295,00 € – 995,00 €
Product details
Synonyms = Kallikrein related peptidase 7 (HGNC Symbol), PRSS6, SCCE
Antibody type = Mouse monoclonal / IgG
Clone = MSVA-707M
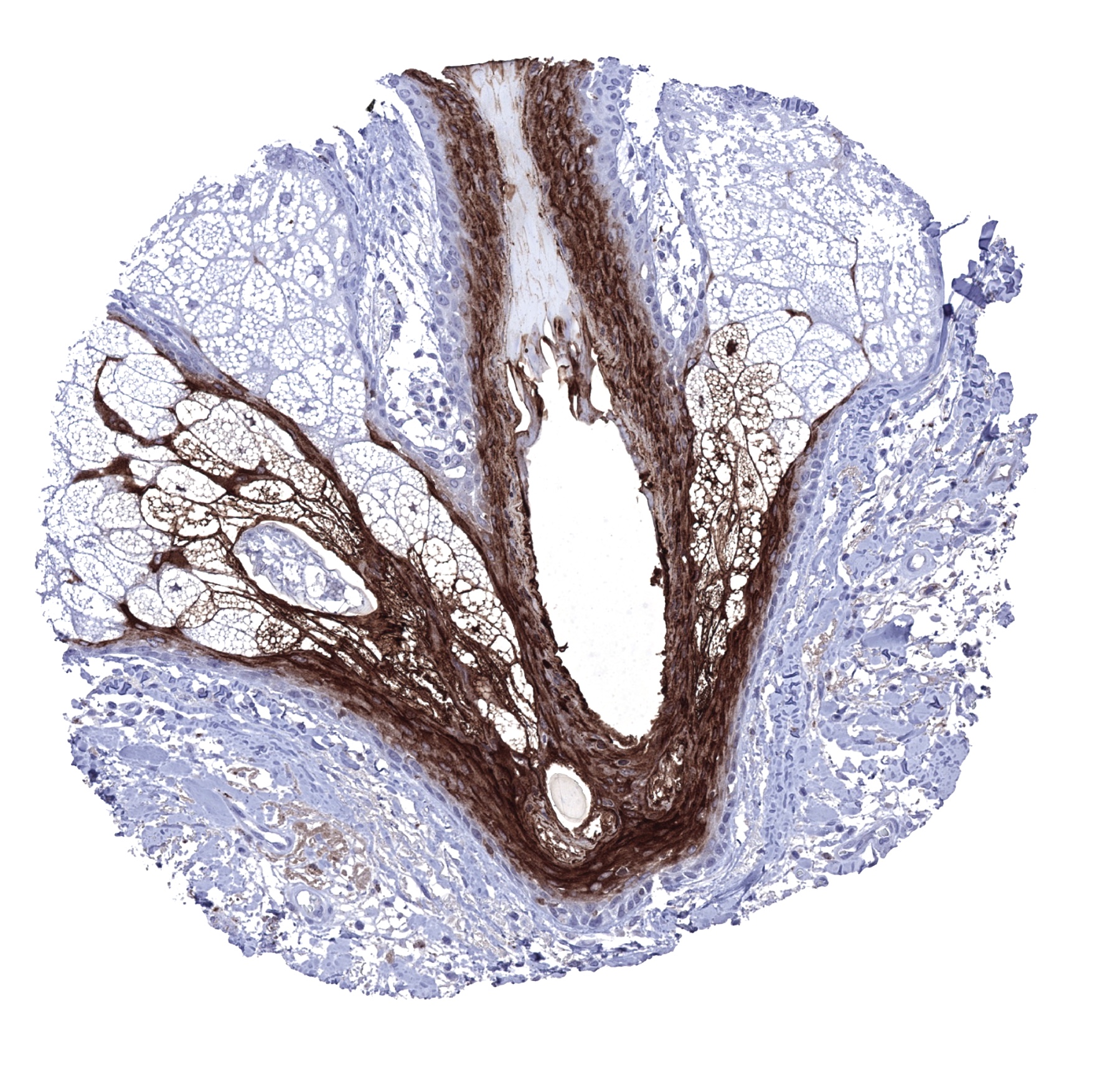
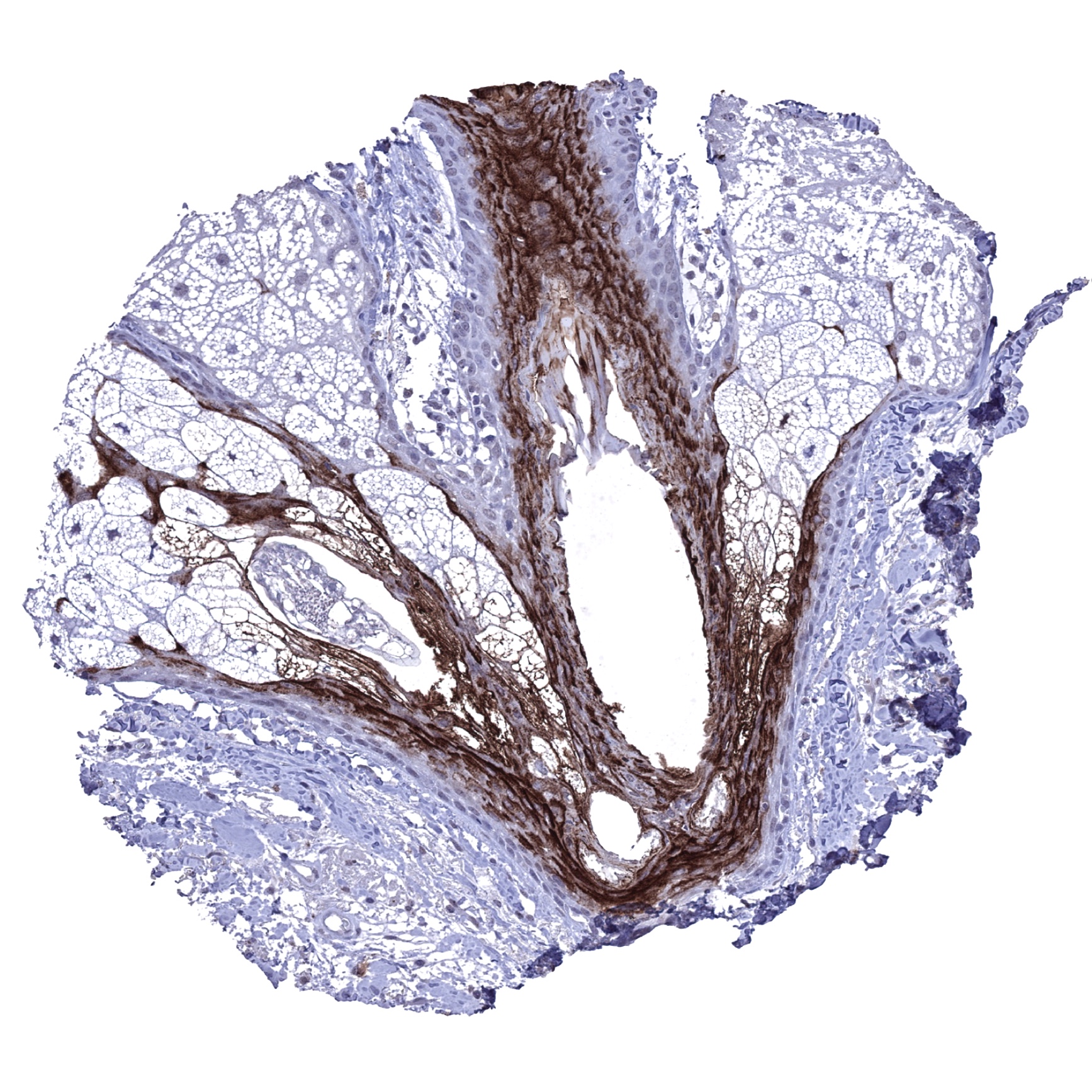
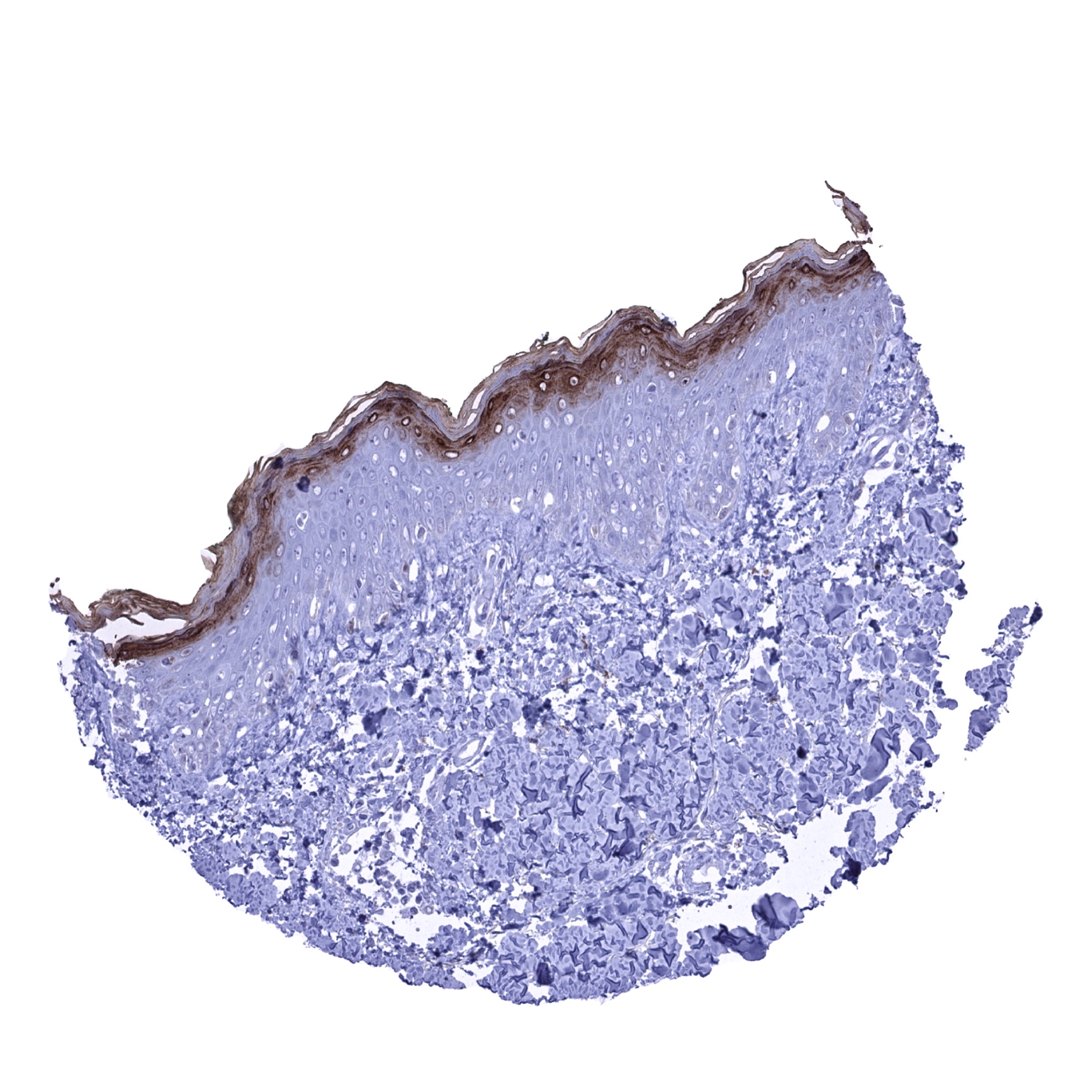
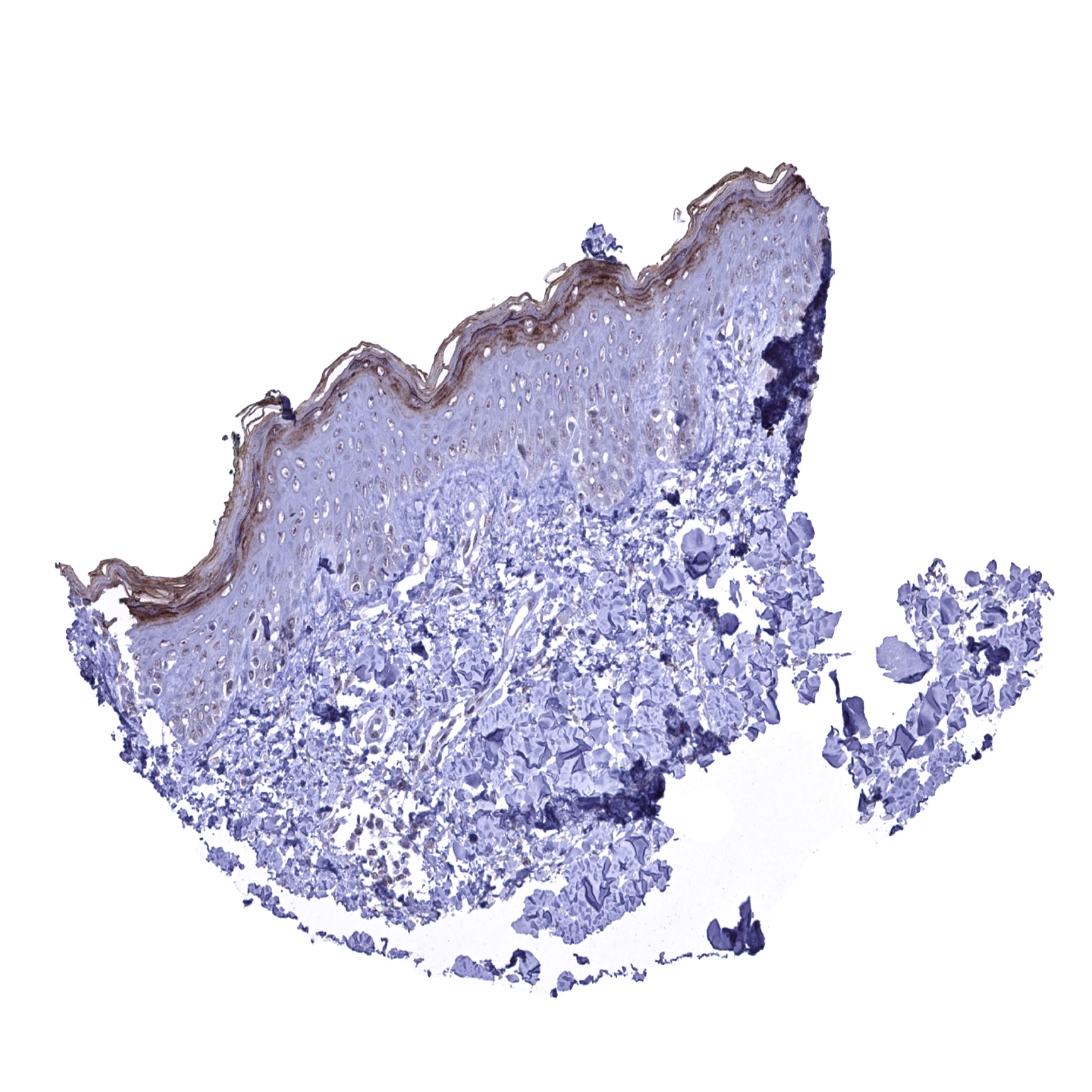
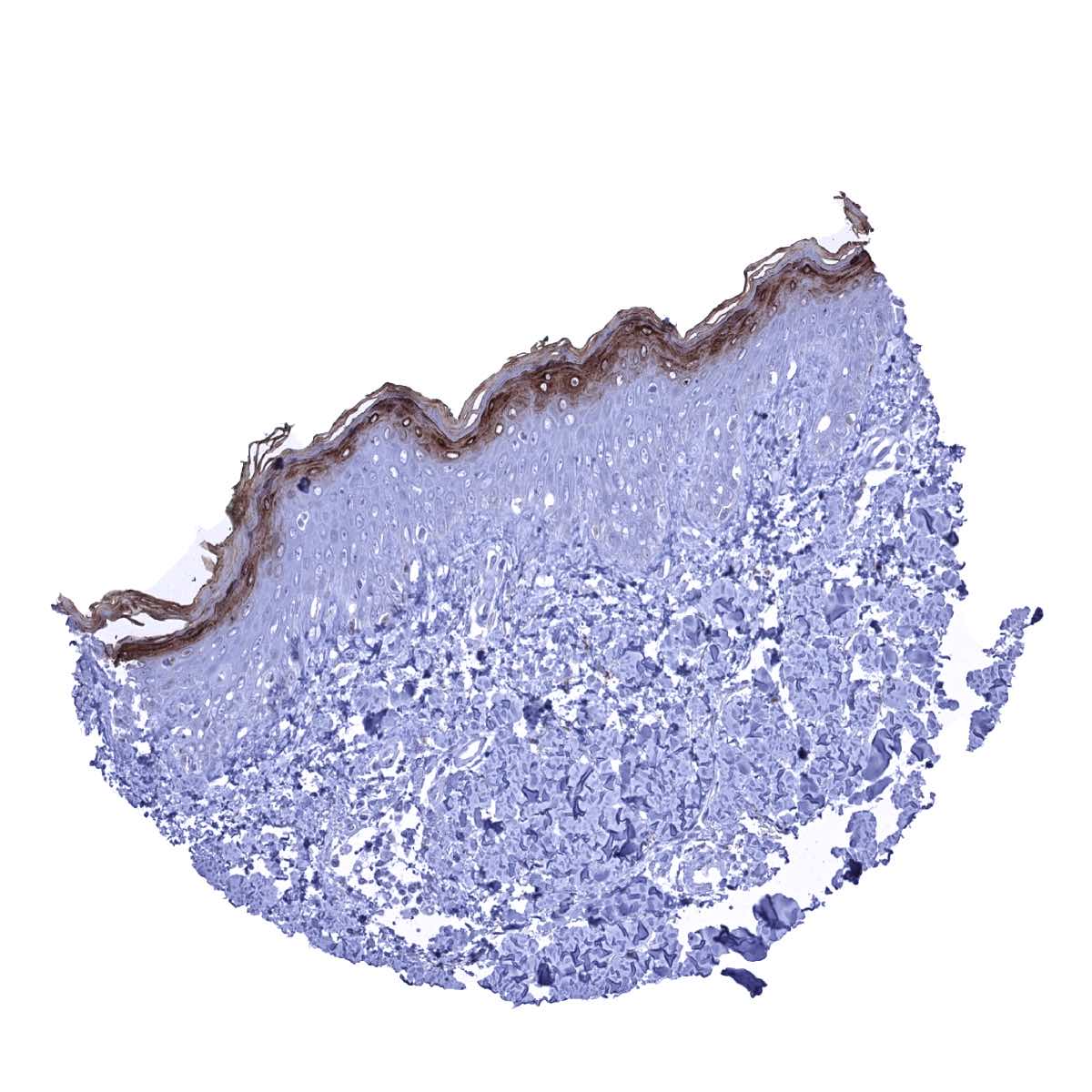
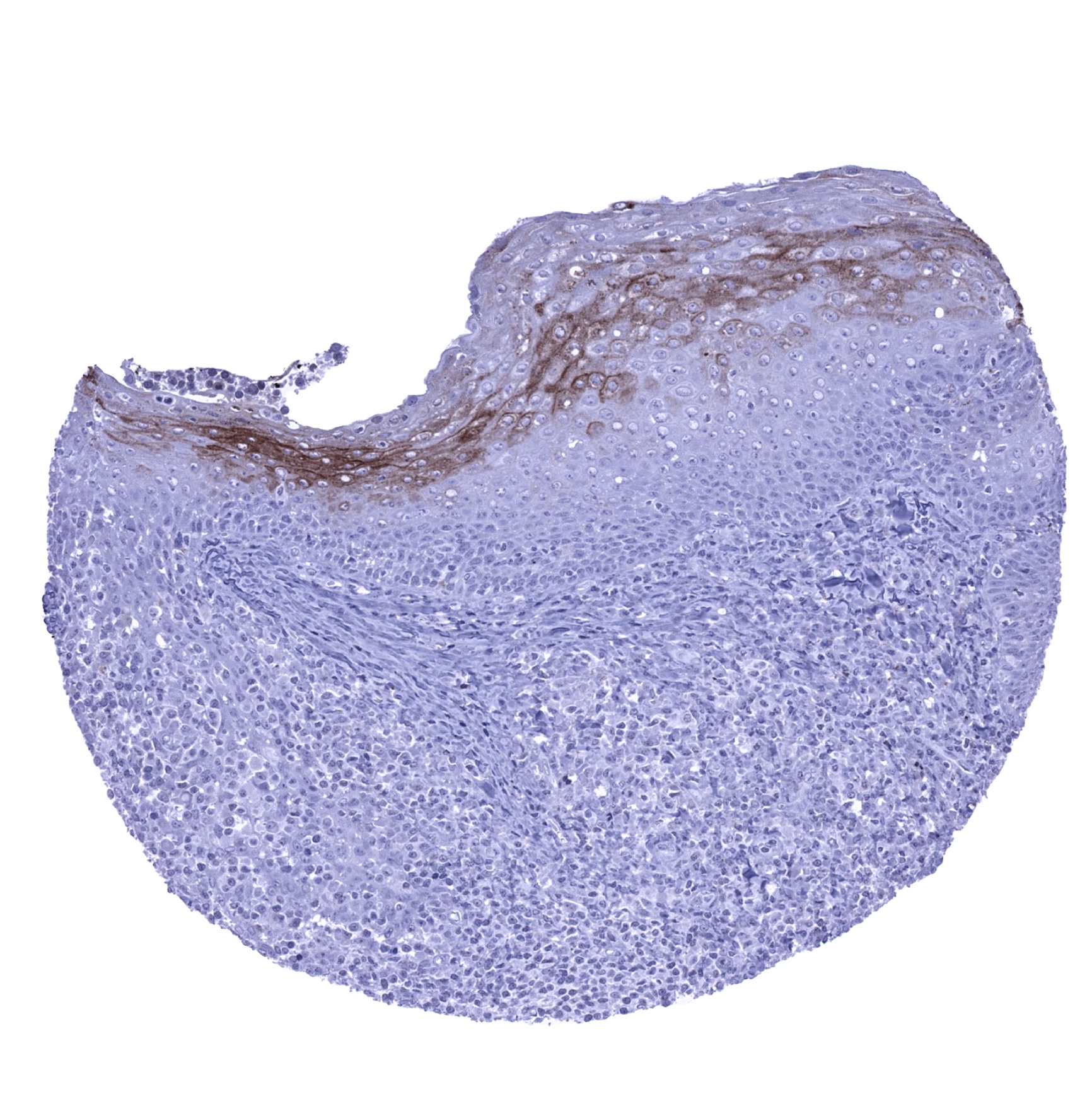
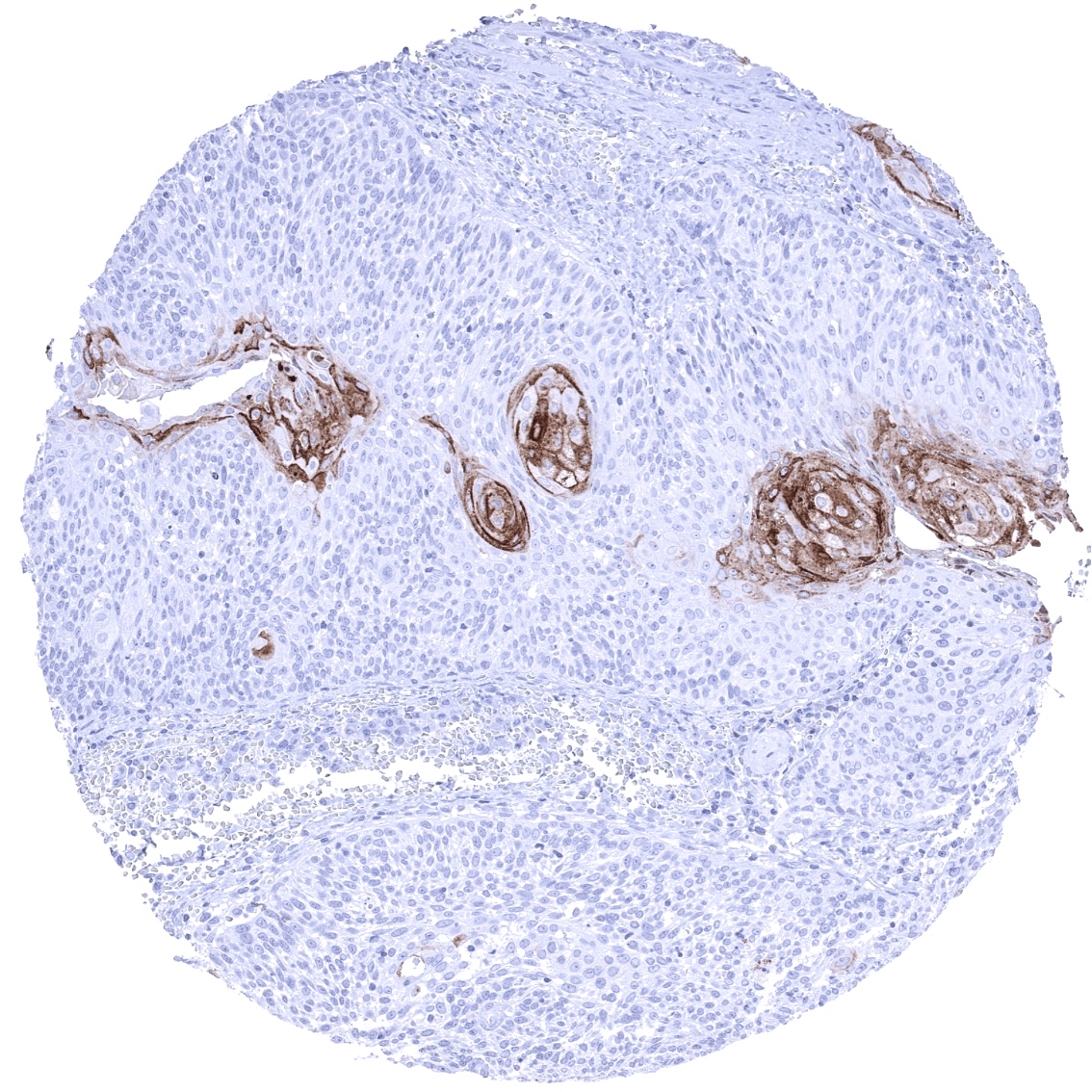
Positive control = Skin: A strong KLK7 staining should be seen in the stratum granulosum and possibly also in the keratinizing cell layers.
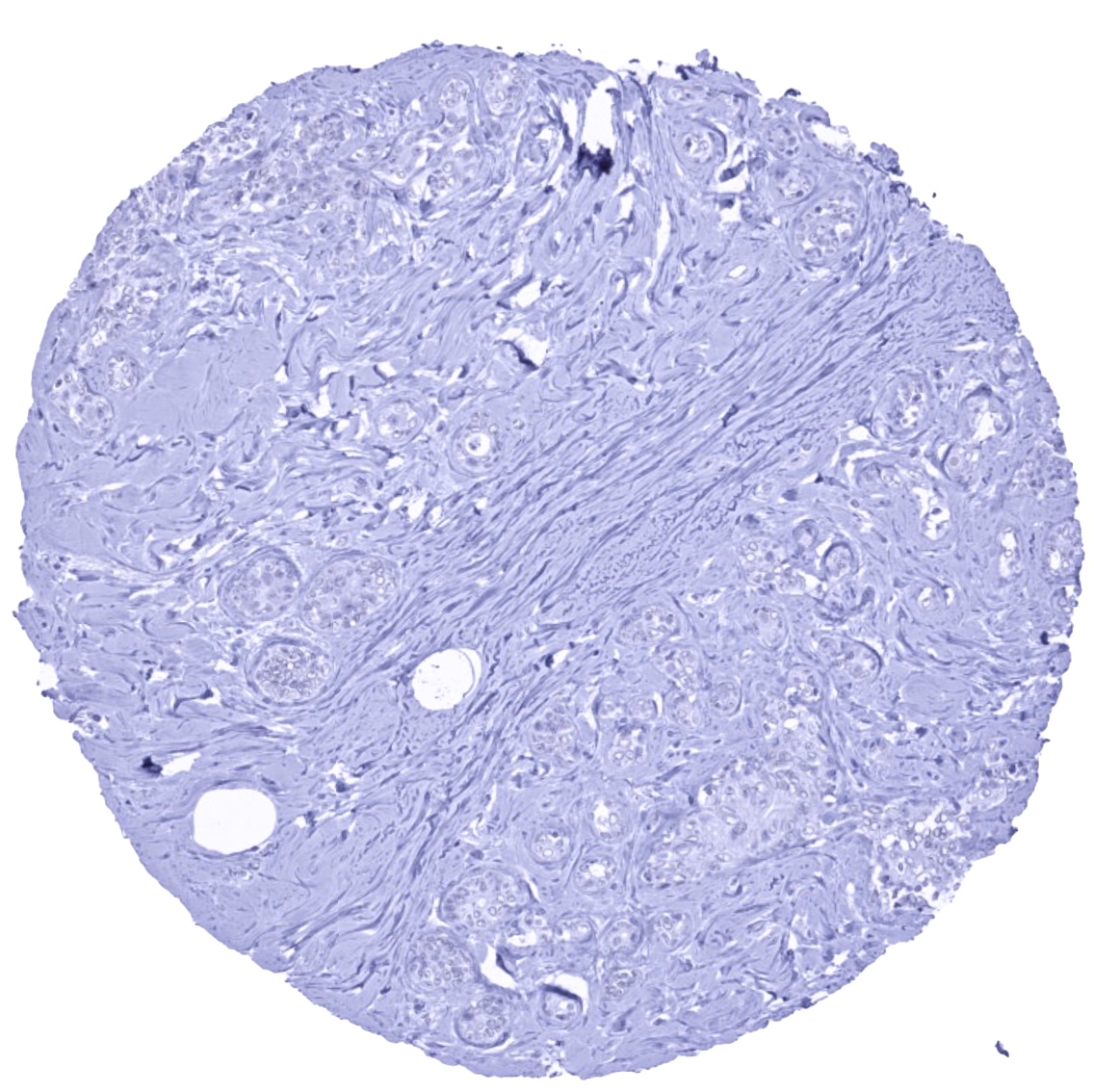
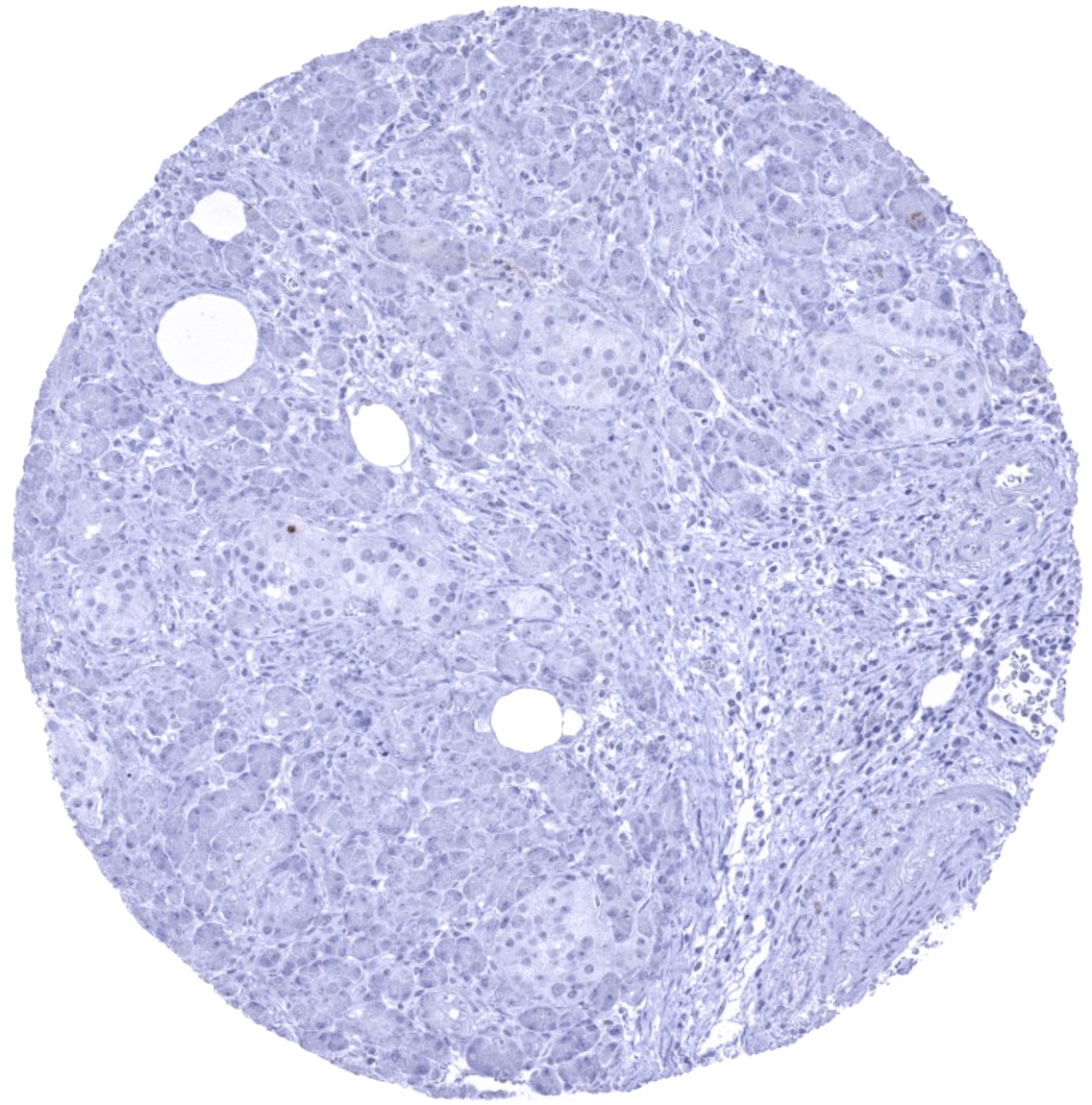
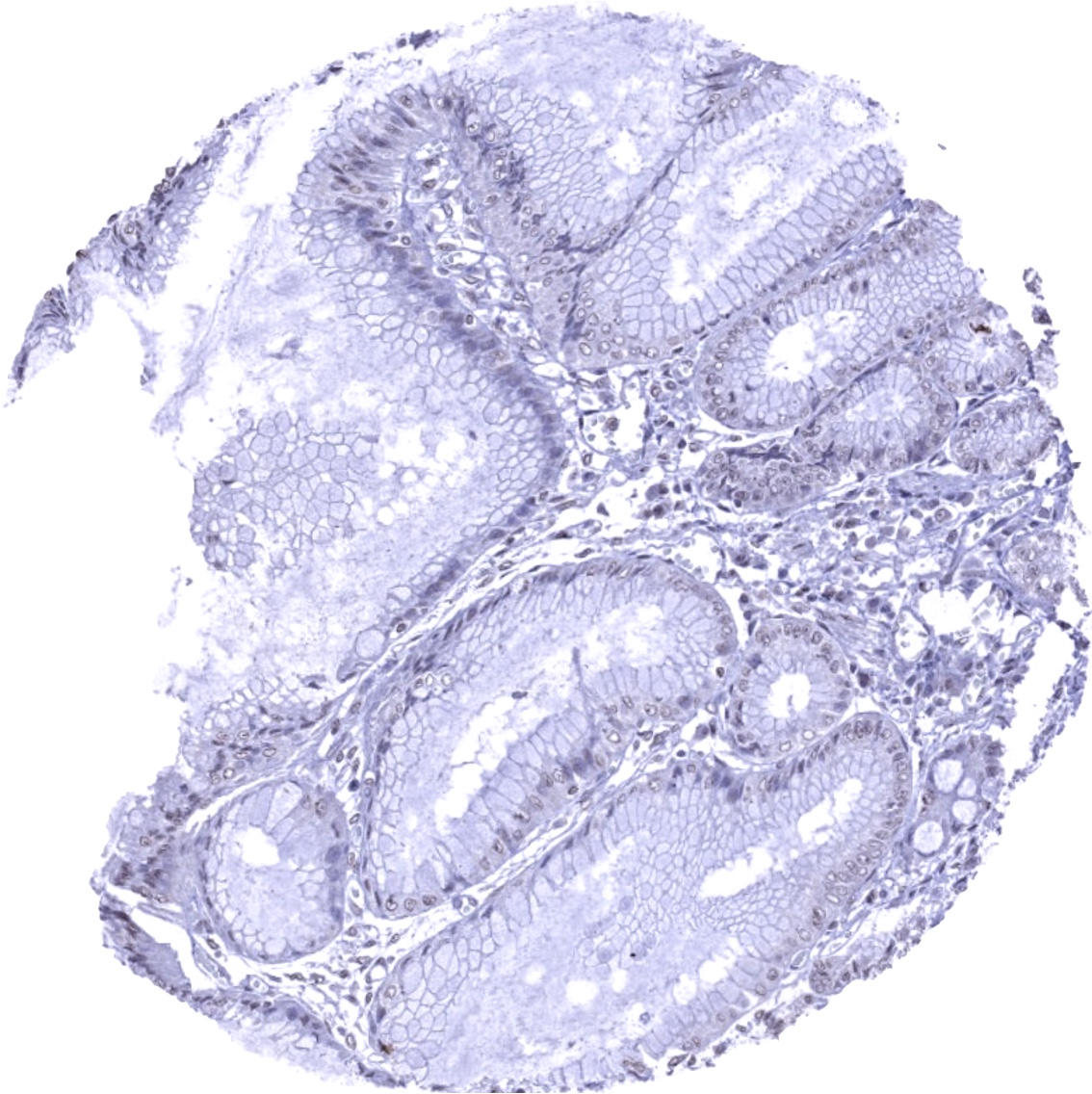
Negative control = Colon: KLK7 immunostaining should be absent in all cells of the colon mucosa.
Cellular localization = Intracelullar Secreted
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
PSA is a marker for prostatic epithelial tissue and prostate cancer.
Biology Behind
Kallikrein-related peptidase 7 (KLK7) is a 27,5 kDa chymotrypsin-like serine protease which is coded by the KLK7 gene located on chromosome 19q13. KLK7 plays a pivotal role in maintaining skin homeostasis. It is secreted into the stratum granulosum layer of the epidermis as an inactive enzyme requiring proteolytic cleavage of the N-terminal for becoming activated. Activated KLK7 triggers the proteolysis of corneodesmosomes. This enables the desquamation of corneocytes from the outer layer of the epidermis. Dysregulation of KLK7 has been associated with several skin disorders characterized by excessively dry, scaly and inflamed skin such as atopic dermatitis, psoriasis, and the Netherton syndrome. In cancer, over expression of KLK7 has been suggested to represent a possible route for metastasis due to excessive cleavage of cell junction proteins.
Staining Pattern in Normal Tissues
KLK7 staining pattern in Normal Tissues with antibody MSVA-707M (images are shown in our “Normal Tissue Gallery”)
| Brain | Cerebrum | Negative. |
| Cerebellum | Negative. | |
| Endocrine Tissues | Thyroid | Negative. |
| Parathyroid | Negative. | |
| Adrenal gland | Negative. | |
| Pituitary gland | Negative. | |
| Respiratory system | Respiratory epithelium | Negative. |
| Lung | Negative. | |
| Gastrointestinal Tract | Salivary glands | Few scattered cells can show a moderate to strong KLK7 positivity. |
| Esophagus | Weak to moderate KLK7 positivity often occurs in the superficial half of the squamous epithelium | |
| Stomach | Negative. | |
| Colon | Negative. | |
| Duodenum | Negative. | |
| Rectum | Negative. | |
| Small intestine | Negative. | |
| Liver | Negative. | |
| Gallbladder | Negative. | |
| Pancreas | Negative. | |
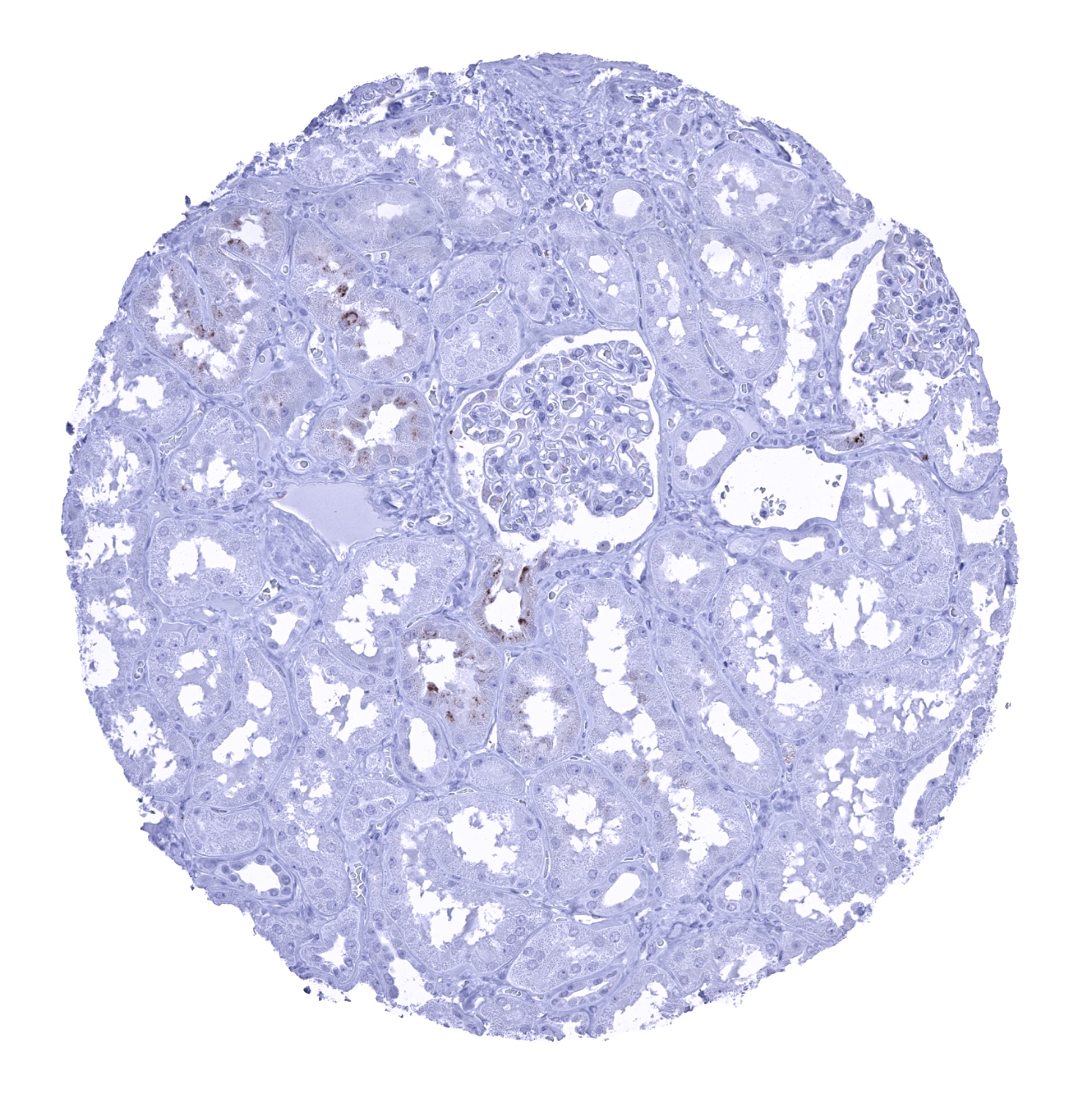
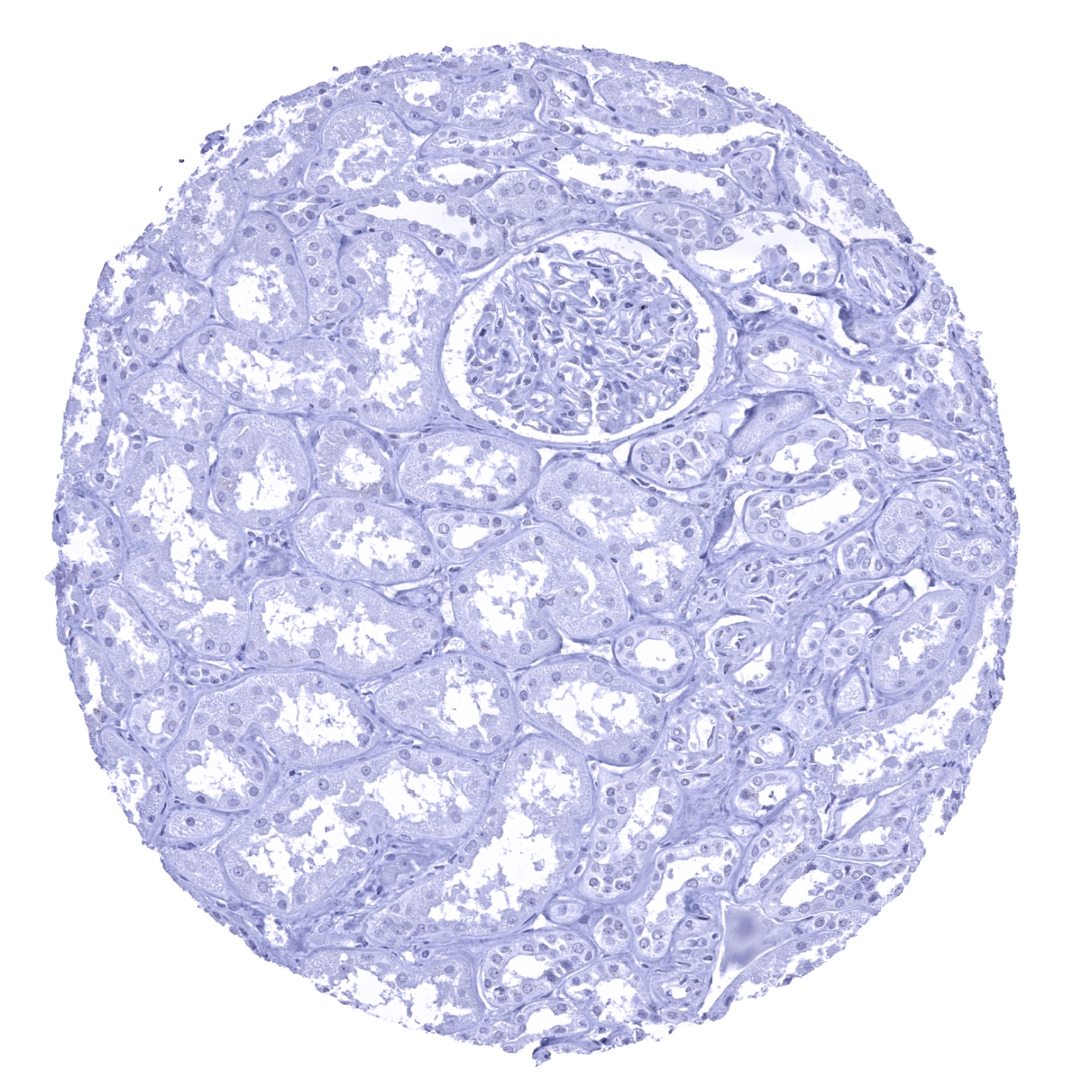
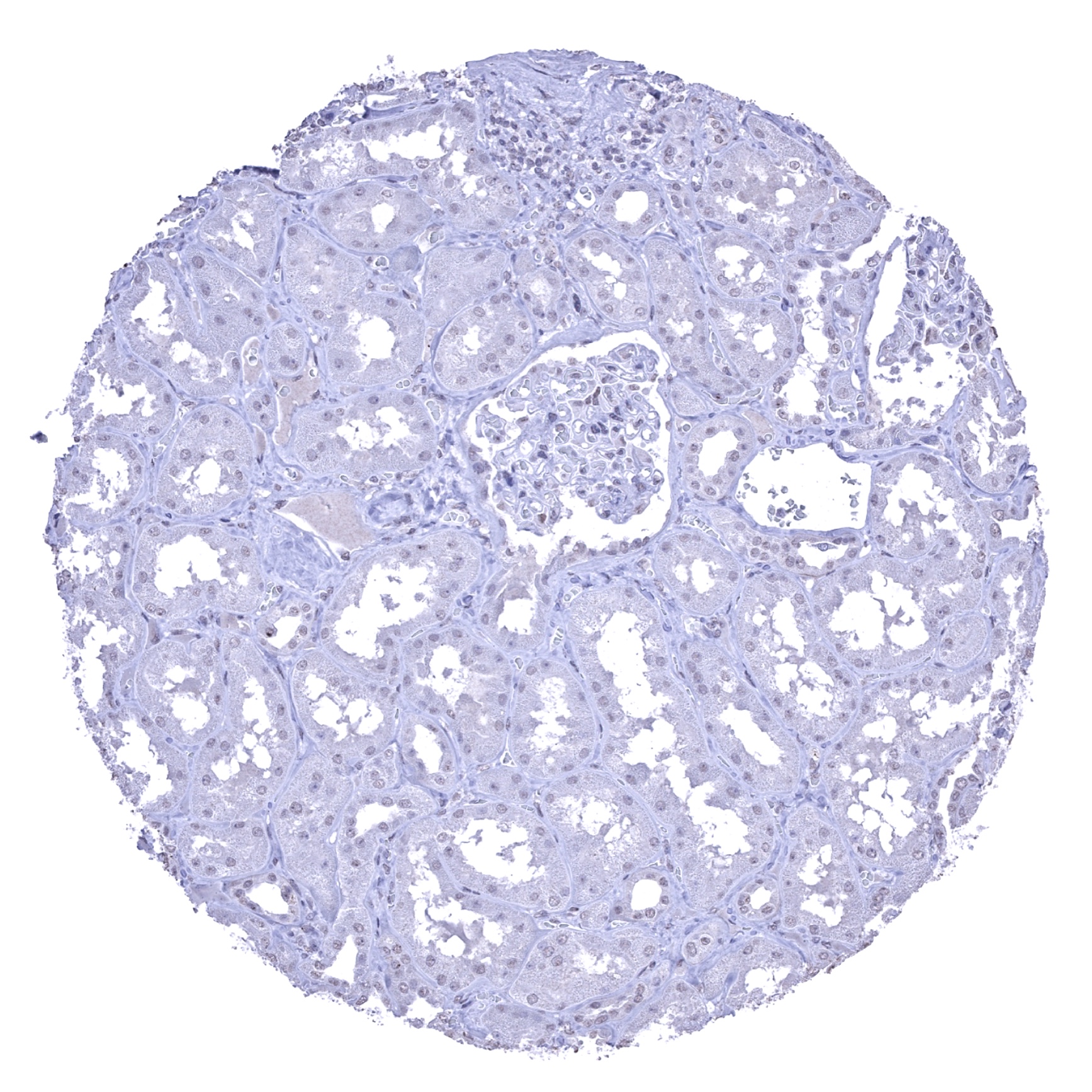
| Genitourinary | Kidney | Focal KLK7 staining in few tubuli may occur. |
| Urothelium | Negative. | |
| Male genital | Prostate | Negative. |
| Seminal vesicles | Negative. | |
| Testis | Negative. | |
| Epididymis | Negative. | |
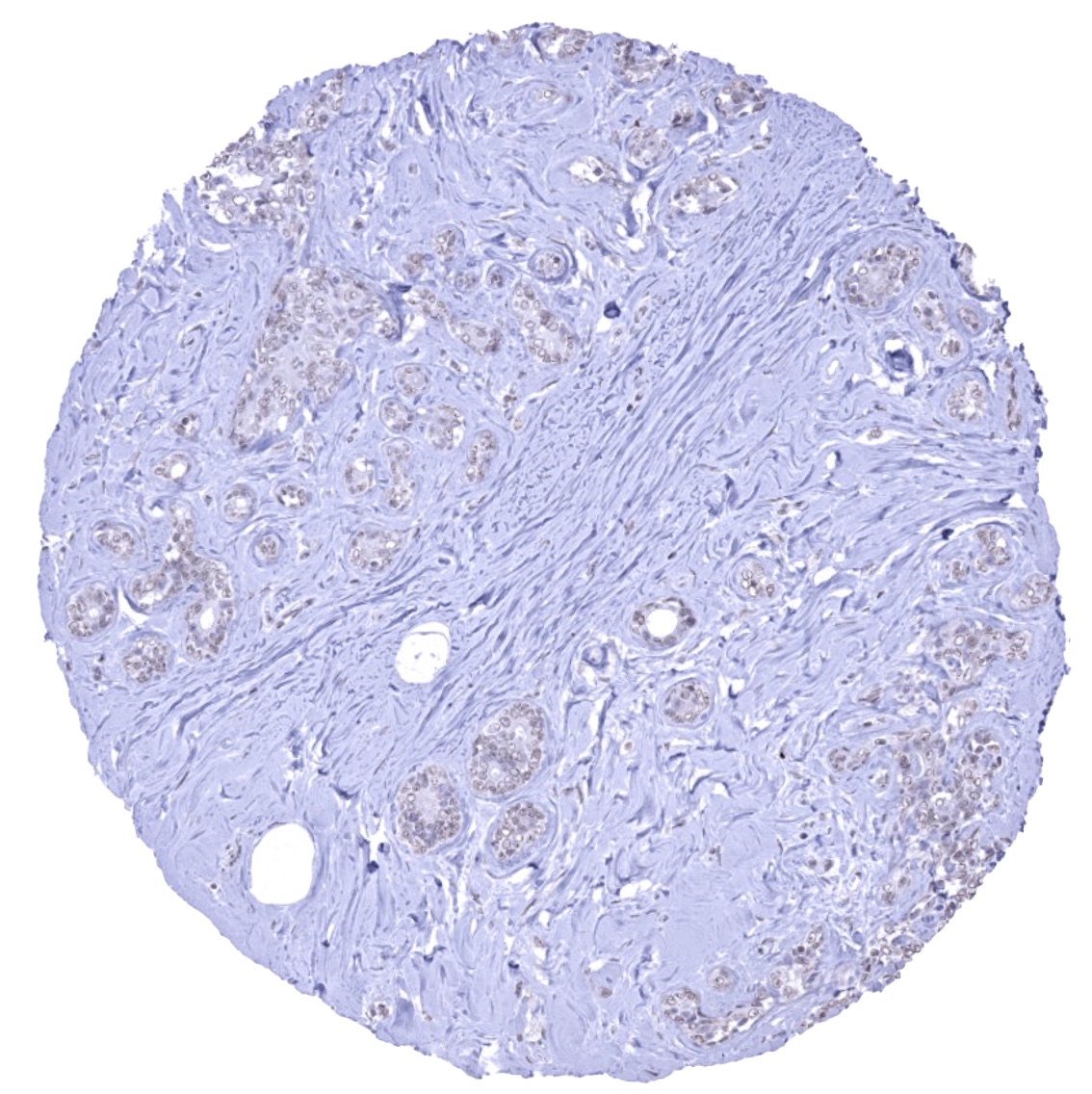
| Female genital | Breast | Negative. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | A faint KLK7 staining can occur in the upper half of the squamous epithelium. | |
| Uterus endocervix | Negative. | |
| Uterus, endometrium | Negative. | |
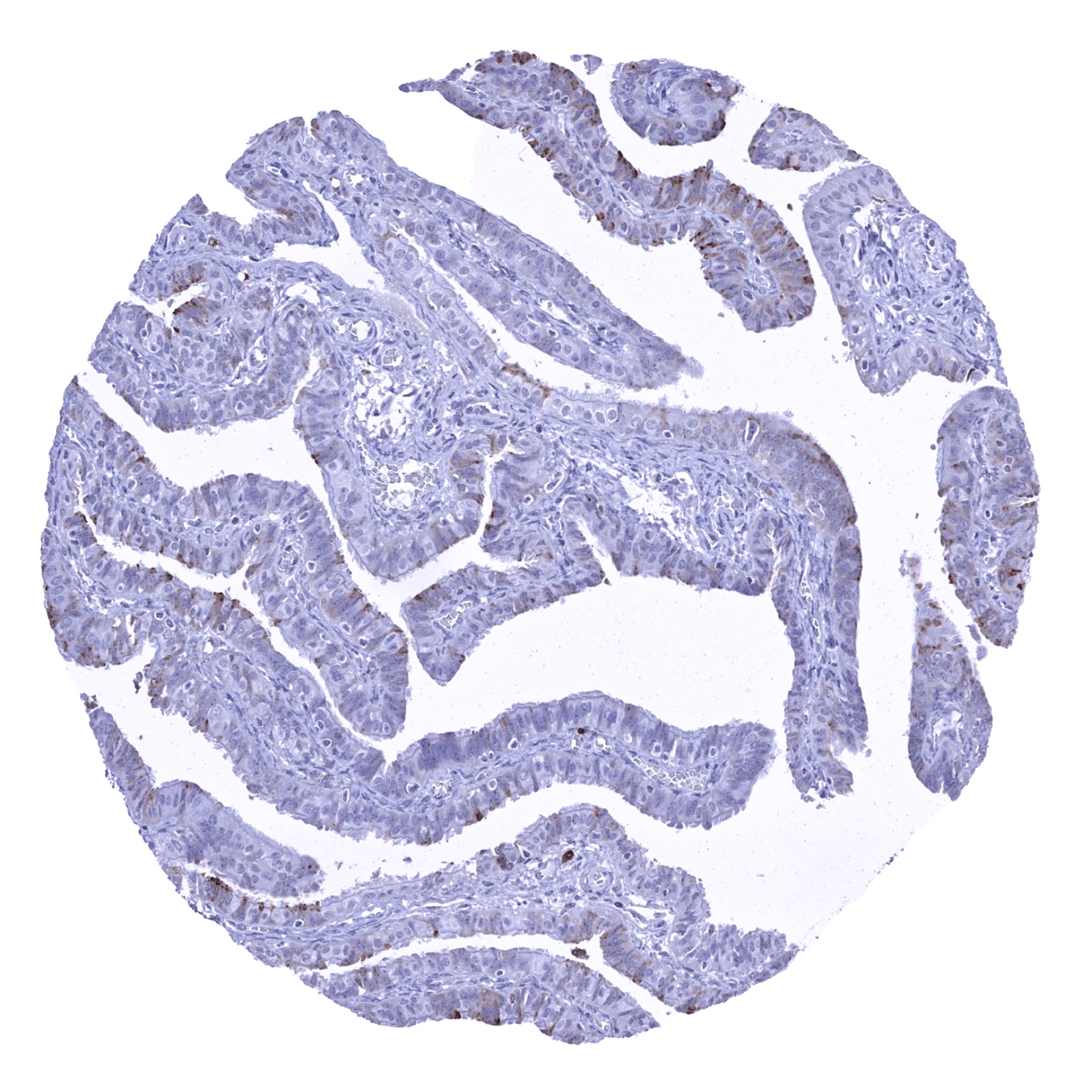
| Fallopian Tube | A predominantly apical cytoplasmic KLK7 staining in a small fraction of epithelial cells is sometimes seen. | |
| Ovary | Negative. | |
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | Negative. | |
| Chorion | Negative. | |
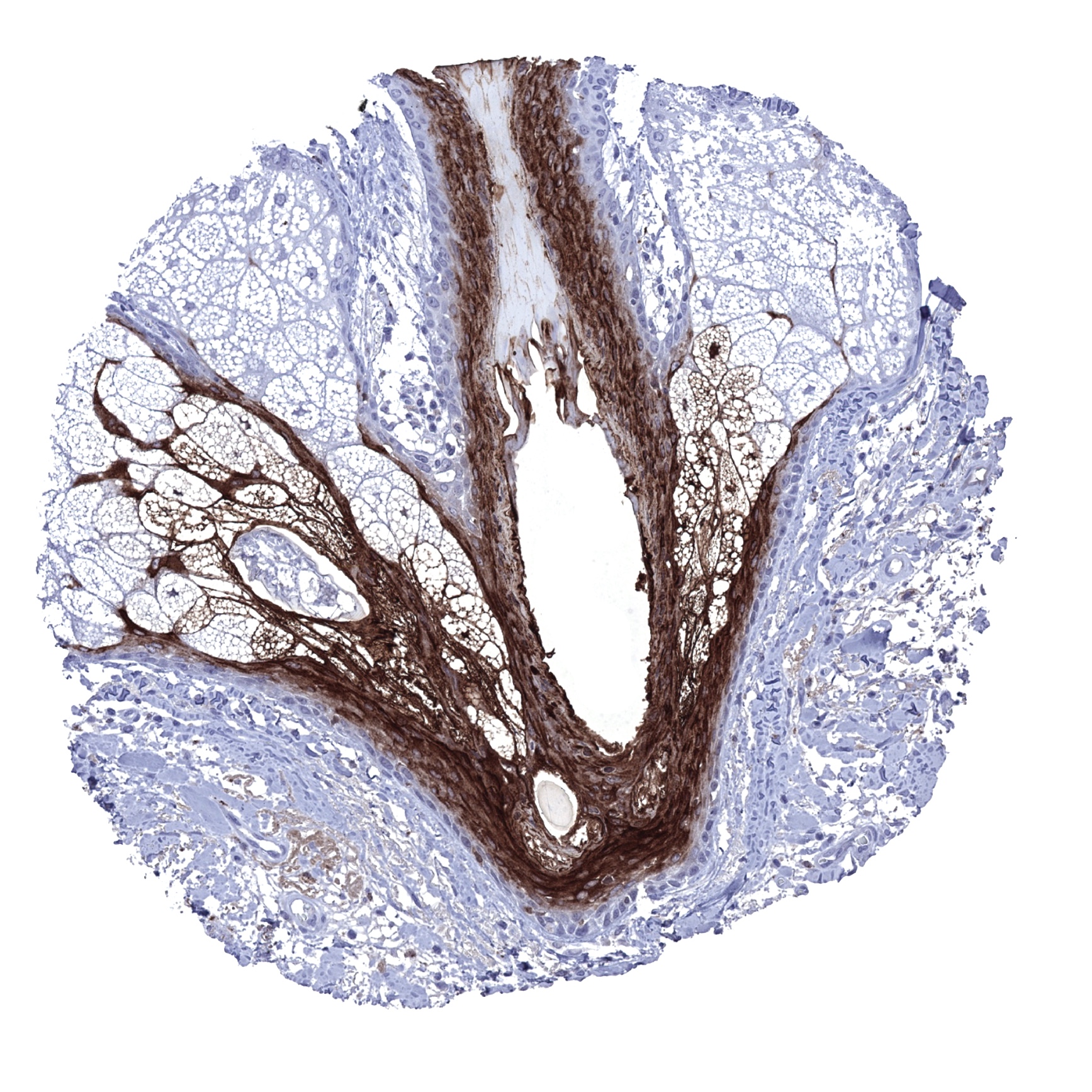
| Skin | Epidermis | Strong KLK7 staining of the stratum granulosum and of the keratinizing layer. |
| Sebaceous glands | Strong KLK7 positivity of the cortex of hair follicles and of the luminal area of sebaceous glands. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/lymphoid | Bone marrow | Negative. |
| Lymph node | Negative. | |
| Spleen | Negative. | |
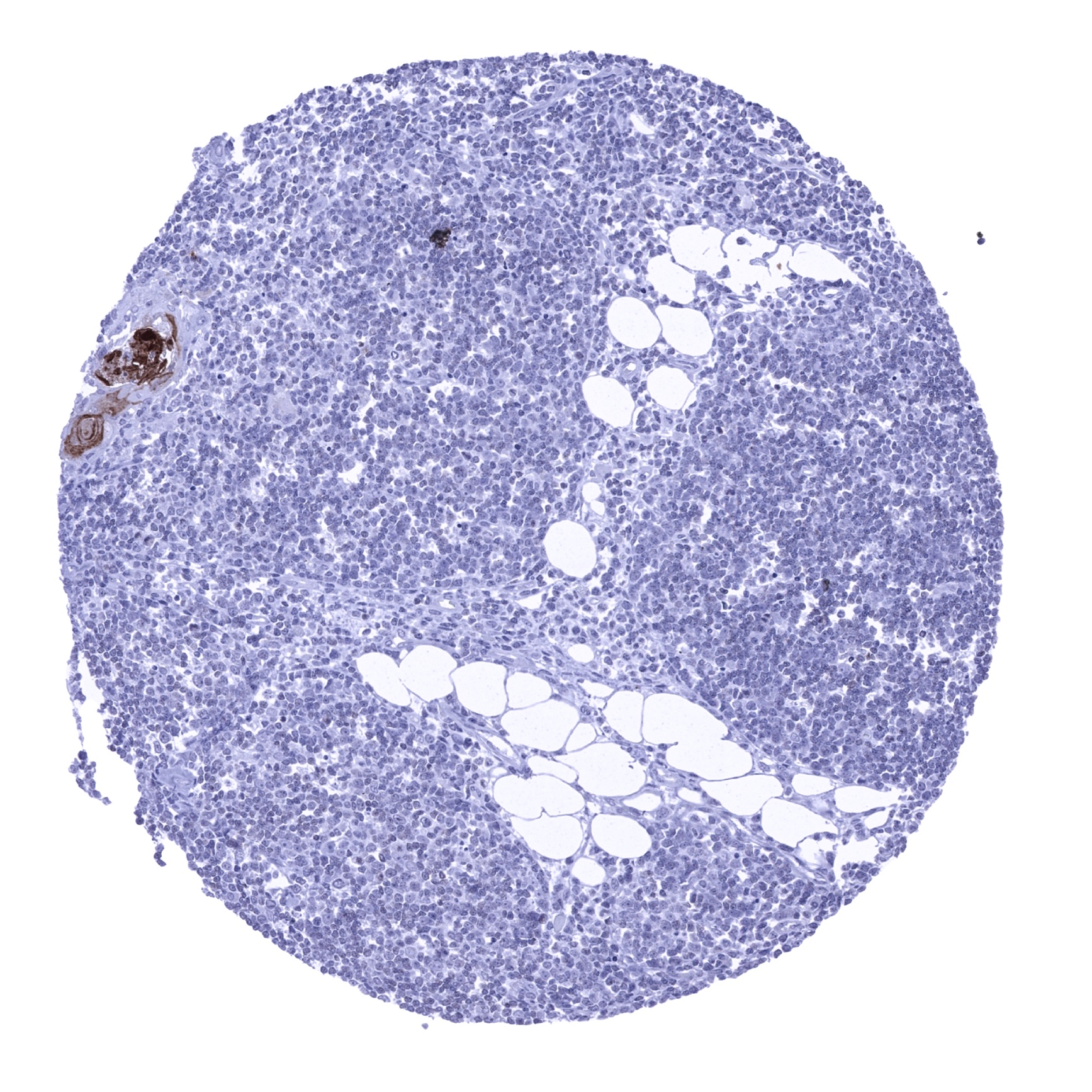
| Thymus | Strong KLK7 staining in keratinizing squamous epithelial cells of corpuscles of Hassall‘s. | |
| Tonsil | Moderate KLK7 staining in the top third of the squamous epithelium at the tonsil surface. | |
| Remarks |
The findings described above are this consistent with the RNA data described in the Human Protein Atlas (Tissue expression KLK7)
Positive control = Skin: A strong KLK7 staining should be seen in the stratum granulosum and possibly also in the keratinizing cell layers.
Negative control = Colon: KLK7 immunostaining should be absent in all cells of the colon mucosa.

Staining Pattern in Relevant Tumor Types
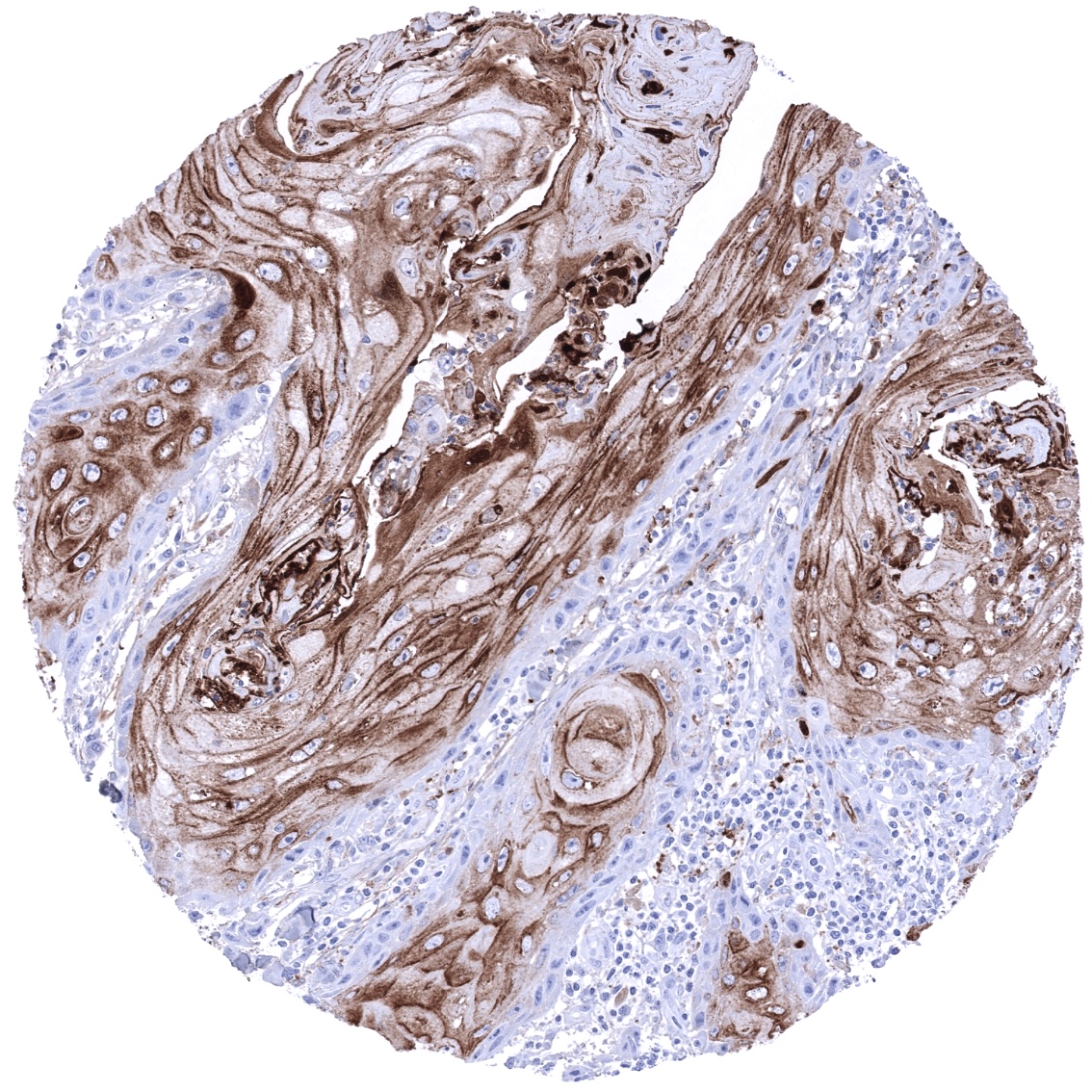
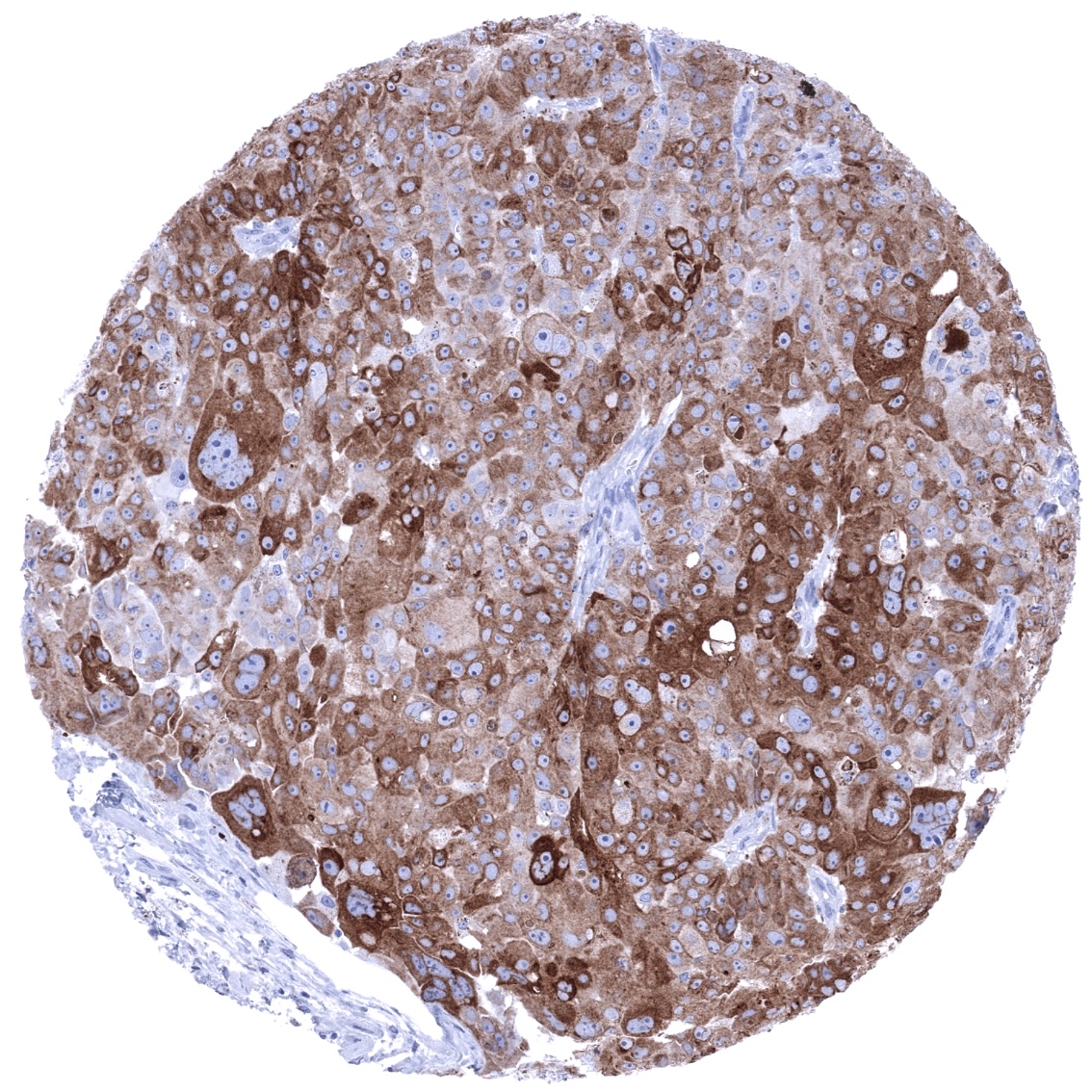
A positive KLK7 immunostaining has been reported in squamous cell carcinomas of various organs of origin, ovarian cancer and in other tumor entities as well. In several tumor entities, overexpression of KLK7 protein has been found to be linked with metastasis and unfavorable prognosis.
The TCGA findings on KLK7 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
KLK7 (MSVA-707M) publication summary
Relevant publication: Kind et al. “KLK7 expression in human tumors: a tissue microarray study on 13,447 tumors” Published in BMC Cancer. 2024 Jul 3;24(1):794. PMID: 38961454
A total of 12’345 tumors were successfully analyzed from 147 different tumor categories by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. MSVA-707M at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
While 64 of 147 tumor categories contained at least one case with weak KLK7 expression there were only 17 tumor categories including at least one case with strong KLK7 positivity. The KLK7 positivity rate was highest in squamous cell carcinomas from various sites (positive in 18.1%-63.8%), various categories of ovarian and endometrium cancers (4.8%-56.2%), salivary gland tumors (4.8%-13.7%), bilio-pancreatic adenocarcinomas (20.0%-40.4%), and in adenocarcinomas of the upper gastrointestinal tract (3.3%-12.5%). Twenty other tumor entities showed KLK7 positivity – usually weak – in less than 9%. In tumor entities originating from KLK7 negative normal cells, KLK7 neo-expression was often linked to unfavorable histologic phenotype. In squamous cell carcinomas – originating from KLK7 positive normal cells – a loss of KLK 7 positivity was associated with high grade of malignancy (p<0,0001). The distribution of positive KLK7 staining results is shown in “organ-systematic” and in “ranking order” figures below (images based on data from Kind et al).
Authors conclusions on diagnostic utility with respect to the distinction of benign versus malignant (Kind et al):
- not applicable
Authors conclusions on diagnostic utility of KLK7 IHC with respect to the distinction of different tumor entities (Kind et al):
- not applicable
Authors conclusions on the prognostic role of KLK7 IHC (Kind et al):
- Detectable KLK7 expression was associated with nodal metastasis (p=0,005), L1 status (p<0,0001), and V1 status (p<0,005) in colorectal cancer.
- Detectable KLK7 expression was associated with advanced pT stage in papillary thyroid cancer (p<0,05).
- Loss of KLK7 expression was associated with poor grade in squamous cell carcinomas (p<0,0001).
Data from the publication: Kind et al. “KLK7 expression in human tumors: a tissue microarray study on 13,447 tumors” Published in BMC Cancer. 2024 Jul 3;24(1):794. PMID: 38961454
Summarized in own graphics:
Figure1. KLK7 staining in tumors (“organ-specific ; according to Kind et al.”) with antibody MSVA-707M

Figure 2. KLK7 staining in tumors (“ranking-order ; according to Kind et al.”) by positivity with antibody MSVA-707M

Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
-Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-707M at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- Immunohistochemical studies on KLK7 expression have been limited so far. The prognostic and diagnostic role of KLK7 expression analysis needs to be further evaluated.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody MSVA-707M specificity is suggested by the strong concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression KLK7). RNA expression predominates in organs covered by squamous epithelium (esophagus, vagina, cervix, skin) where a significant staining is observed by MSVA-707M. In addition, low level RNA expression in salivary glands, kidney, and fallopian tube is – in principle – consistent with focal MSVA-707M immunostaining observed in these organs. Low level RNA expression in the gallbladder and the breast is, however, not necessarily explicable by MSVA-707M staining data as these organs were completely negative by IHC. Given the limitation of KLK7 positivity to only few cells in salivary glands, it is possible that few KLK7 expressing cells in gallbladder glands and breast glands were not identified due to a sampling error.
Comparison of antibodies: True expression of KLK7 in squamous epithelium and in salivary glands is further corroborated by comparison with a commercially available independent second antibody (termed “validation antibody”). Because the validation antibody did not confirm MSVA-707M findings in kidney and fallopian tube, these focal findings are considered possible cross-reactivities (tolerable) of MSVA-707M in spite of positive RNA findings in these organs. Independence of the two antibodies used for validation is documented by cytoplasmic smooth muscle staining and nuclear staining in several organs (often predominating on nuclear membranes) which was only seen by the validation antibody but not by MSVA-707M.
Antibody Comparison: MSVA-707M vs another commercially available KLK7 antibody called “Validation Antibody”