
295,00 € – 995,00 €
Product details
Synonyms = AIS; Dihydrotestosterone receptor (DHTR); HUMARA; HYSP1; Kennedy disease (KD); Nuclear receptor subfamily 3 group C member 4 (NR3C4); SMAX1; Spinal and bulbar muscular atrophy (SBMA); Testicular Feminization (TFM)
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = MSVA-367R
Positive control = Kidney: An at least weak to moderate nuclear AR immunostaining should be seen in a subset of kidney tubuli and of glomerular cells.
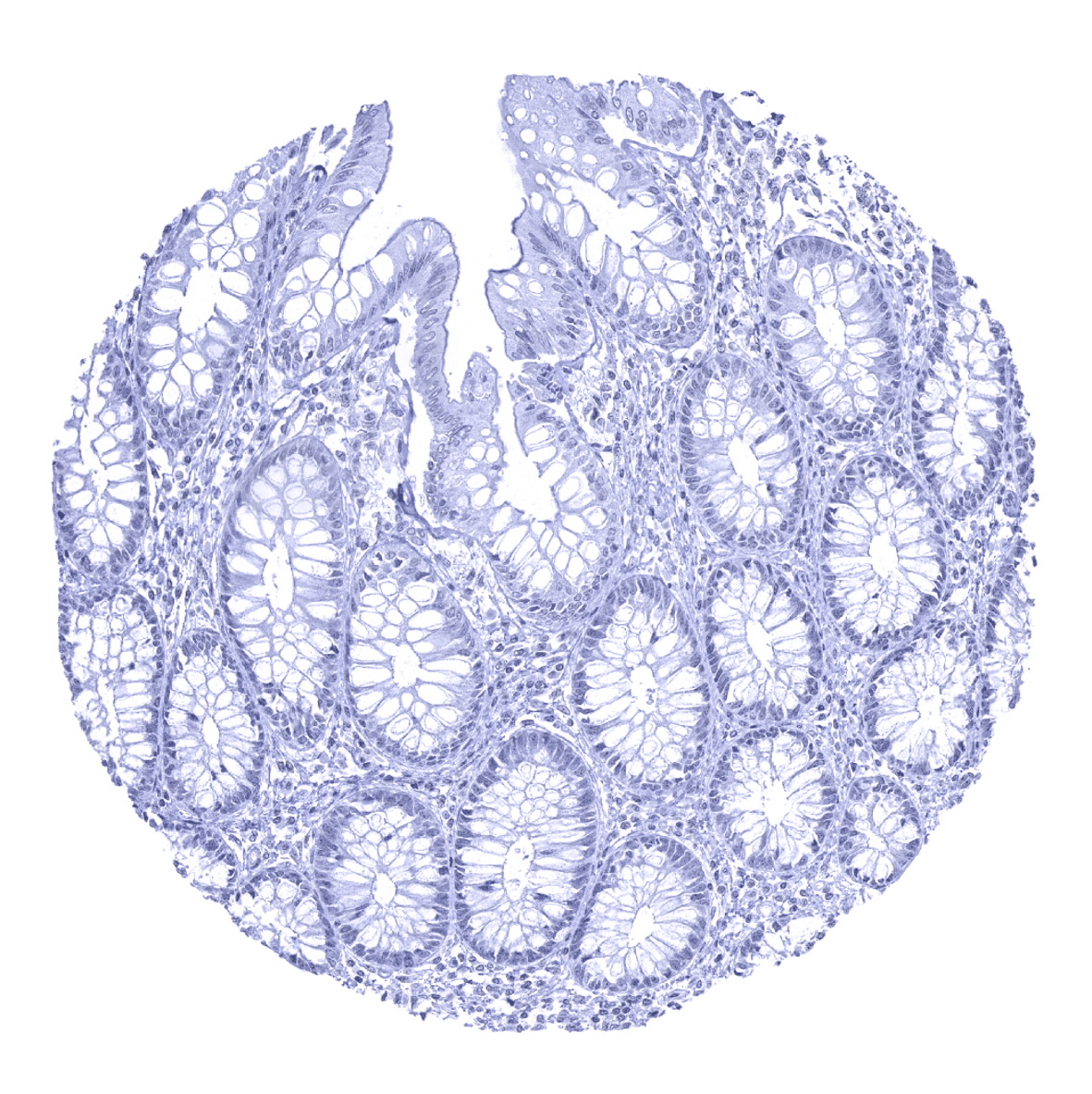
Negative control = Colon: AR immunostaining should be absent in colonic mucosa.
Cellular localization = Nuclear
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
Biology Behind
The androgen receptor (AR) is a 110 kDa DNA-binding transcription factor protein coded by the ASR gene located at Xq12. Inactive AR is located in the cytoplasm where it is bound to heat shock proteins (HSPs). AR activation by testosterone, dihydrotestosterone, or androgen independent mechanisms (JAK1, Aurora A, Src, MAPK2 and ERK1/2 pathways) results in a relieve of heat shock proteins, phosphorylation, conformational transformation, dimerization and translocation of the protein into the nucleus. The dimerized AR binds to a specific 15 base pair sequence of DNA (androgen response element; ARE) which occurs in numerous AR target genes and initiates transcription of these genes. Androgen receptors do also interact with specific signal transduction proteins in the cytoplasm. Androgen binding to cytoplasmic androgen receptors can thus induce changes in cell function independent of changes in gene transcription, such as changes in ion transport. The AR is an important therapeutic target in prostate cancer.
Staining Pattern in Normal Tissues
Androgen receptor immunostaining most prominently occurs in organs of the male genital system. In the prostate, seminal vesicle, and the epididymis, luminal, basal, and stroma cells stains strongly. In the testis, Sertoli, Leydig and stromal cells are AR positive. A moderate to strong staining is also seen in sebaceous glands and in several tissues of the female genital system. Here, a stromal and epithelial cell staining occurs in the myometrium, endometrium (stroma>epithelium), and endocervix of the uterus, the fallopian tube (stromal cells and intercalated cells), and the ovary (follicular cells, theca cells, stromal cells). A moderate AR immunostaining is also seen in hepatocytes, basal cells of the respiratory epithelium, a fraction of tubuli (mostly distal) and podocytes of the kidney, breast glands, and skeletal muscle cells. In squamous epithelium and transitional epithelium of the anal mucosa, a weak to moderate staining of a fraction of cells occurs, predominantly in the lower half of the epithelium. AR is also detectable in the basal cell layers of tonsil crypt epithelium and in a fraction of thymic epithelial cells. A weak AR immunostaining also occurs (at least occasionally) in gallbladder epithelium, excretory and intercalated ducts of the pancreas, glandular cells of salivary glands, gastric glands, decidua cells, placenta trophoblastic cells (predominantly in the first trimenon), thyroid glandular cells, adenohypophysis (few cells with weak staining), urothelium, stroma of the glans penis, smooth muscle of kidney pelvis, and in a fraction of cells in the aortic wall. AR immunostaining is completely absent in the adrenal gland, corpus luteum of the ovary, hematopoietic and lymphoid tissues, many mesenchymal tissues, surface epithelium of the gastrointestinal tract, lung, neurohypophysis, and the brain.
These findings are largely consistent with the RNA and protein data described in the Human Protein Atlas (Tissue expression Androgen Receptor)
Positive control: Kidney: An at least weak to moderate nuclear AR immunostaining should be seen in a subset of kidney tubuli and of glomerular cells.
Negative control: Colon: AR immunostaining should be absent in colonic mucosa.

Staining Pattern in Relevant Tumor Types
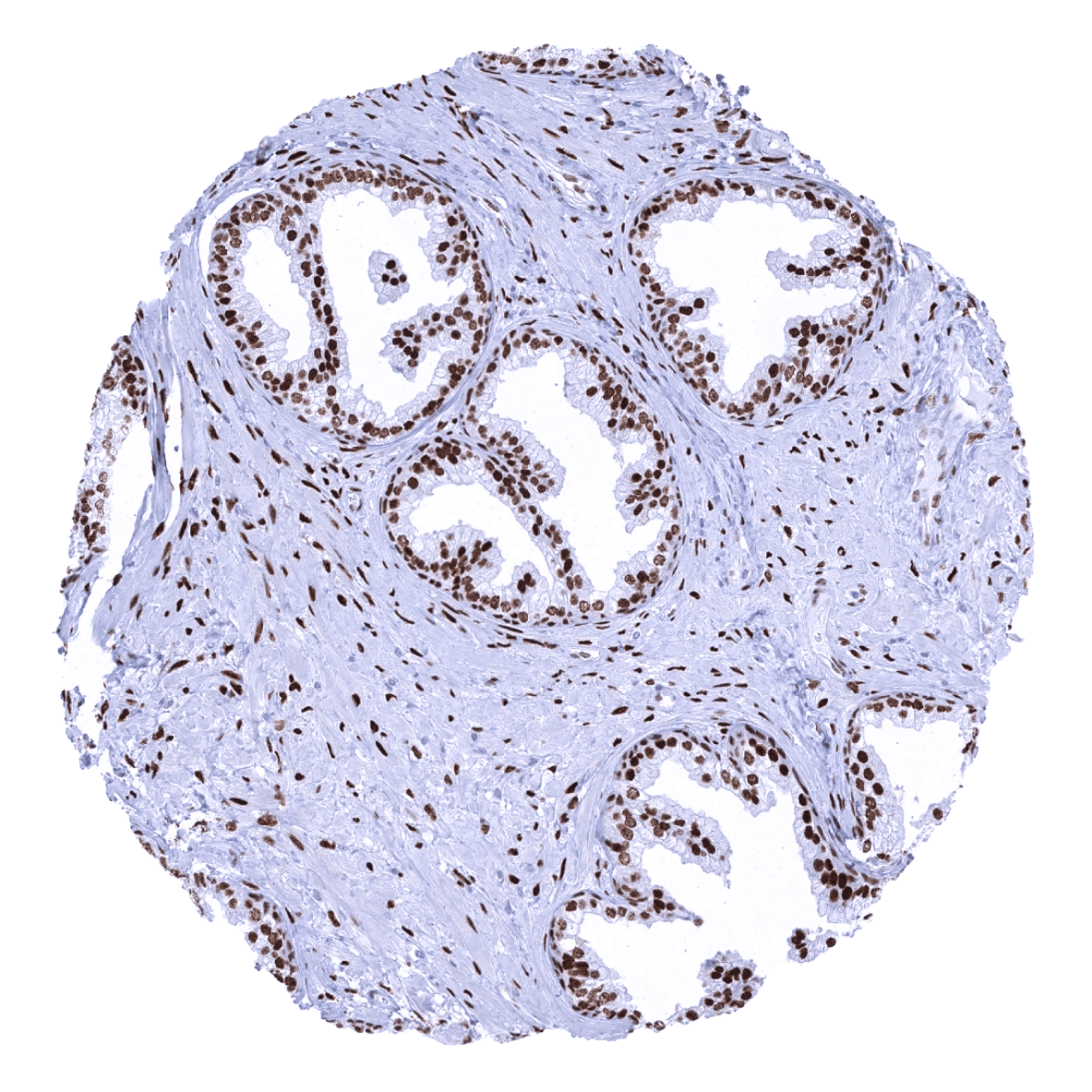
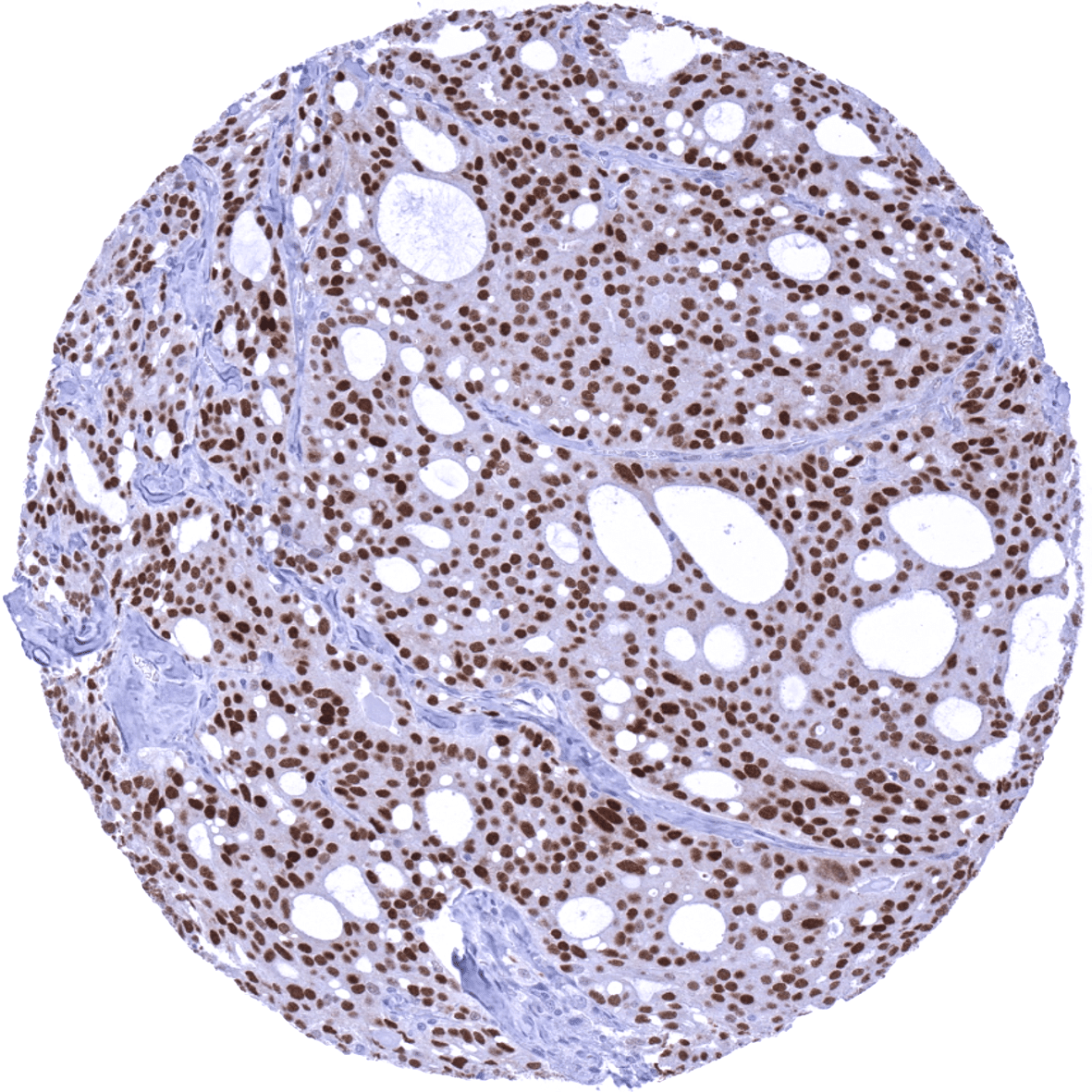
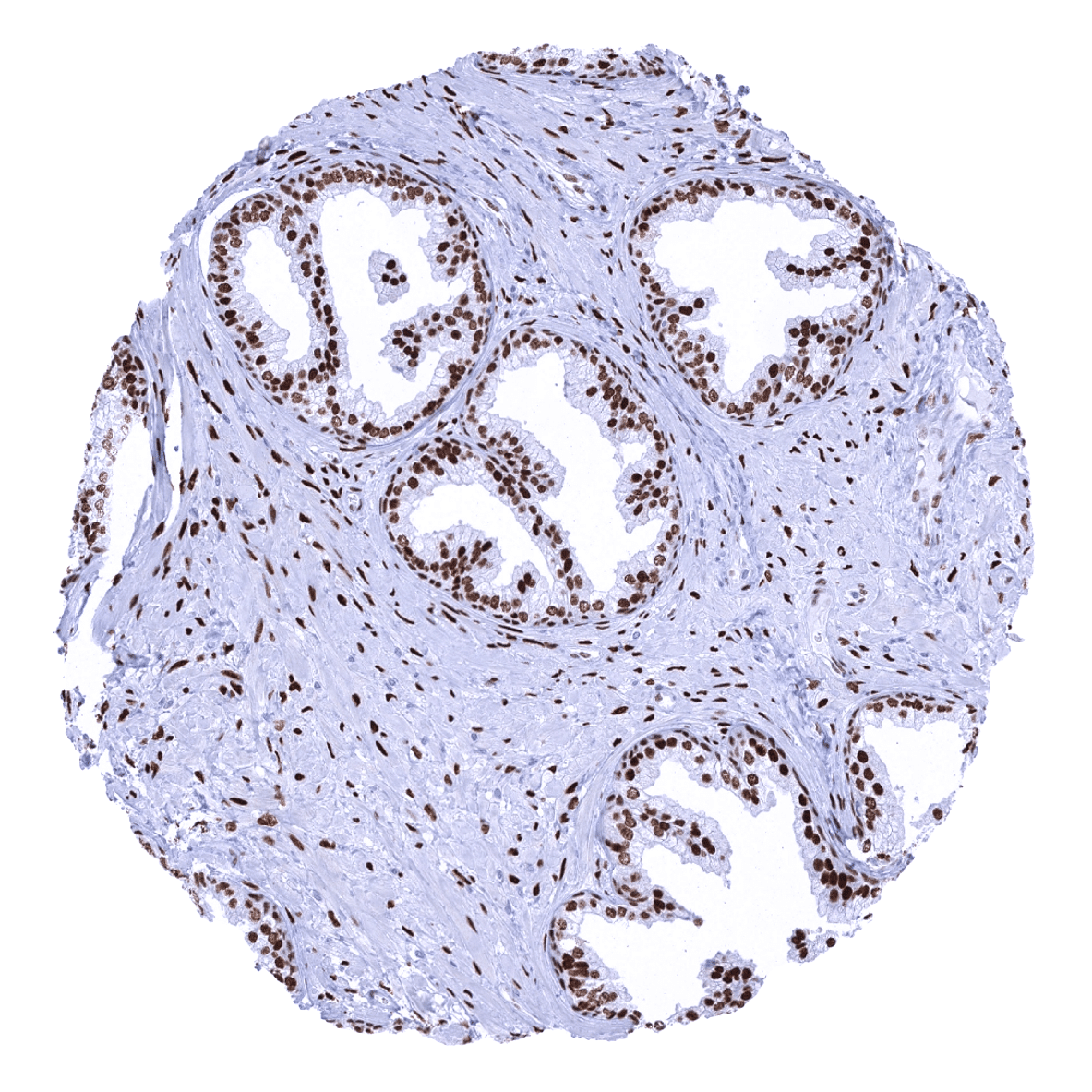
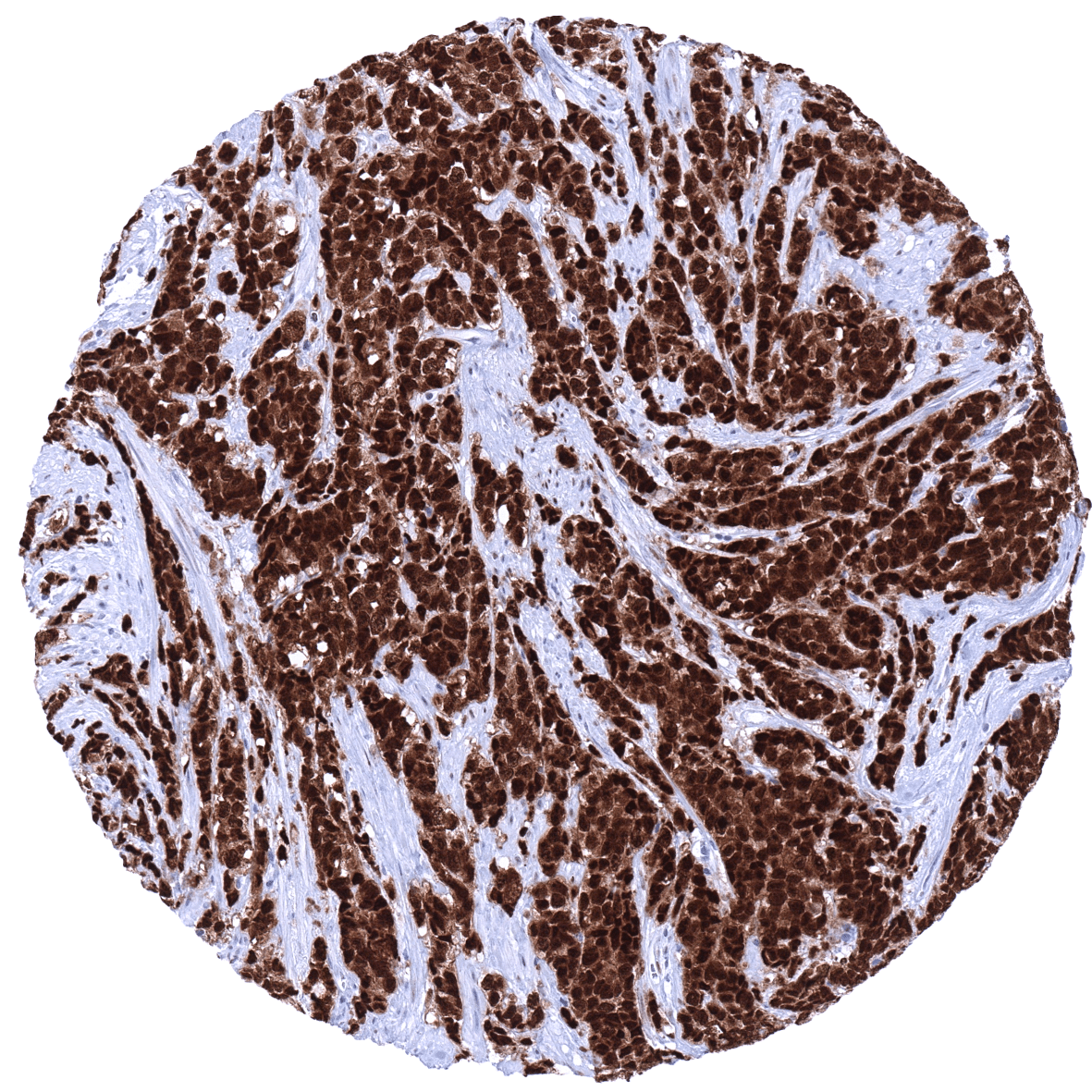
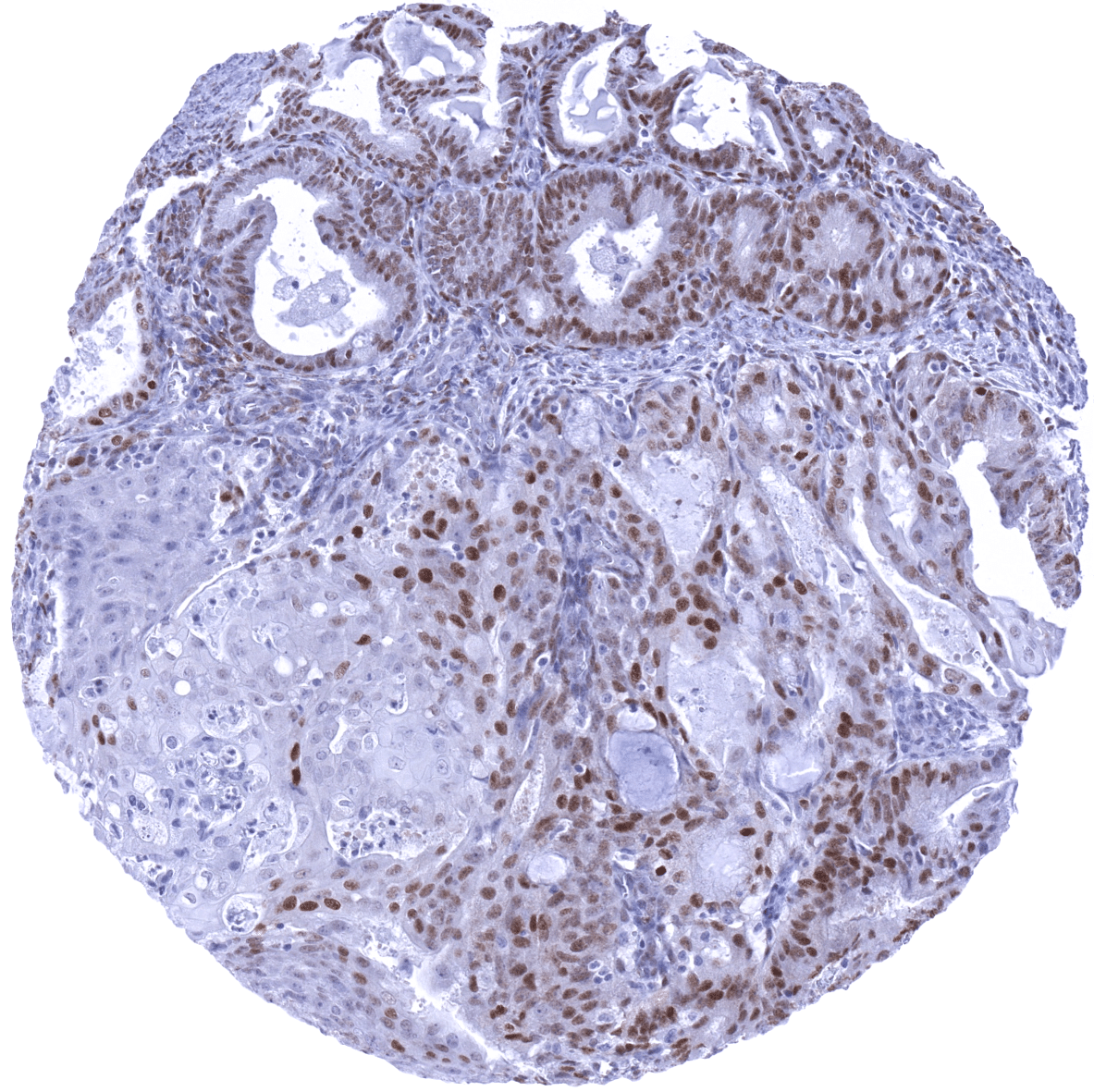
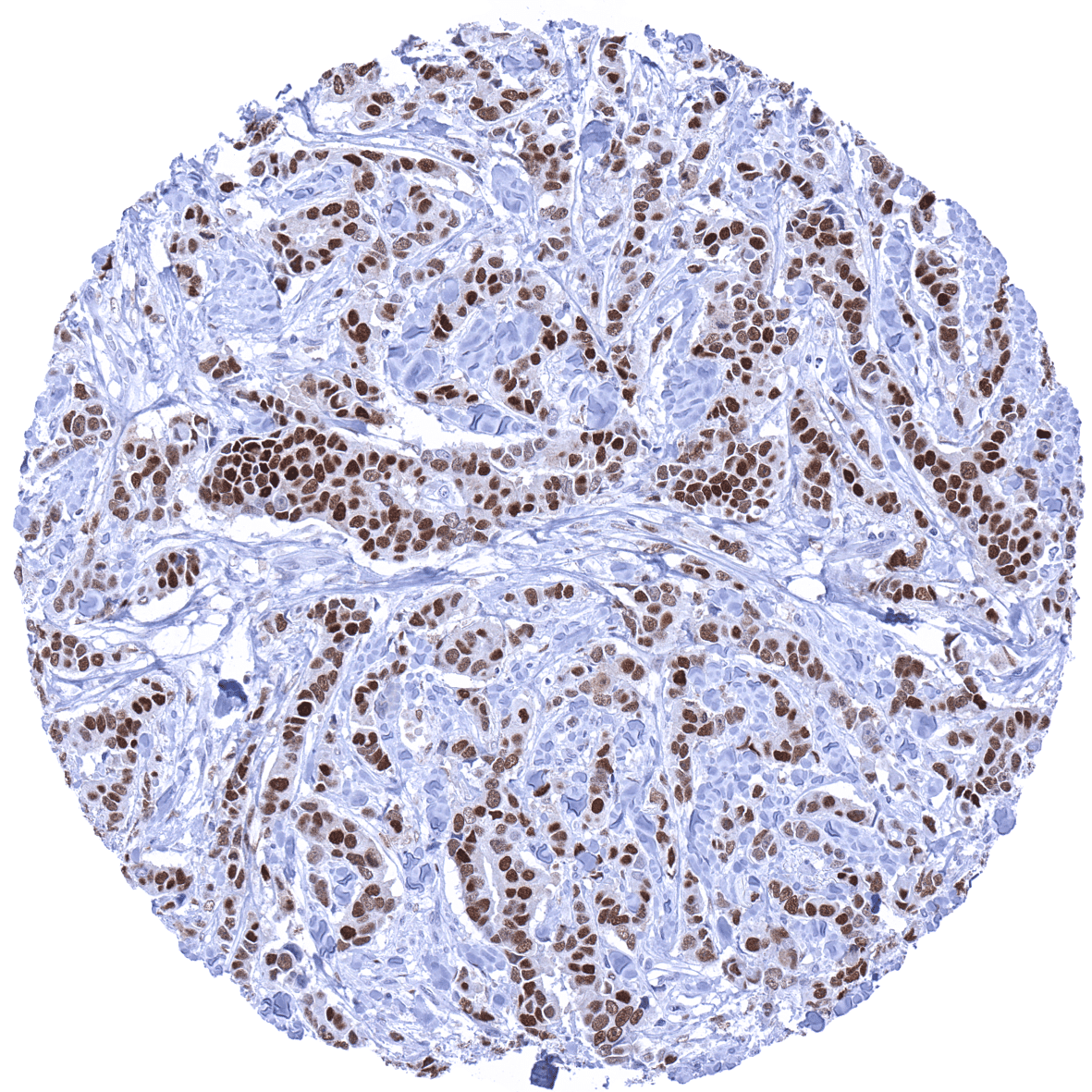
Androgen receptor immunostaining is found in the vast majority of prostate cancers at the time of the initial diagnosis. AR expression can be lost in these tumors as a consequence of long-term treatment with drugs targeting the AR pathway. A loss of AR expression is, however, not a prerequisite for castration resistant prostate cancer. AR immunostaining is at lower frequency and often at lower level also seen in various other tumor types including breast, kidney, endometrium, ovarian, lung, pancreatic, colorectal, bladder, and liver cancer as well as in neuroendocrine tumors.
The TCGA findings on Androgen Receptor RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
Androgen receptor (MSVA-367R) publication summary
Relevant publication: Viehweger et al. “Frequency of Androgen Receptor Positivity in Tumors: A Study Evaluating More Than 18,000 Tumors” Published in Biomedicines. 2024 Apr 25;12(5):957. doi: 10.3390/biomedicines12050957. PMID: 38790919
A total of 14,408 tumors from 141 different tumor categories were successfully analyzed by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. MSVA-367R, at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
Overall, 116 of 141 tumor categories showed detectable androgen receptor (AR) staining with 66 tumor categories showing at least one strongly positive case. A particularly high percentage of tumors with moderate to strong AR immunostaining was detected in sex cord-stromal tumors of the testis (93.3–100%), adenocarcinoma of the prostate (79.3–98.7%), breast neoplasms (25.0–75.5%), other gynecological tumors (0.9–100%), renal cell carcinomas (5.0–44.1%), and in urothelial carcinomas (5.4–24.2%). The distribution of positive staining results is shown in an “organ-systematic” (Figure 1) and in a “ranking order” figure (Figure 2) below (images based on data from Viehweger et al). Data on associations with histopathological and clinical parameters are also summarized below (Table 3; based on data described by Viehweger et al).
Authors conclusions on diagnostic utility of AR IHC with respect to the distinction of different tumor entities (Viehweger et al.):
- All previously suggested diagnostic applications of AR IHC (such as the distinction of prostate cancer or breast cancer with apocrine differentiation) are not strongly supported by the data of this study given the abundance of AR expression – even at high levels –in many different cancer types.
Authors conclusions on the prognostic role of AR immunostaining results (Viehweger et al.):
- Low AR was linked to advanced tumor stage (pTa versus pT2-4; p<0.0001) in urothelial carcinoma.
- Low AR was linked to high tumor stage (p<0.0001), high tumor grade (p<0.0001), lymph node metastasis (p<0.0001), and shorter overall survival (p=0.0094) In invasive breast carcinoma.
- Low AR was linked to high pT stage (p<0.0001) and high tumor grade (p<0.0001) in clear cell renal cell carcinoma (RCC),
- Low AR was linked to high pT stage (p=0.0055) as well as high ISUP (p=0.0179) and Fuhrman grade (p=0.0018) in papillary RCC.
Figure 1. Androgen Receptor staining in cancer (“organ-systematic”; according to Viehweger et al.)

Figure 2. Androgen Receptor staining in cancer (“ranking list”; according to Viehweger et al.)

Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
-Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-367R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The diagnostic utility of AR immunohistochemistry needs to be evaluated
- The prognostic and predictive role of androgen receptor expression in breast cancer and other cancers should be evaluated.
- The complex relationship between AR and interaction partners such as JAK1, Aurora A, Src, MAPK2 and ERK1/2 requires further investigation.
Evidence for Antibody Specificity in IHC
There are only two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody MSVA-367R specificity is suggested by the strong concordance of its immunostaining properties with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression Androgen receptor). Immunostaining by using MSVA-367R is regularly detected in organs with documented RNA expression such as in male and female genital organs, liver, gallbladder, kidney, skeletal muscle, skin, and the thymus. For some other tissues (pancreas, salivary glands, respiratory epithelium, bronchial glands, gastric glands) the AR protein expression detected by MSVA-367R is not matched by a significant RNA expression found for these organs. This is probably because the AR positive cell types are making up only for a small fraction of the respective organs, resulting in a massive underrepresentation of the RNAs of AR expressing cells. True expression of AR in these organs is, however, supported by a comparison with a second independent antibody.
Comparison of antibodies:
True expression of AR in:
- pancreas
- salivary glands
- respiratory epithelium
- bronchial glands
- * gastric glands is suggested by a comparable – although very weak – staining obtained by the use of the antibody CAB065764 in the human protein atlas analysis.
