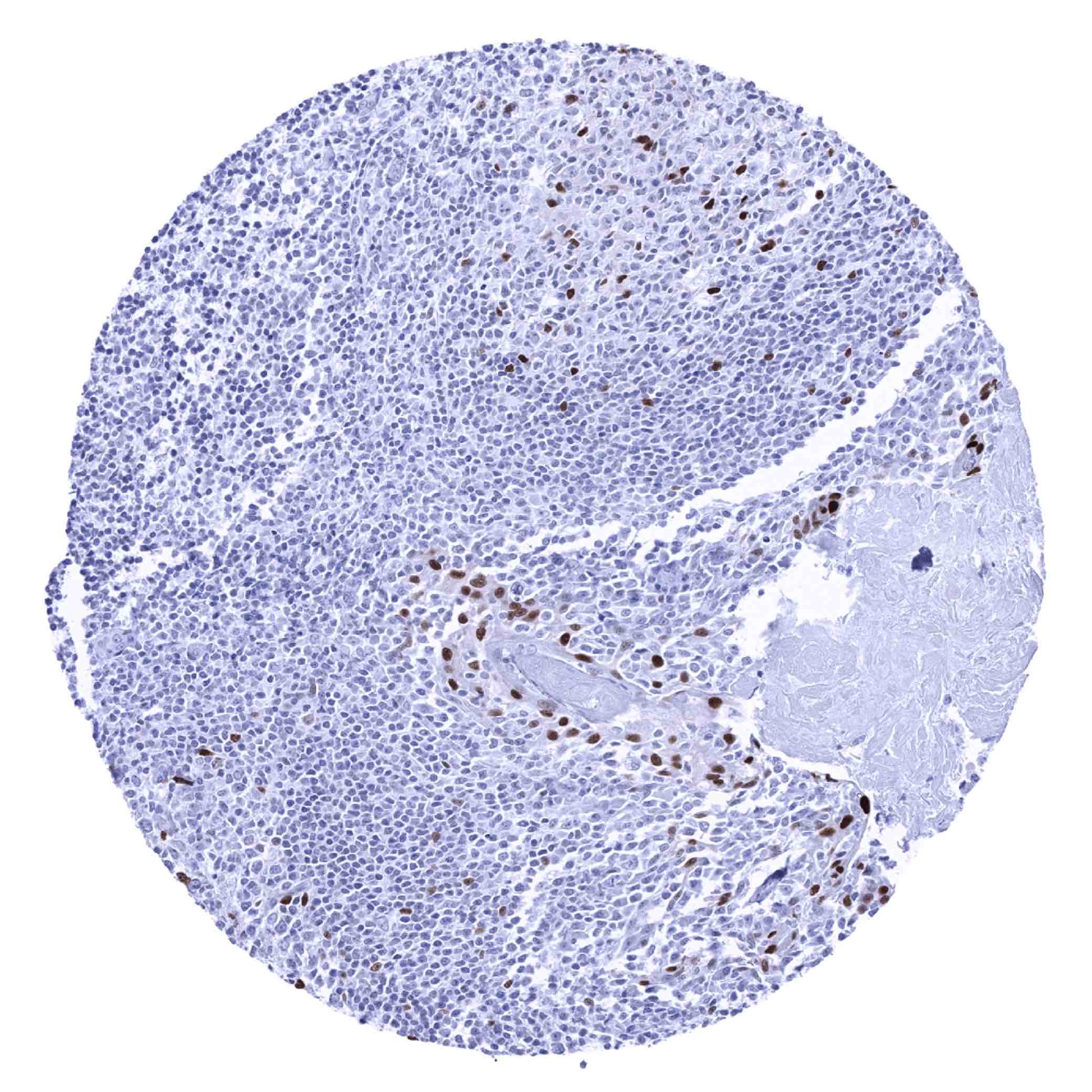
| Lymph node | Weak to moderate nuclear SOX9 positivity of a fraction of cells in germinal centres. | |
| Spleen | Negative. | |
| Thymus | Negative. | |
| Tonsil | Weak to moderate nuclear SOX9 staining of a fraction of epithelial cells. Weak to moderate nuclear SOX9 positivity of a fraction of cells in germinal centres. | |
| Remarks | * SOX9 negativity in the brain contradicts RNA expression data. It is possible that this discrepancy is due to the prolonged formalin fixation of brain tissues rendering protein detection by IHC more difficult. |
These findings are largely consistent with the RNA and protein data described in the Human Protein Atlas (Tissue expression SOX9)
Positive control = Colon: A strong SOX9 immunostaining should be seen in epithelial cells of the crypt base.
Negative control = Colon: SOX9 immunostaining should be absent in all non-epithelial cell types (except few cells in lymphoid germinal centres – if present).
Staining Pattern in Relevant Tumor Types
Tumors with variable levels of SOX9 immunostaining can be seen within a variety of different tumor entities.
The TCGA findings on SOX9 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-709R at a dilution of 1:50 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The role of SOX9 is of considerable interest in many different fields such as for example in cancer, regeneration, and stem cell research.
- The prognostic role of SOX9 expression in cancer is under investigation.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: Data derived from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression SOX9) suggest that SOX9 expression occurs in a very broad variety of tissues. That SOX9 RNA expression was particularly low or undetectable in the few organs without detectable protein expression (muscles of all types, fat, placenta, lung, parathyroid gland, bone marrow, spleen) supports the validity of the antibody MSVA-709R to some extent. The only exception was brain with considerable RNA levels but lacking SOX9 detectable protein expression. It is possible that this discrepancy is due to variablilty of SOX9 expression between particular brain regions or to the prolonged formalin fixation of brain tissues rendering IHC detection more difficult.
Comparison of antibodies: Additional evidence for a specific staining of MSVA-709R comes from the confirmation by another independent commercial antibody. This antibody (“validation antibody”) confirmed every individual cell type stained by MSVA-709R and did also not show any staining in the cerebrum and cerebellum samples analyzed by MSVA-709R (images are shown below). Independence of MSVA-709R and the “validation antibody” is supported by a membranous staining of cytotrophoblast cells by the validation antibody but not by MSVA-709R. This cytotrophoblast staining is considered a (tolerable) antibody specific cross-reactivity of the validation antibody.