
195,00 € – 695,00 €
Product details
Synonyms = Gastric mucin 6; MUC6; MUC6 mucin; Mucin 6 oligomeric mucus/gel forming; Mucin glycoprotein Fragment; Mucin-6; Secretory mucin MUC6
Antibody type = Recombinant Rabbit monoclonal / IgG1
Clone = MSVA-806R
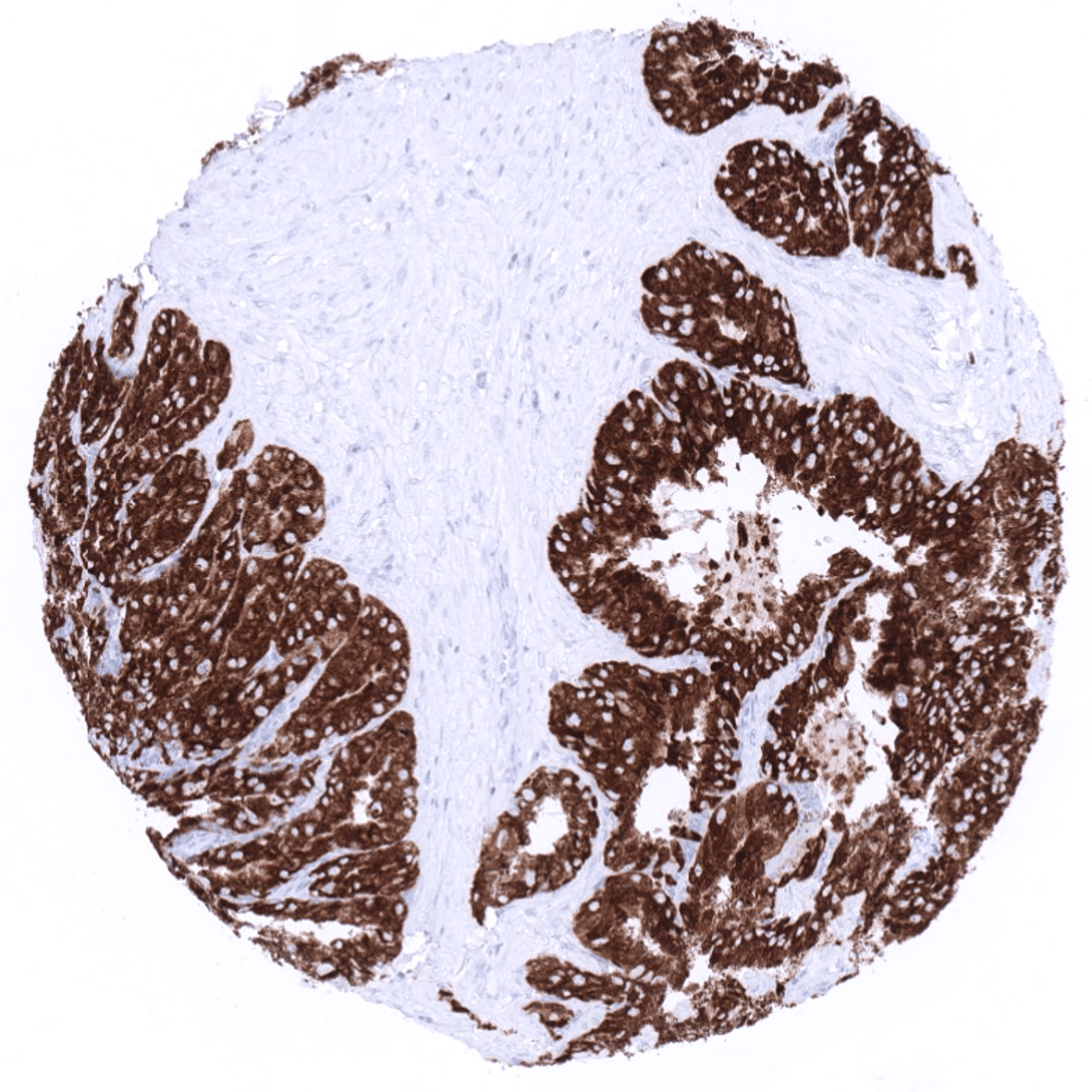
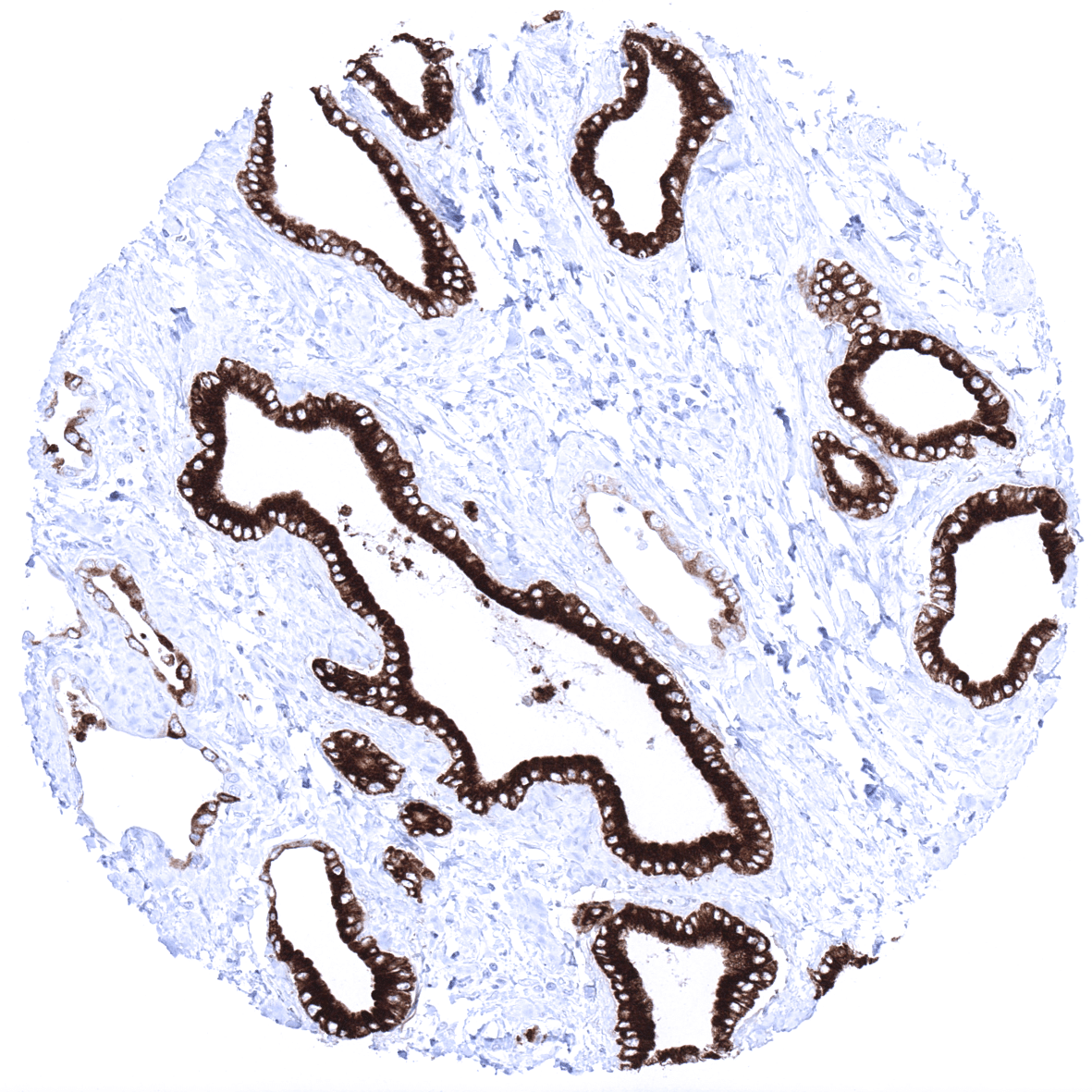
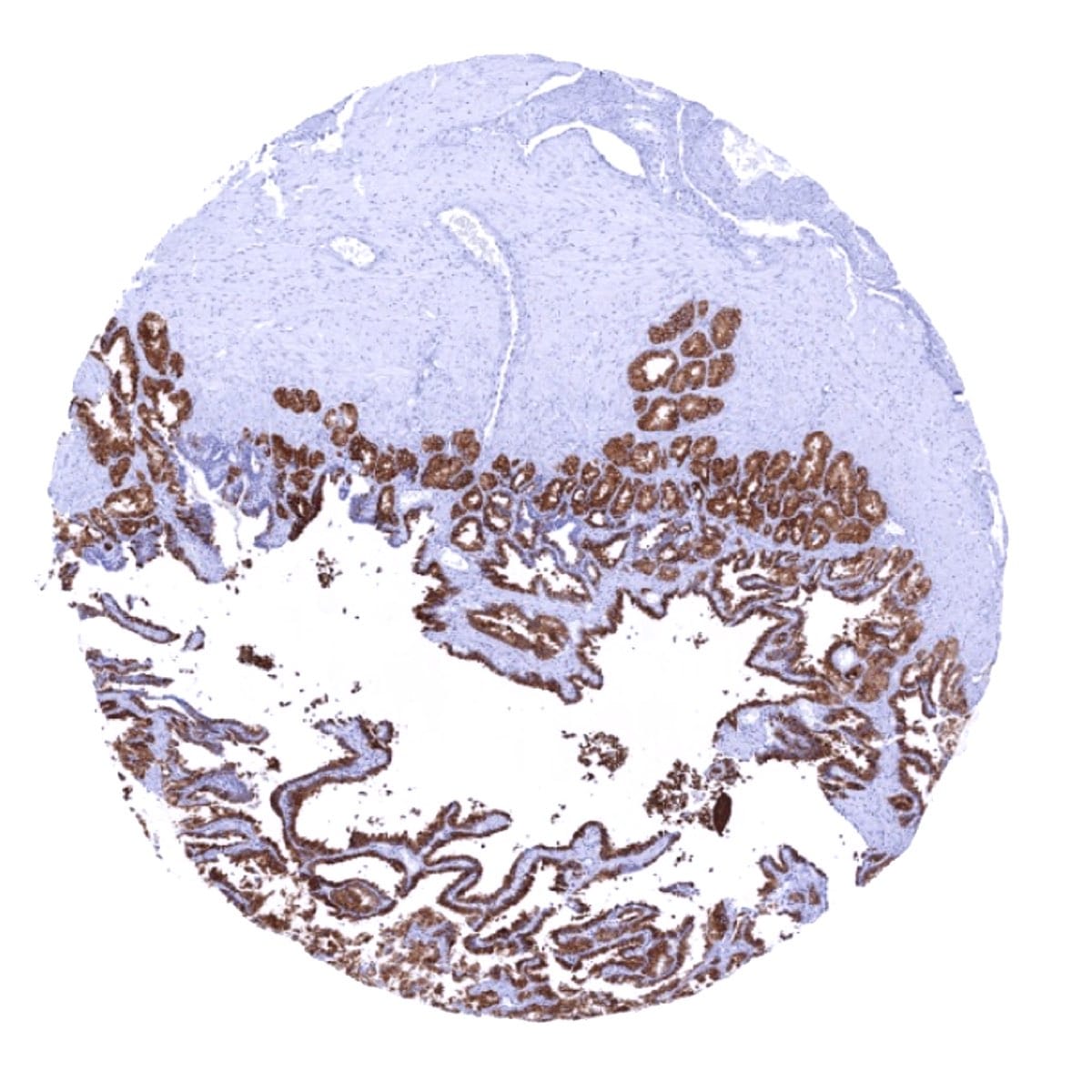
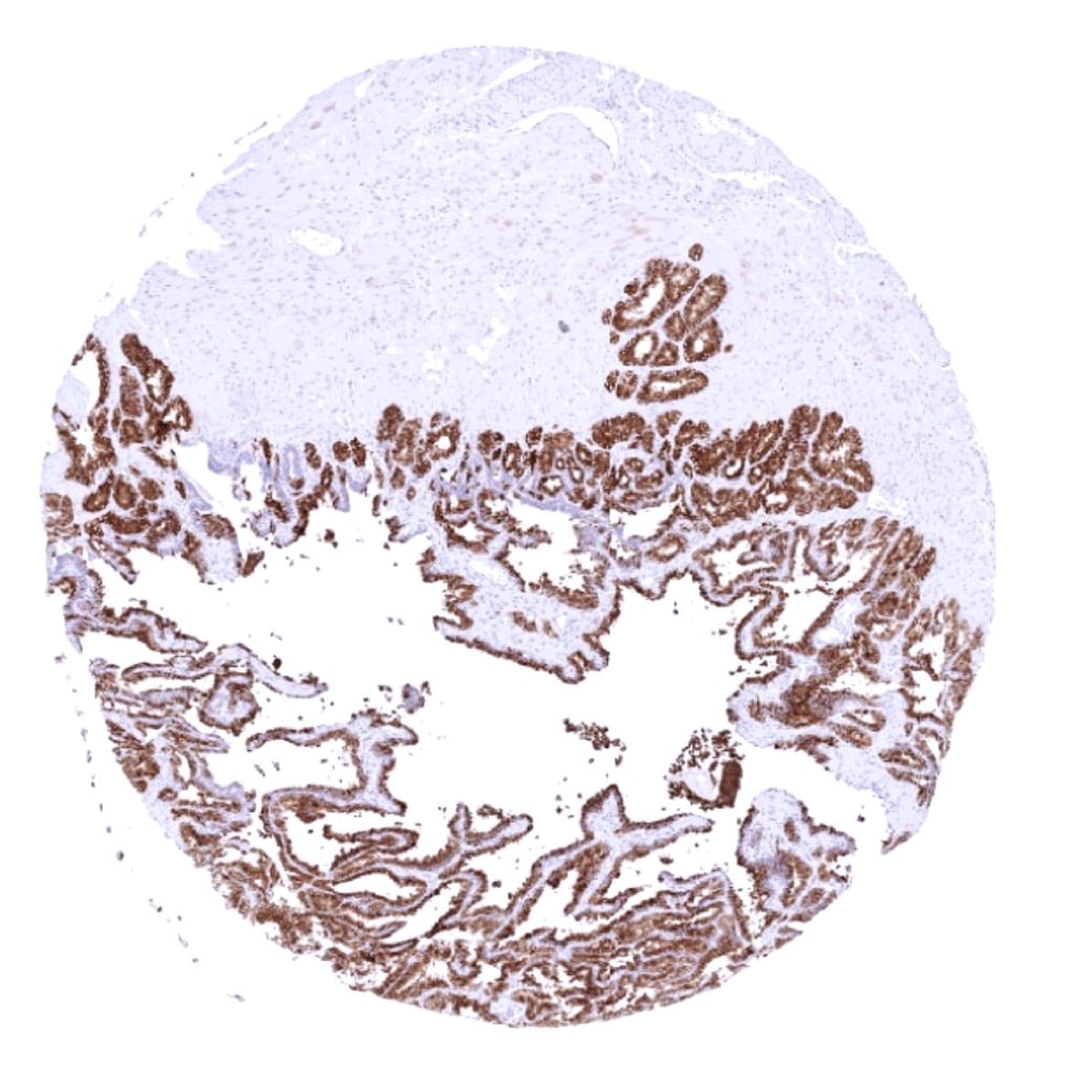
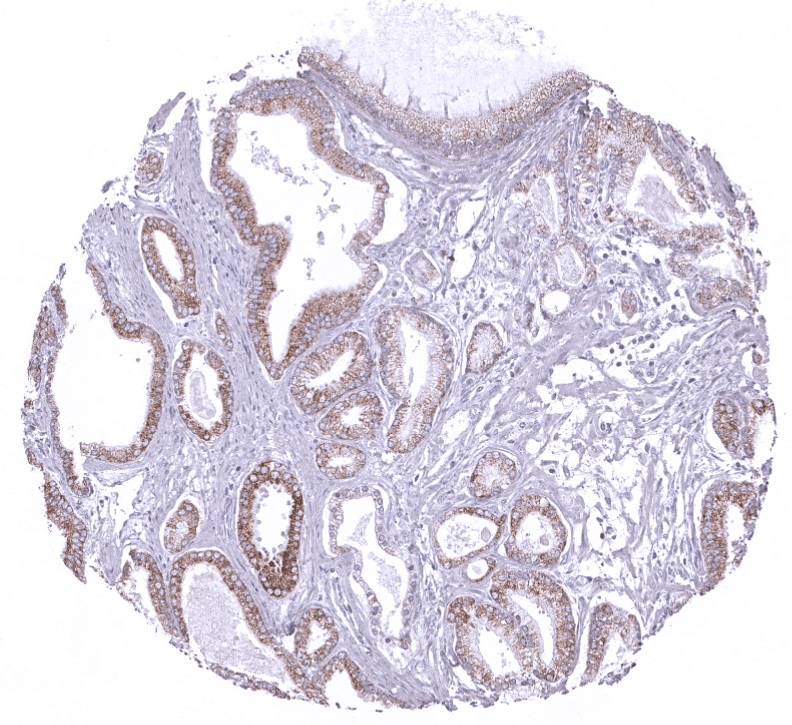
Positive control = Stomach: Mucous secreting glands should be strongly positive.
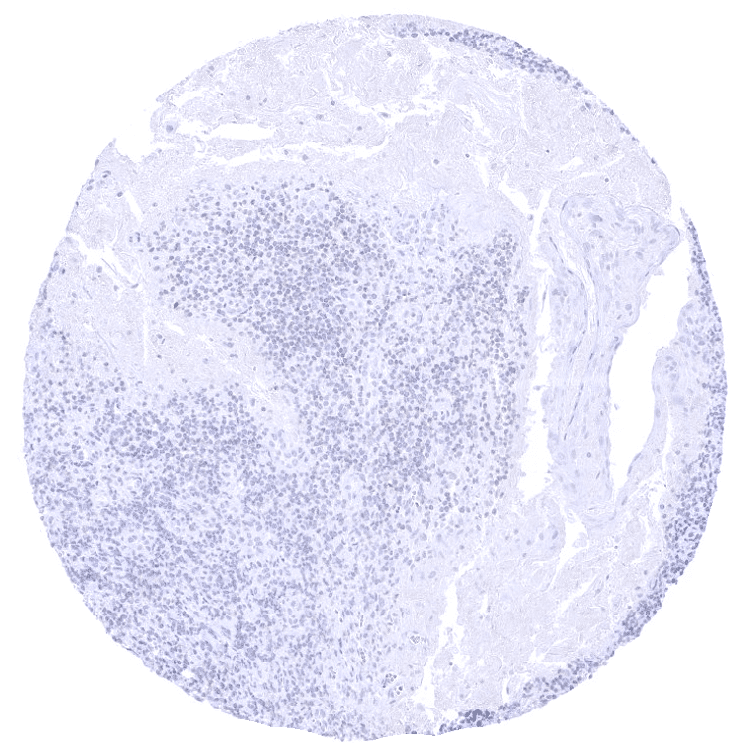
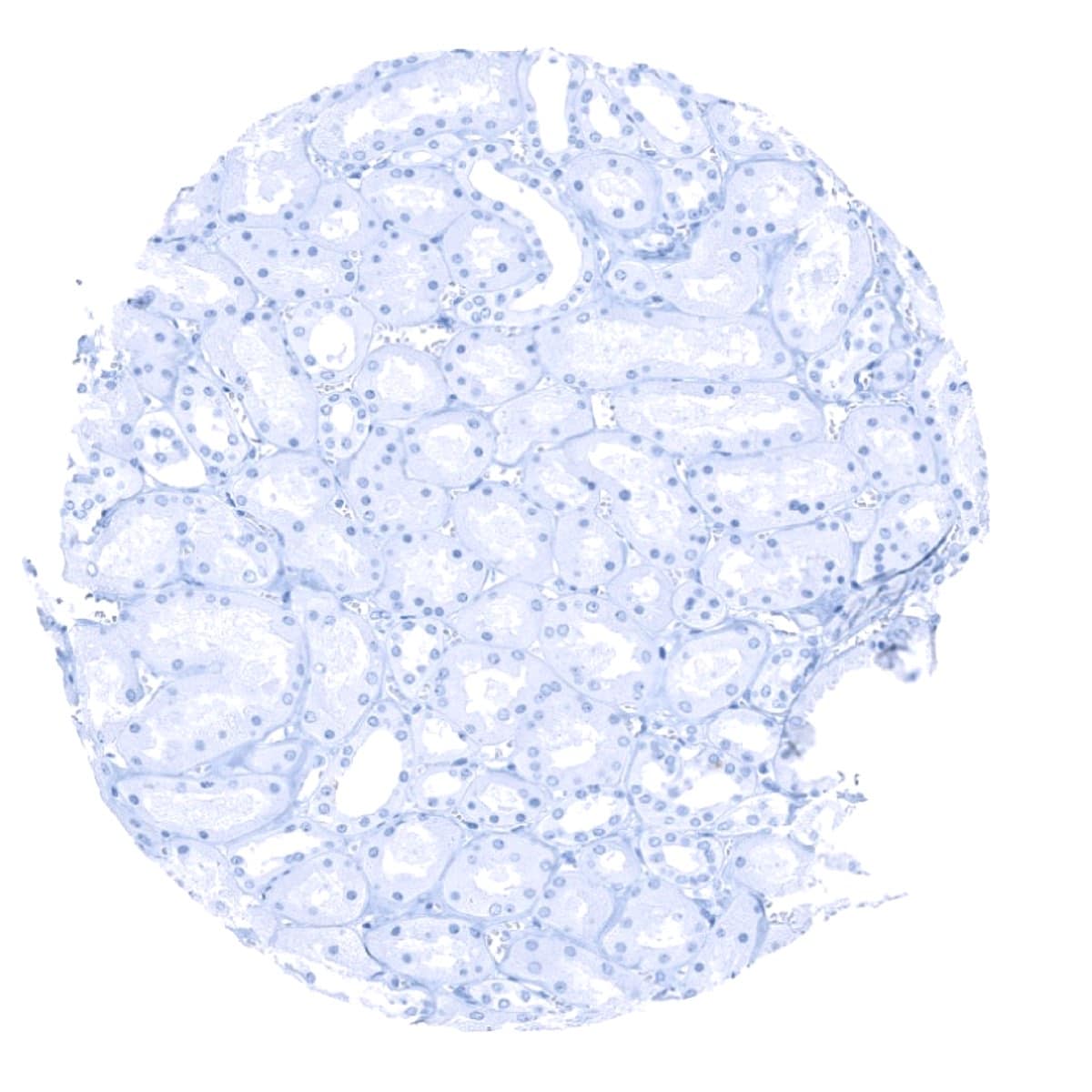
Negative control = Stomach: Surface epithelium should be completely negative.
Cellular localization = Cytoplasmic
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
Mucin 6 (MUC6) is a secretory gastric mucin which is expressed in various tumor types.
Biology Behind
Mucin 6 (MUC6) is a secretory gastric mucin that was first identified from a gastric mucosal cDNA library. As a secretory mucin, its main role is the formation of a protective barrier for the stomach epithelium and the lubrification of nutrition which is accomplished in collaboration with other mucins. MUC6 is also expressed in various cancers, where it may also play a role for tumor biology. There is evidence that MUC6 inhibits tumor cell motility and that it becomes epigenetically deregulated in carcinoma cells.
Staining Pattern in Normal Tissues
The strongest MUC6 expression (+++) is detected in epithelial cells of seminal vesicles, Brunner glands of the duodenum, and the mucous secreting glands – but not the surface epithelium – of the stomach. MUC6 immunostaining is also consistently present in Intercalated and interlobular ducts of the pancreas, small juxtaportal bile ducts (portal bile ducts are largely negative), gallbladder surface epithelium (not all cells in all samples), epididymis (more intense staining in the cauda than in the caput, where positivity can be focal), fallopian tube (variable number of scattered positive cells), and endocervical glands (weak). In some samples, few scattered MUC6 positive cells can be found in collecting ducts of the kidney, breast glands, pregnancy endometrium, and in the trophoblast of the first trimenon placenta. Skin and non-keratinizing squamous epithelium of oral cavity, lip, tonsil surface and crypts, ectocervix, and esophagus as well as Hassal’s corpuscles in the thymus are MUC6 negative. MUC6 staining is also absent in all mesenchymal tissues including myometrium, lymphatic and hematopoietic cells, hepatocytes, proximal and distal tubuli as well as glomeruli of the kidney, salivary glands, prostate, testis, respiratory epithelium, lung, ovary including corpus luteum and follicular cysts, mature placenta, adrenal gland, thyroid, cerebrum, cerebellum, adeno- and neurohypophysis.
MSVA-806R validation data showed strong MUC6 immunostaining in all tissues that were delineated as MUC6 positive in the Human Protein Atlas (Tissue expression MUC6). In extension to these data, we show strong MUC6 expression in Brunner glands of the duodenum, which are not depicted in the tissue atlas image gallery and which may explain occasional MUC6 RNA expression found in the duodenum. Other findings like the staining of small juxtaportal bile ducts are visible on some images provided within the human protein atlas but not explicitly described.
Suggested positive tissue control: Stomach: Mucous secreting glands should be strongly MUC6 positive.
Suggested negative tissue control: Stomach: Surface epithelium should be completely MUC6 negative.
Staining Pattern in Relevant Tumor Types
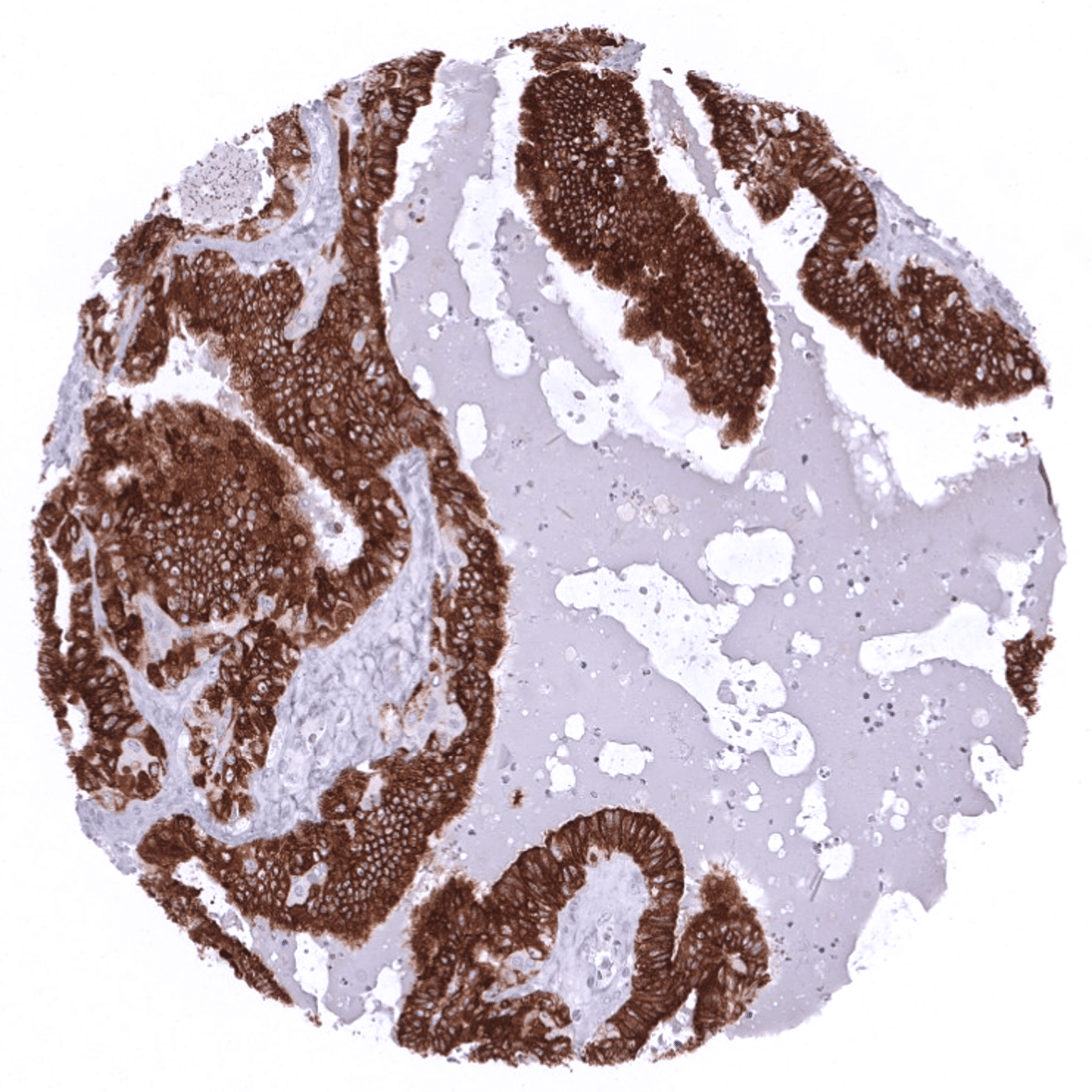
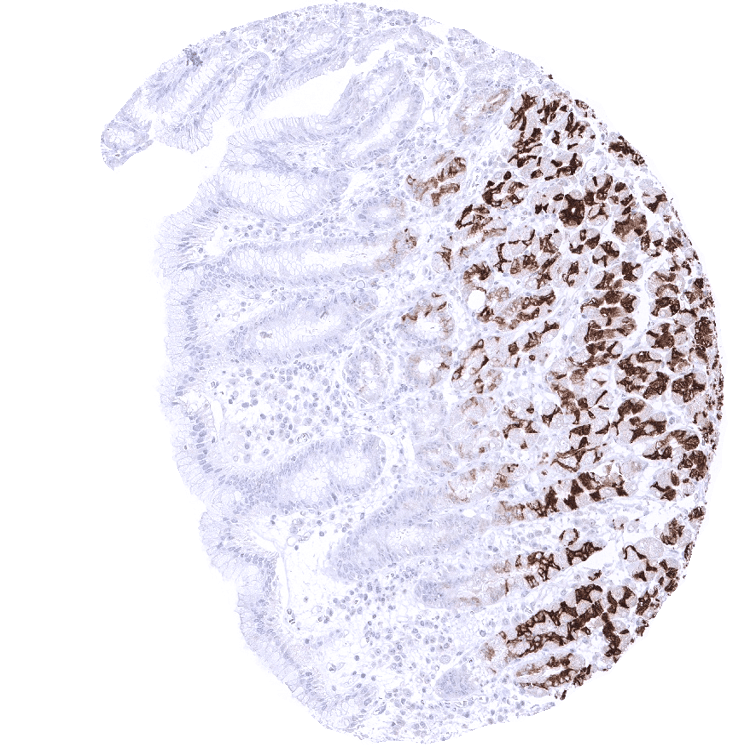
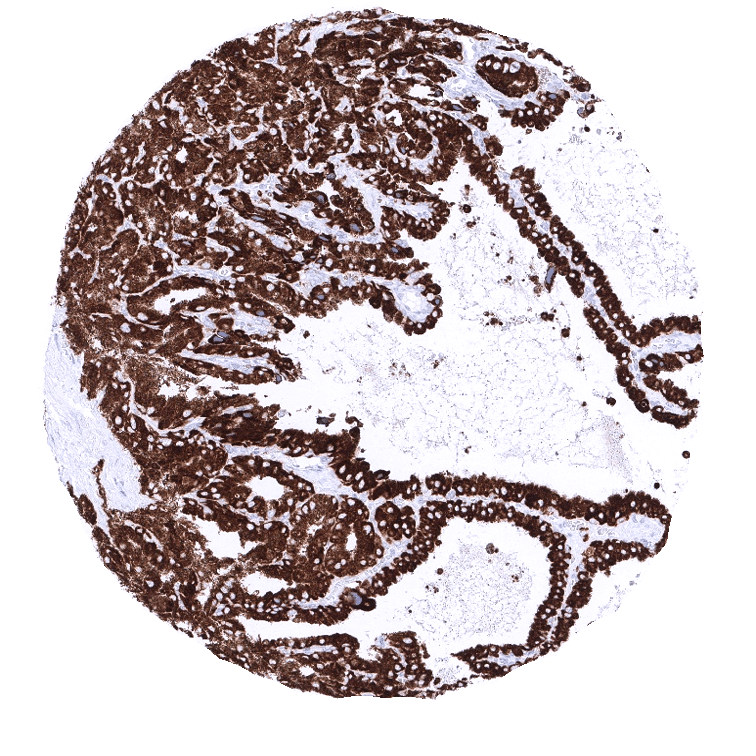
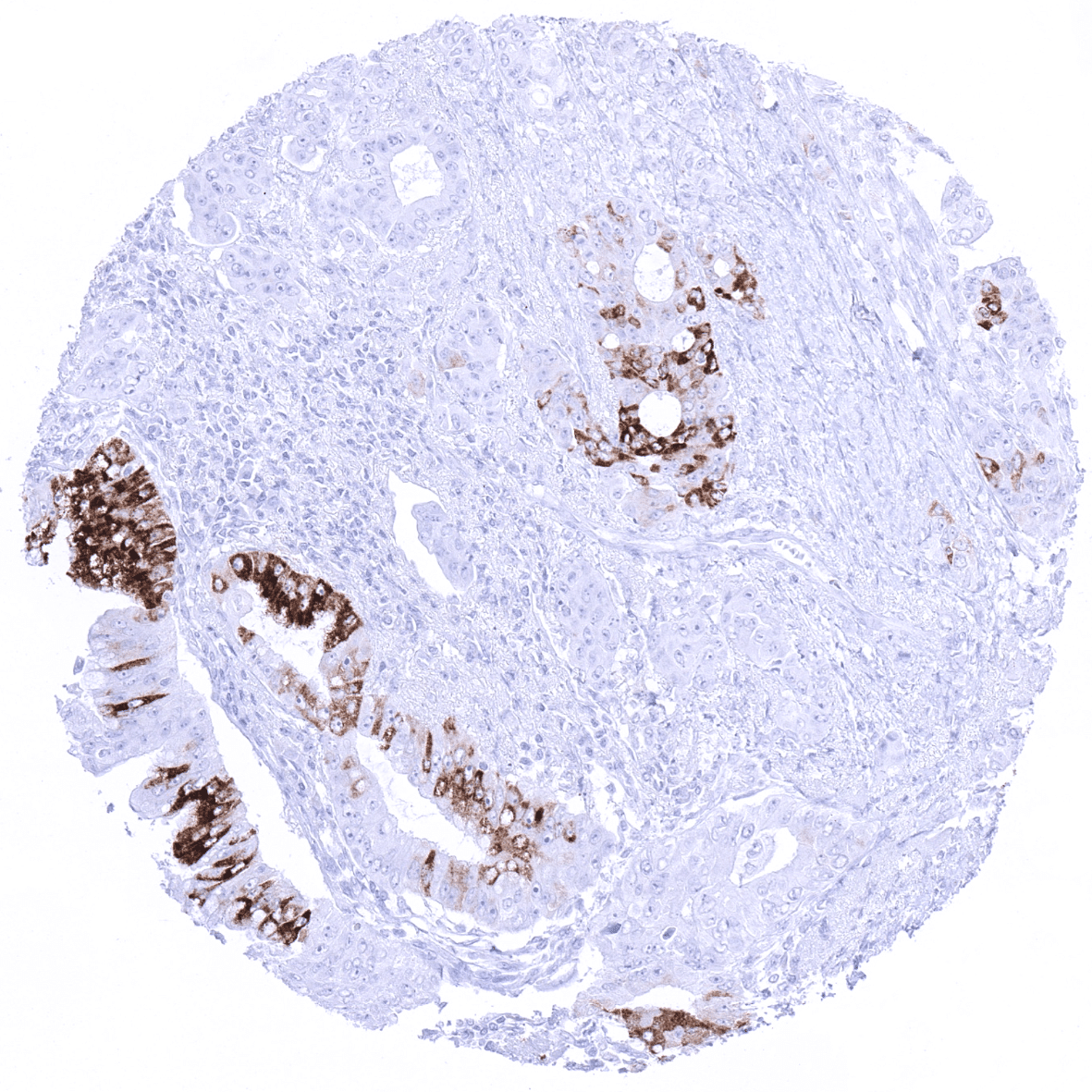
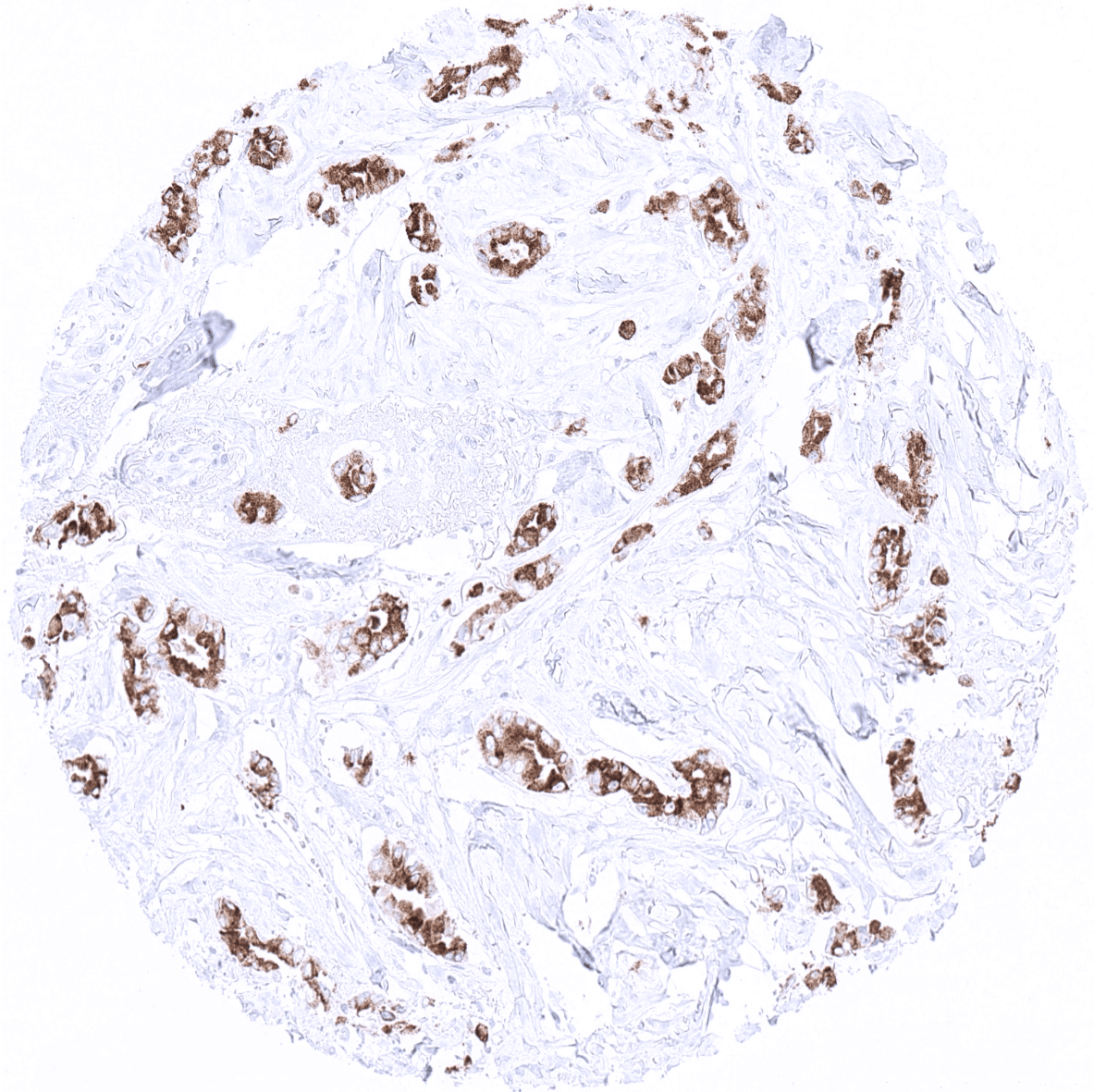
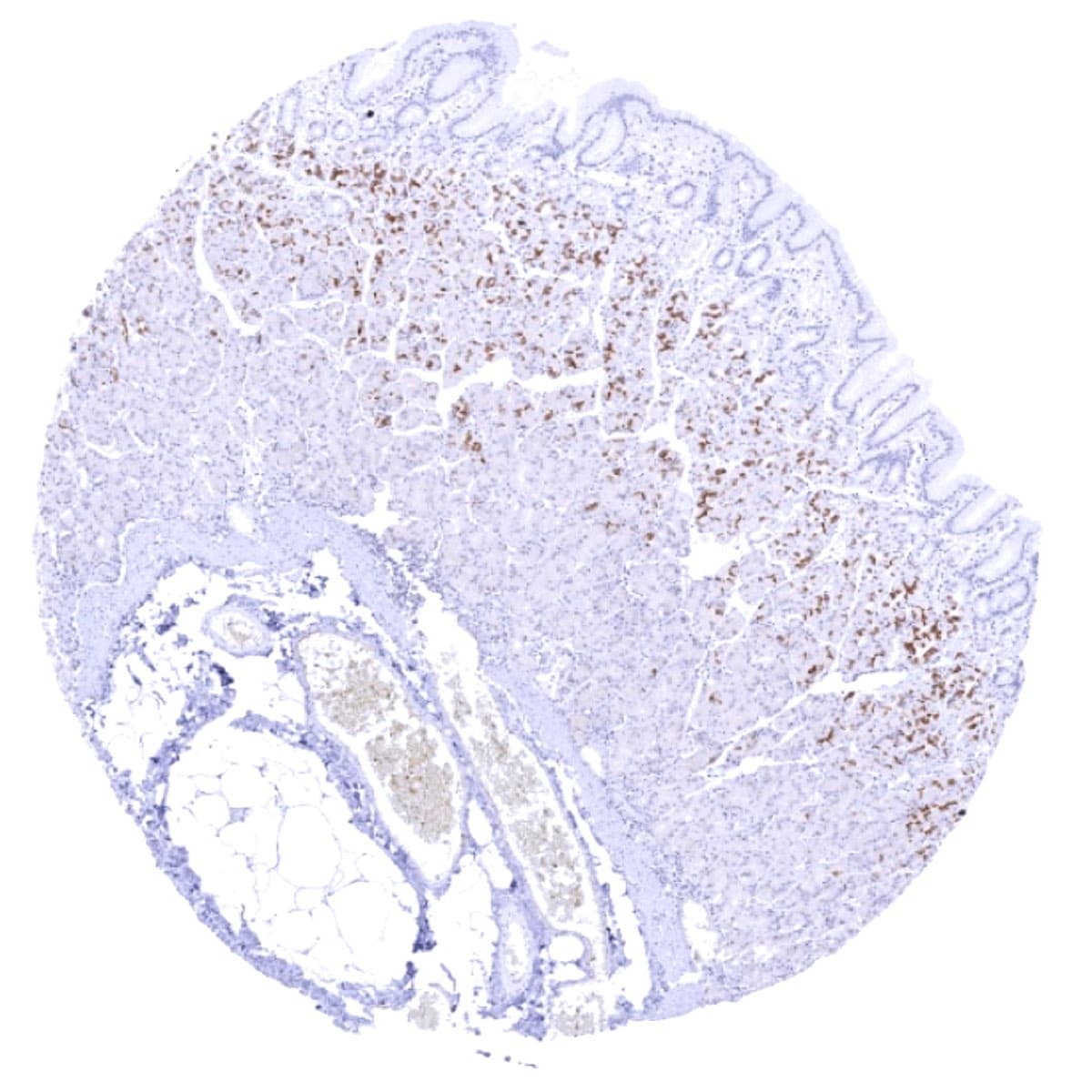
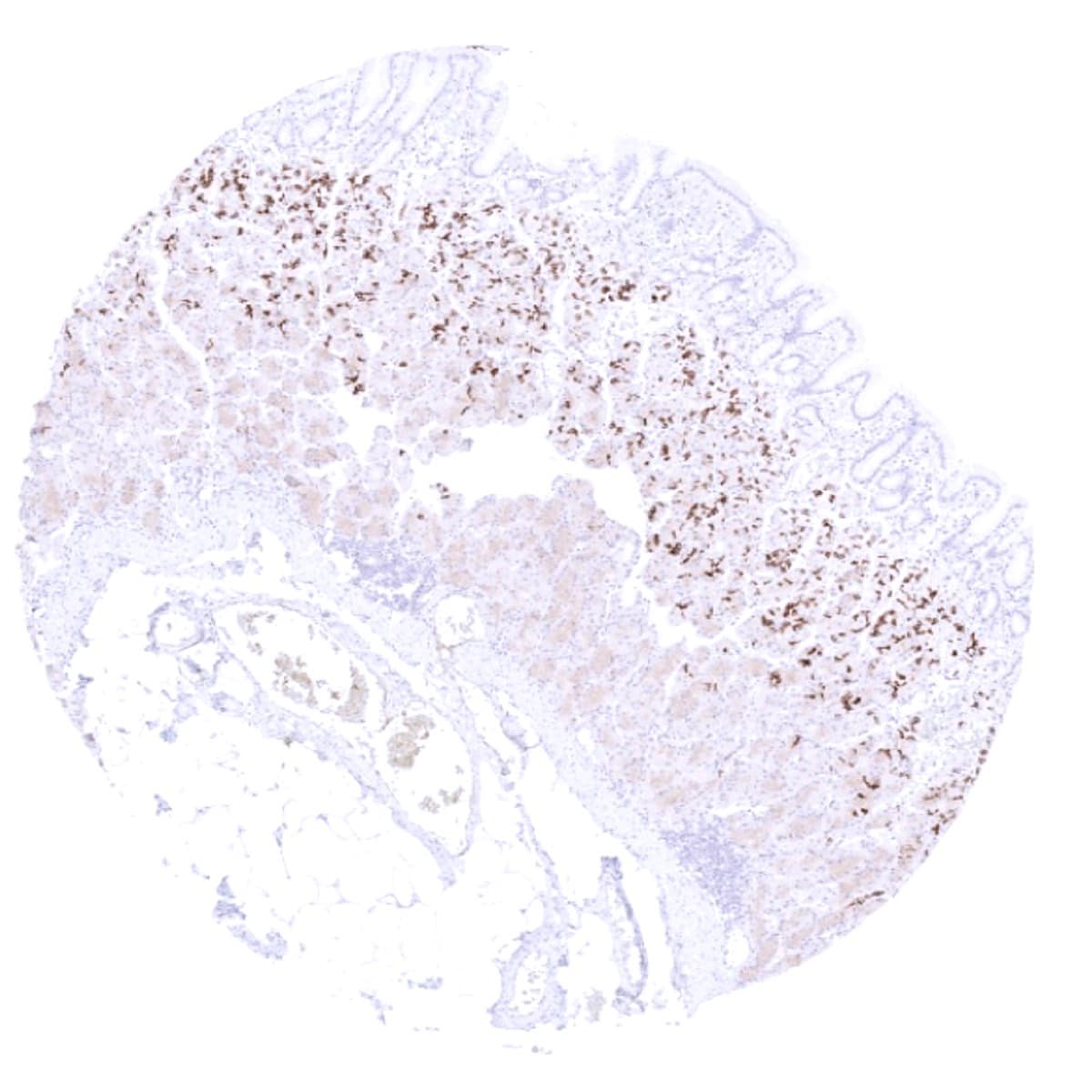
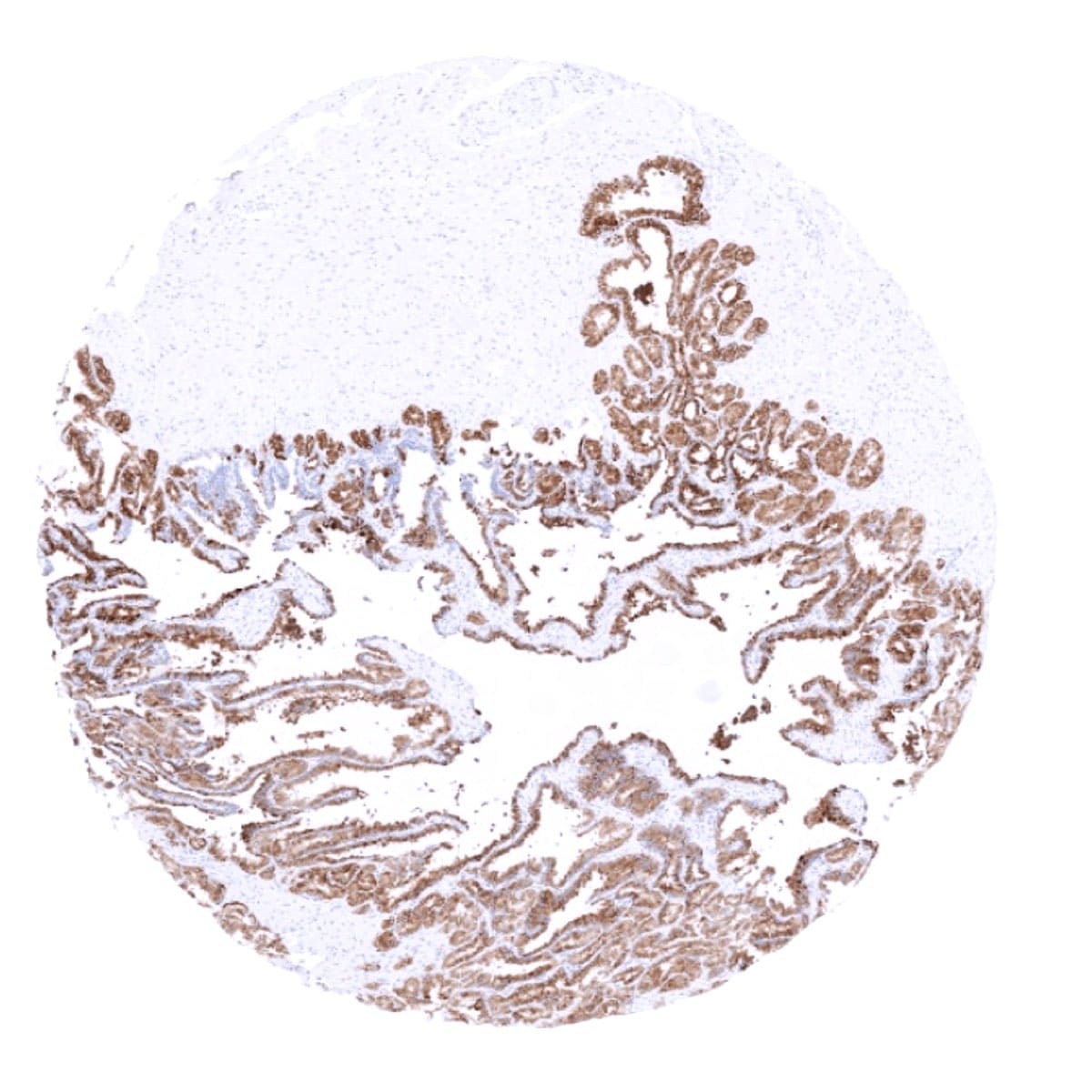
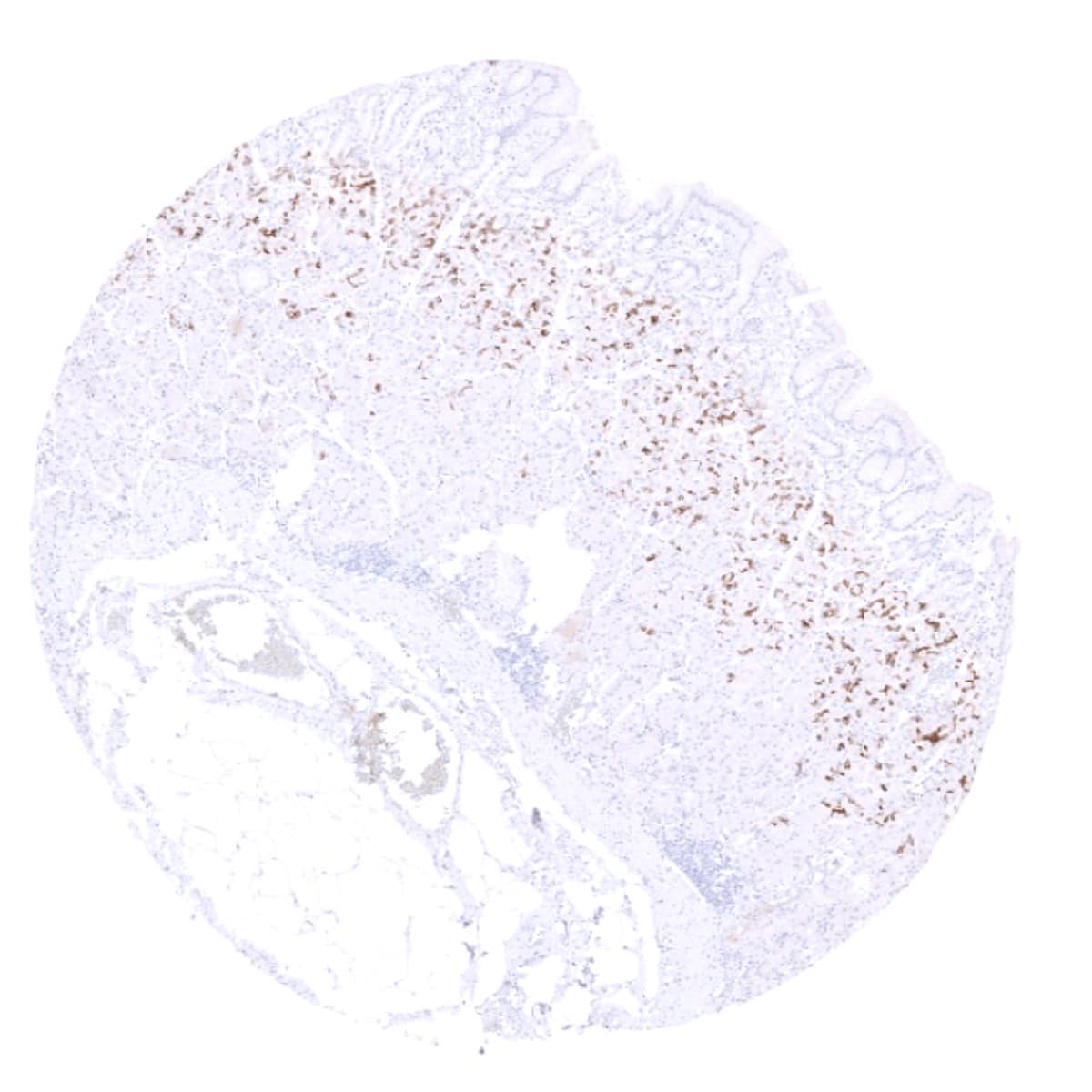
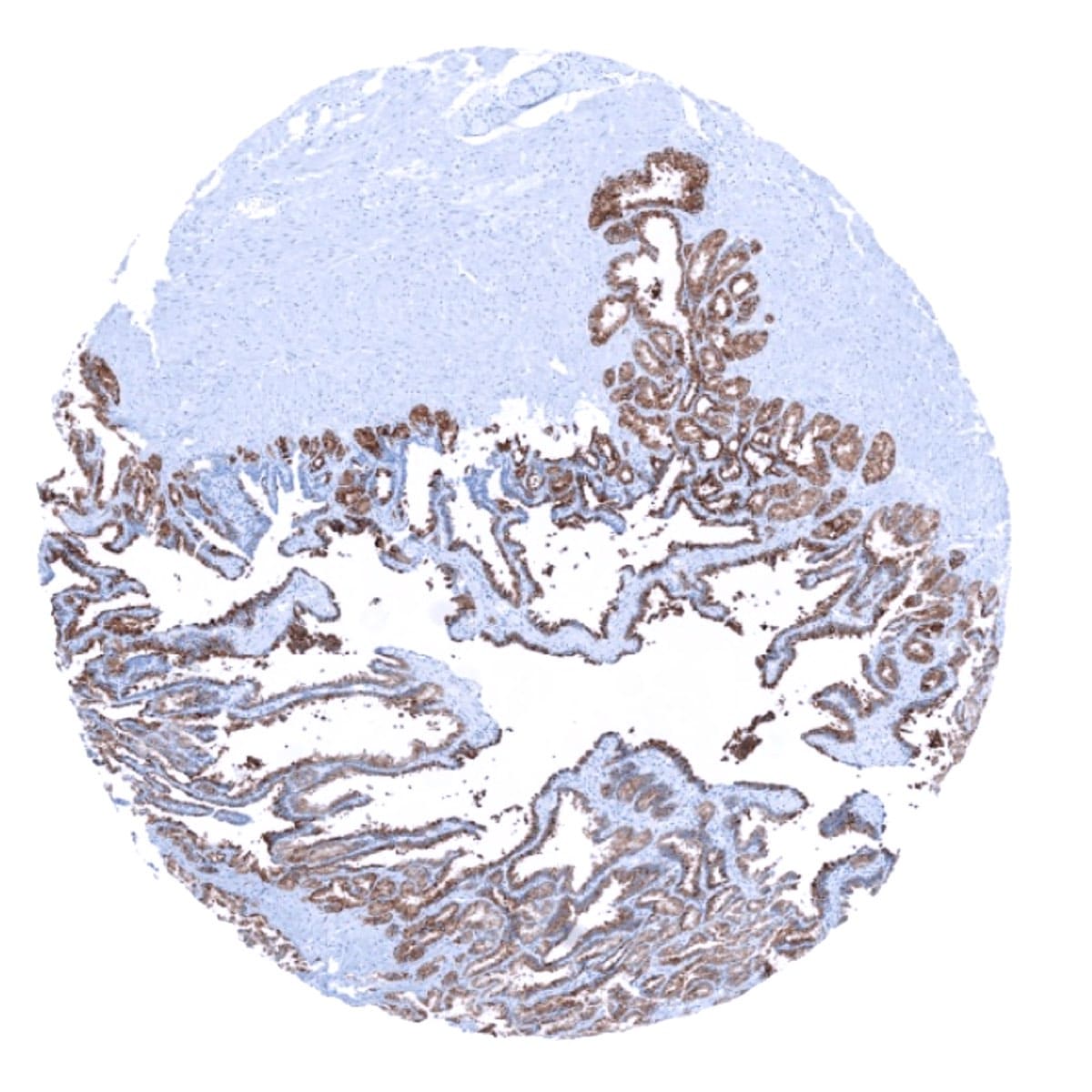
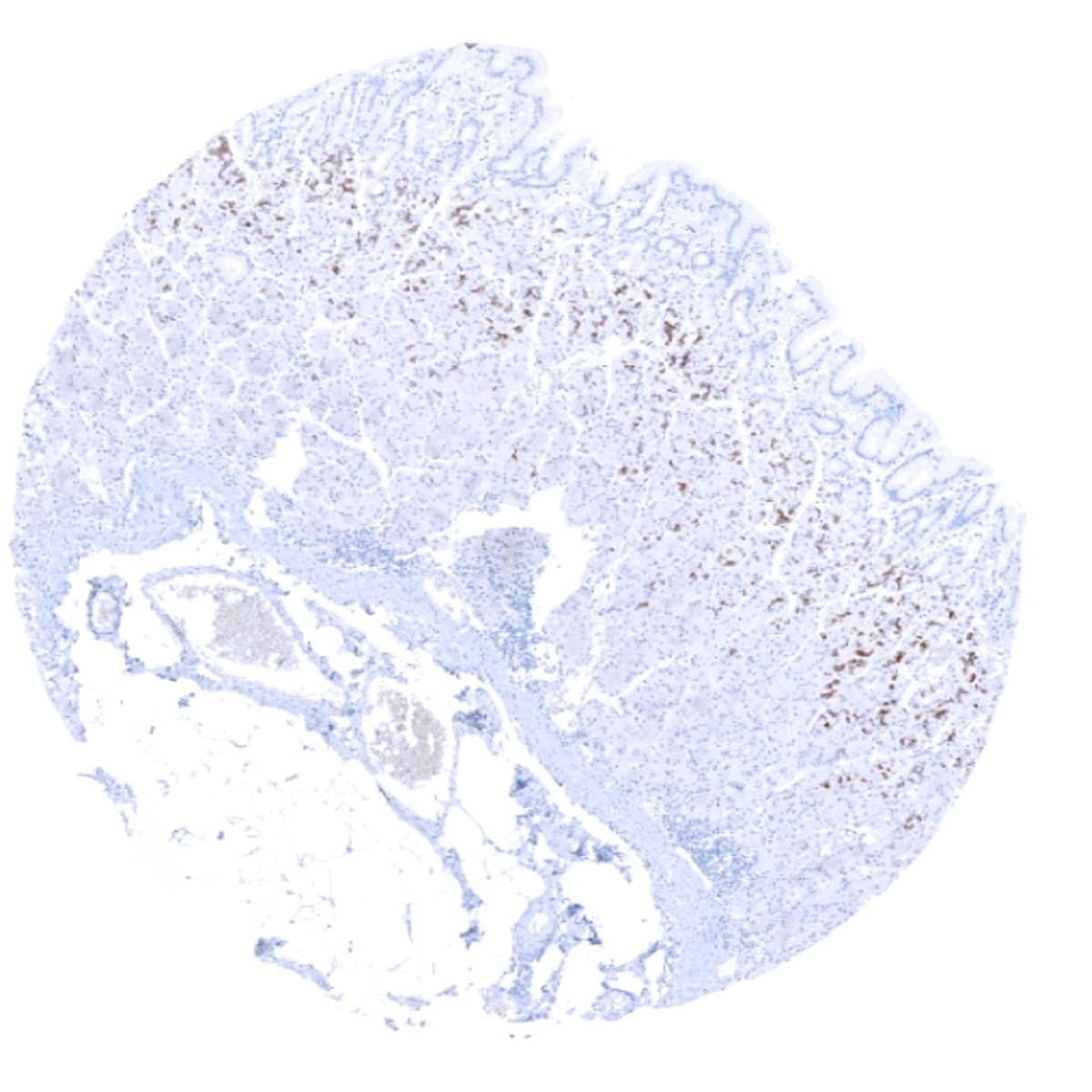
MUC6 can be expressed in various tumor types including for example pancreatic, breast, ovarian, endometrial, stomach, colorectal, and cholangiocellular carcinoma. In principle, three different patterns can be seen: diffuse staining of all cells, patchy focal staining of tumor areas that sometimes exhibit a different morphology as compared to non-stained areas groups, and a mosaic pattern containing a variable number of scattered strongly MUC6 positive cancer cells quite regularly distributed between clearly negative tumor cells.
The TCGA findings on MUC6 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
MUC6 (MSVA-806R) publication summary
Relevant publication: Dwertmann Rico et al. “Pattern of MUC6 expression across 119 different tumor types: A tissue microarray study on 15 412 tumors” Published in Pathol Int. 2023 Jul;73(7):281-296. PMID: 37057870
A total of 11,685 tumors from 119 different tumor categories were successfully analyzed by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. MSVA-806R, at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
Overall, 50 of 119 tumor categories showed a detectable MUC6 staining of at least one tumor with 33 tumor categories showing at least in one case a strong positivity. The highest positivity rates occurred in mucinous carcinomas of the breast (44%), gastric adenocarcinomas (30%–40%), esophageal adenocarcinomas (35%), neuroendocrine carcinomas of the colon and gallbladder (33% each), endometrioid carcinomas of the ovary (29%), tubular carcinomas of the breast (29%), ductal adenocarcinomas of the pancreas (28%), endometrioid endometrial carcinomas (24%), carcinosarcomas of the ovary (24%), and lobular carcinomas of the breast (21%). The distribution of positive staining results is shown in an “organ-systematic” (Figure 1) and in a “ranking order” figure (Figure 2) below (images based on data from Dwertmann Rico et al). Data on associations with histopathological and clinical parameters are also summarized below (Figure 3; based on data described by Dwertmann Rico et al).
Authors conclusions on diagnostic utility of MUC6 IHC with respect to the distinction of different tumor entities (Dwertmann Rico et al.):
- The broad range of tumor types with MUC6 expression limits the utility of MUC6 immunohistochemistry for the distinction of different tumor types.
Authors conclusions on the prognostic role of MUC6 immunostaining results (Dwertmann Rico et al.):
- In colorectal cancer, strong MUC6 staining was linked to advanced pT stage (p = 0.0464), defective mismatch repair status and right‐sided tumor location (p < 0.0001 each).
- In breast carcinomas of no special type, strong MUC6 staining was associated with high tumor grade (p = 0.0291), nodal metastasis (p = 0.0485), HER2 positivity (p < 0.0001), ER negativity (p = 0.0332), and PR negativity (p = 0.0257).
Figure 1. MUC6 staining in cancer (“organ-systematic”; according to Dwertmann Rico et al.)

Figure 2. MUC6 staining in cancer (“ranking list”; according to Dwertmann Rico et al.)

Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-806R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Agilent / Dako – Autostainer Link 48
Pretreatment in PT-Link for 30 minutes at 95°C (pH high); FLEX peroxidase blocking for 5 minutes (room temperature), MSVA-806R 1:100 for 20 minutes (room temperature), FLEX+ mouse/rabbit (LINKER) for 15 minutes (room temperature), horseradish peroxidase (HRP) for 20 minutes (room temperature), FLEX DAB+Sub-Chromo for 10 minutes (room temperature), FLEX hematoxylin for 5 minutes (room temperature).
These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, and a longer incubation time of FLEX+LINKER result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Leica – BOND RX
Dewax at 72°C for 30 seconds; Pretreatment in Bond Epitope Retrieval Solution (ER2 – EDTA pH9) for 20 minutes at 100°C; Peroxidase blocking for 5 minutes (room temperature), MSVA-806R 1:150 for 15 minutes (room temperature), Post primary (rabbit anti mouse) for 8 minutes (room temperature), Polymer (goat anti rabbit) for 8 minutes (room temperature), mixed DAB refine for 10 minutes (room temperature), hematoxylin for 5 minutes (room temperature).

These images reflect stainings by the protocol described above. It is of note that a comparable staining result can also be obtained by different protocols. In general, a longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of Post primary and or the Polymer result in stronger staining, potentially at the cost of more background staining. Modifications of the protocol with a strengthening effect on staining intensity in combination with changes of other parameters that result in lower staining intensity can result in a comparable result as shown above.
Roche – Ventana Discovery ULTRA
Pretreatment for 64 minutes at 100°C (pH 8,4); CM peroxidase blocking for 12 minutes (room temperature), MSVA-806R 1:150 for 20 minutes at 36°C, secondary antibody (anti-rabbit HQ) for 12 minutes at 36°C, anti-HQ HRP for 12 minutes at room temperature, DAB at room temperature, hematoxylin II at room temperature for 8 minutes, bluing reagent at room temperature for 4 minutes.
These images depict staining results obtained by the protocol described above. It is of note, that the Ventana machines generally require higher antibody concentrations than other commonly used autostainers because the antibodies are automatically diluted during the procedure. Various other protocols can result in an identical result as shown above. A longer pretreatment, a longer incubation time of the primary antibody, a higher antibody concentration, a higher temperature during incubation, and a longer incubation time of secondary antibody and or the anti-HQ HRP result in stronger staining, potentially at the cost of more background staining.
Impact of pH

For antibody MSVA 806R pH9 is optimal but pH7,8 results in only slightly weaker stainings. At pH6, MUC6 immunostaining is markedly reduced.
Potential Research Applications
- A comprehensive study analyzing MUC6 expression in various different tumor entities would be helpful to assess the diagnostic significance of MUC6 IHC.
- The clinical significance of MUC6 expression in various cancer entities is unclear.
Evidence for Antibody Specificity in IHC
Specificity of MSVA-806R is documented by strong positive staining in cell types that are well documented to express MUC6 such as glandular but not surface epithelium of the stomach, Intercalated and interlobular ducts of the pancreas, and seminal vesicle. The complete absence of MUC6 immunostaining in cell types from 70 different normal tissue types documents absence of cross-reactivity and low propensity to generate non-specific background staining for MSVA-806R.
