295,00 € – 995,00 €
Product details
Synonyms = SRY-box 2 , ANOP3 , MCOPS3
Antibody type = Mouse monoclonal
Clone = HMV338
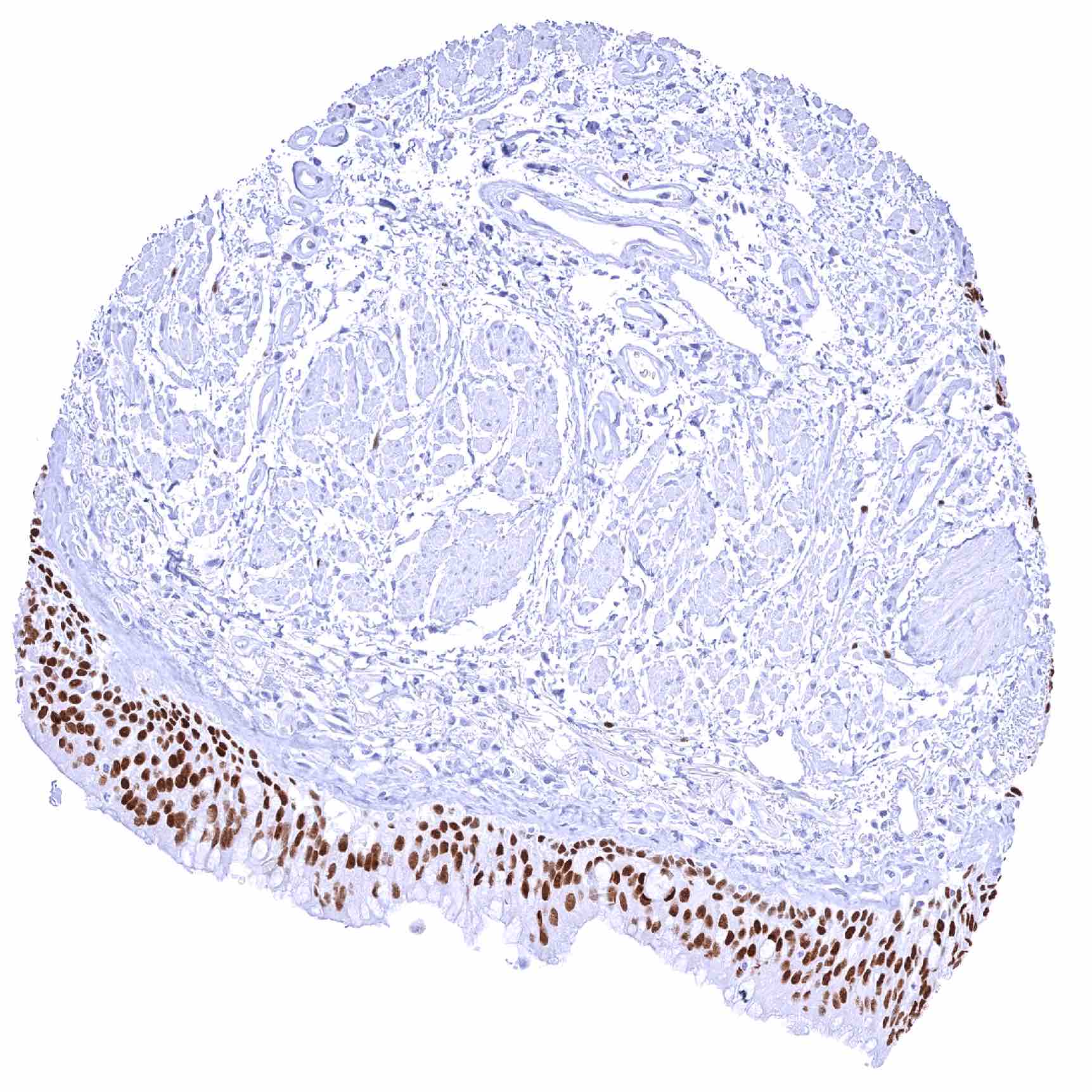
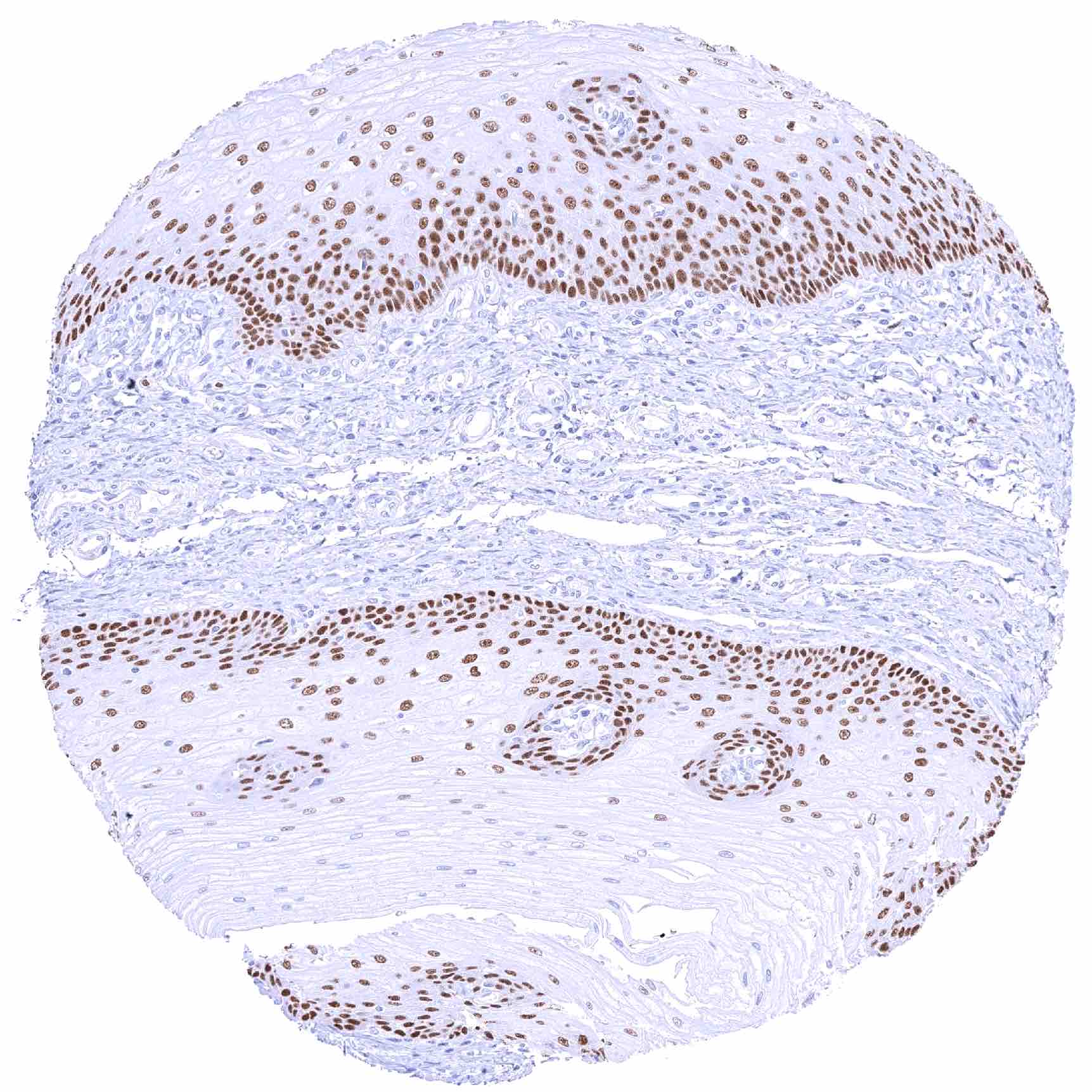
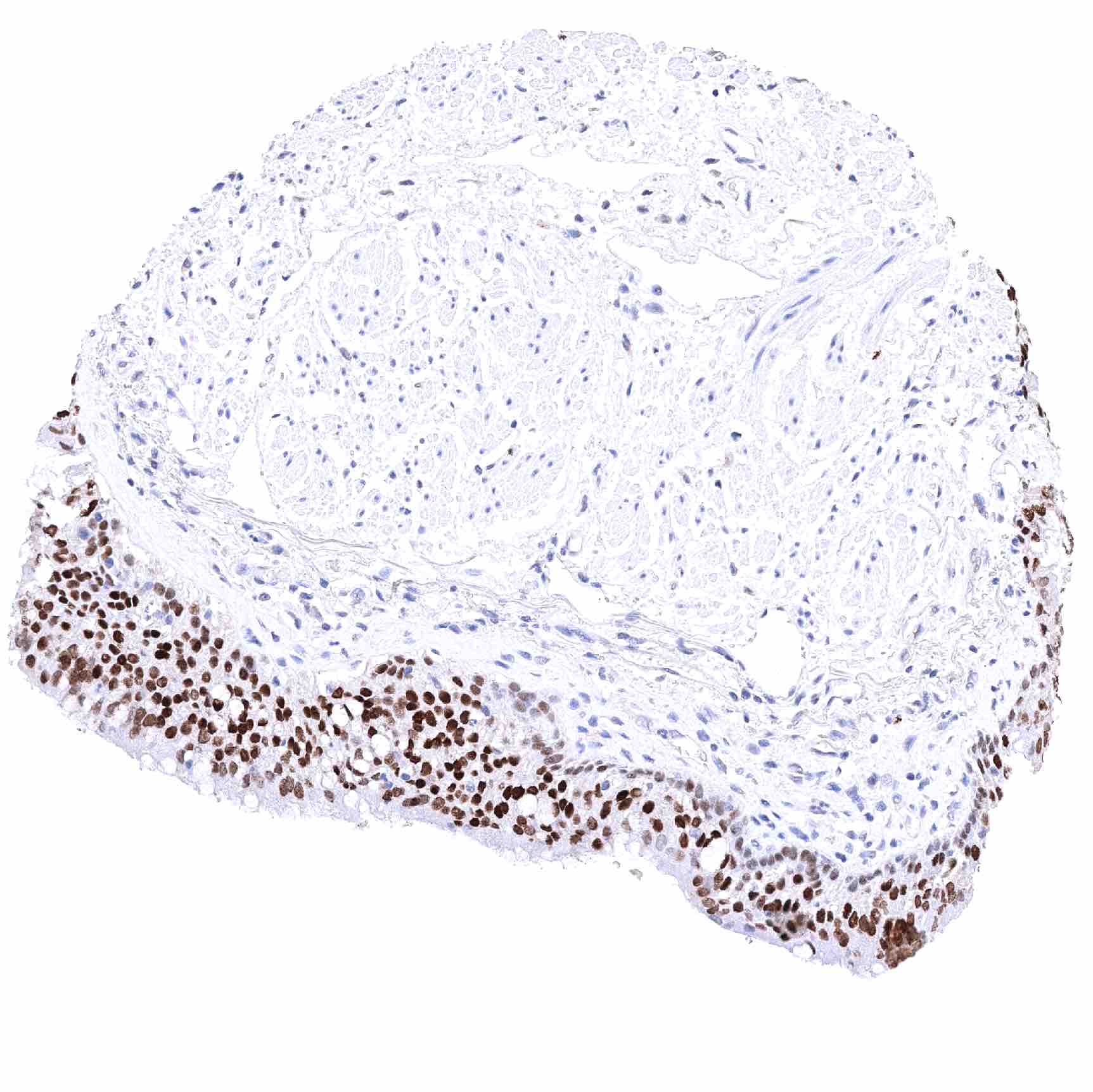
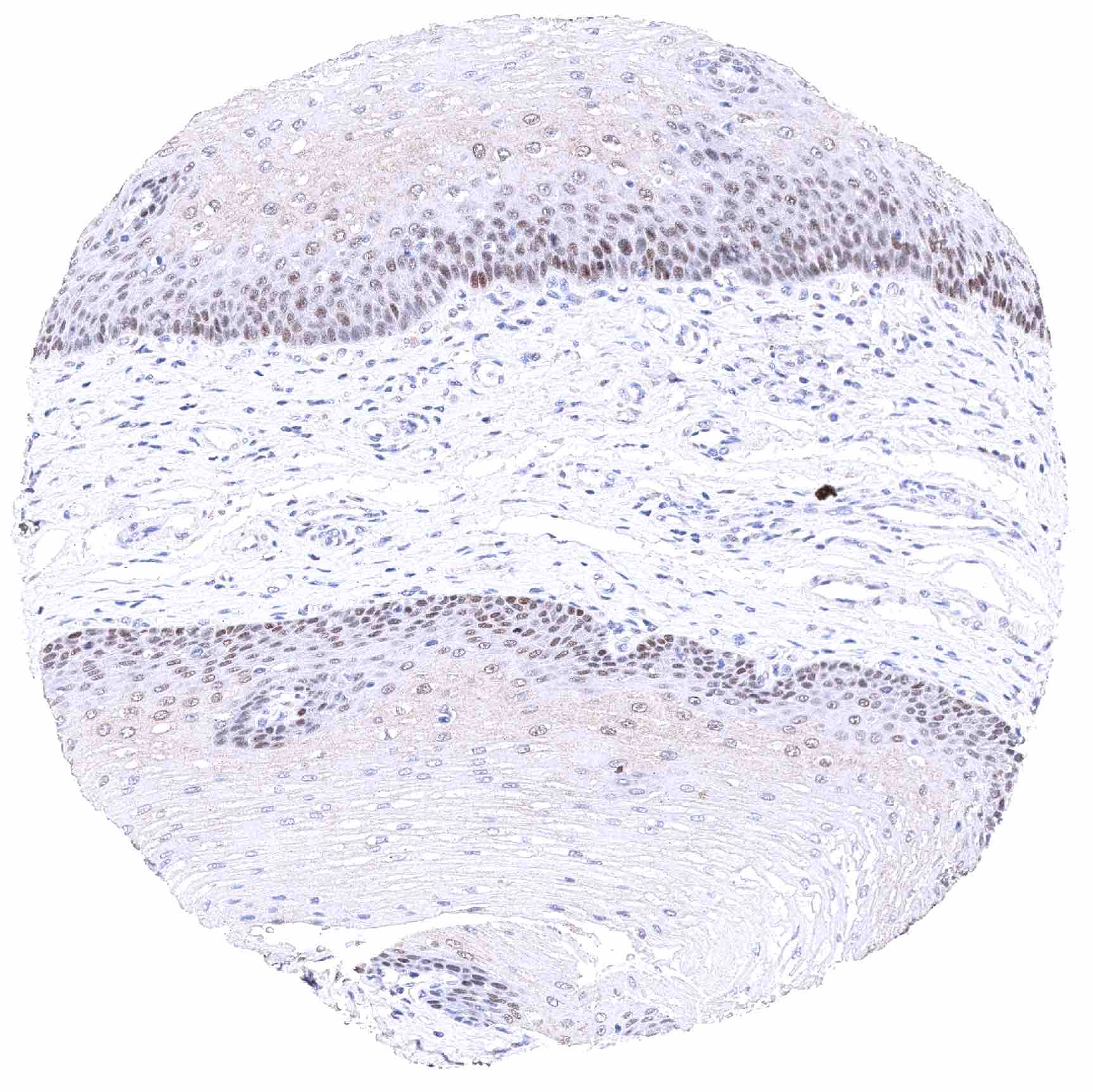
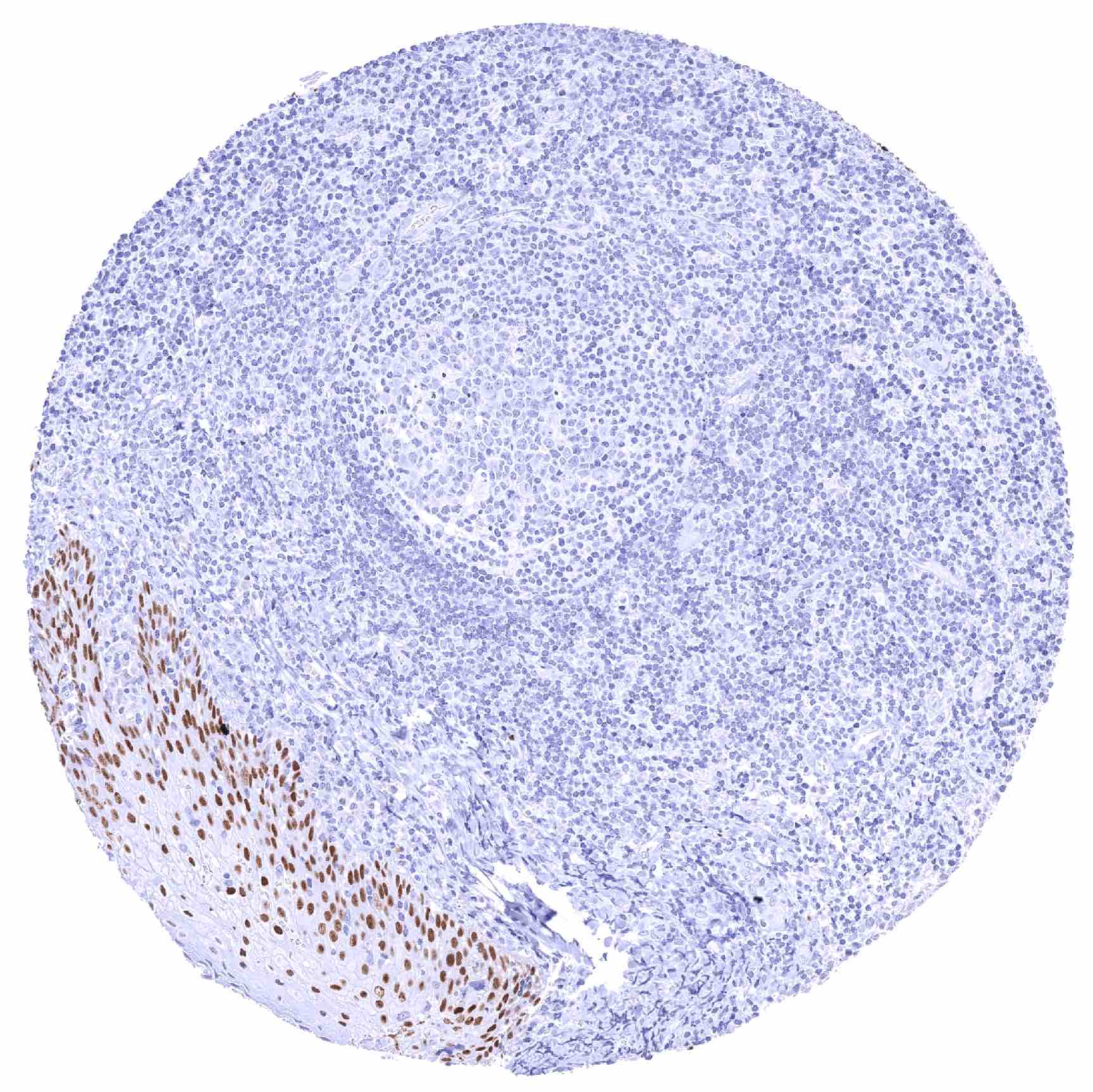
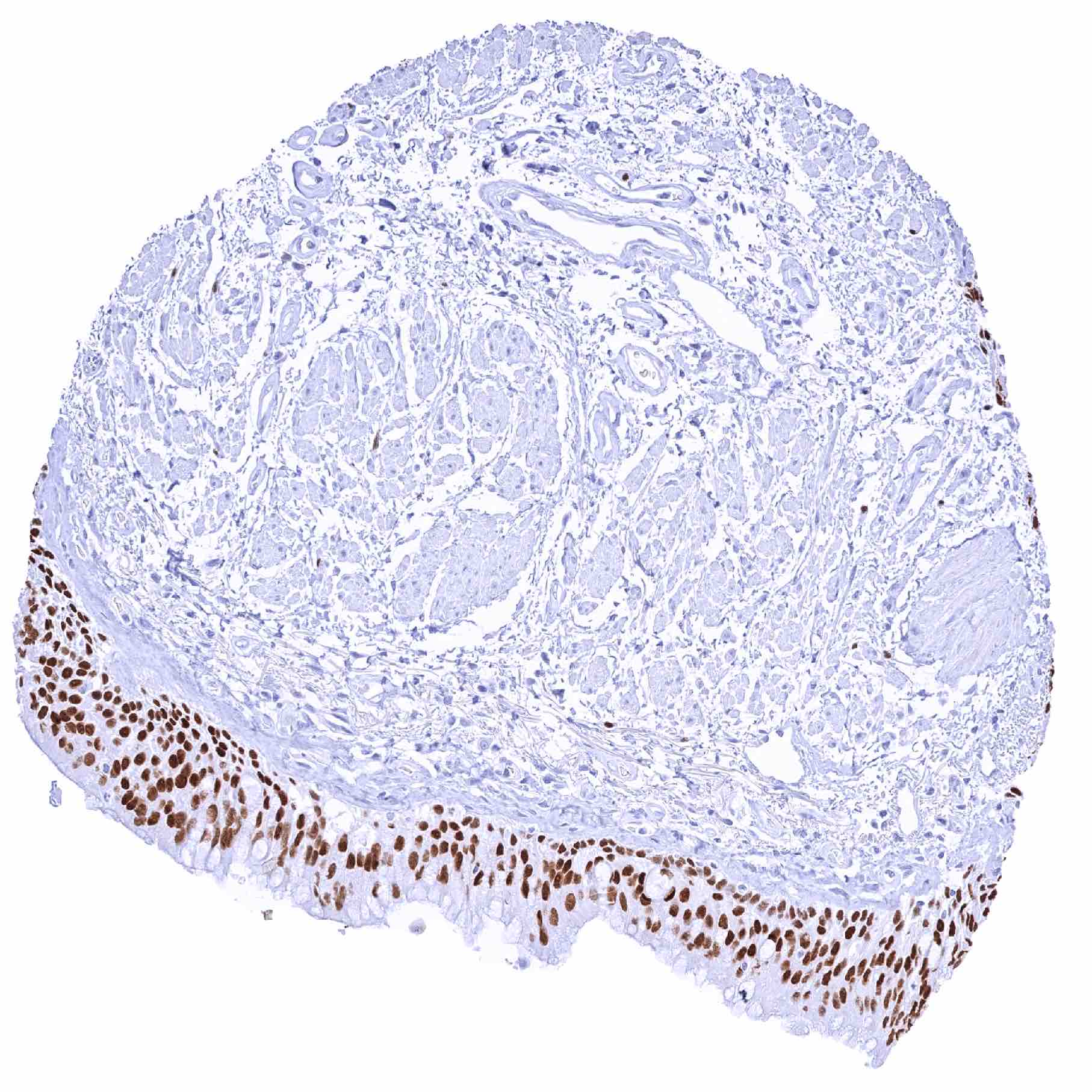
Positive control = Tonsil: A moderate to strong SOX2 staining should be seen in the bottom 2/3 of squamous epithelial cells.
Negative control = Tonsil: SOX2 staining should be absent in lymphocytes and in other immune cells.
Cellular localization = Nuclear
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
SOX2 is a pivotal protein for stemness and tissue development.
Biology Behind
SOX2, also known as SRY (sex determining region Y)-box 2, is a member of the SOX family of transcription factors coded by the SOX2 gene located on chromosome 3q26.3-27. SOX2 is essential for maintaining the cell’s capability for self-renewal and therefore has a critical role in maintenance of embryonic and neural stem cells. Forced re-expression of SOX2 together with Oct4, c-Myc, and Klf4 is sufficient to reprogram differentiated cells into pluripotent stem cells. SOX2 is also critical for normal embryonal development. It is expressed already at a two cell stage of murine embryo formation. SOX2-deficient embryos die straight after implantation. Inactivating mutations of SOX2 occur in patients with bilateral anophthalmia, a severe structural eye deformity. Dysregulation of SOX2 also plays a role in the pathogenesis of cancer. SOX2 expression has been linked to cancer stem cell formation, epithelial-mesenchymal transition, migration, invasion, increased cell proliferation, resistance to apoptosis and therapy, colony formation, and metastasis in various cancer types.
Staining Pattern in Normal Tissues
Images describing the SOX2 staining pattern in normal tissues obtained by the antibody HMV338 are shown in our “Normal Tissue Gallery”.
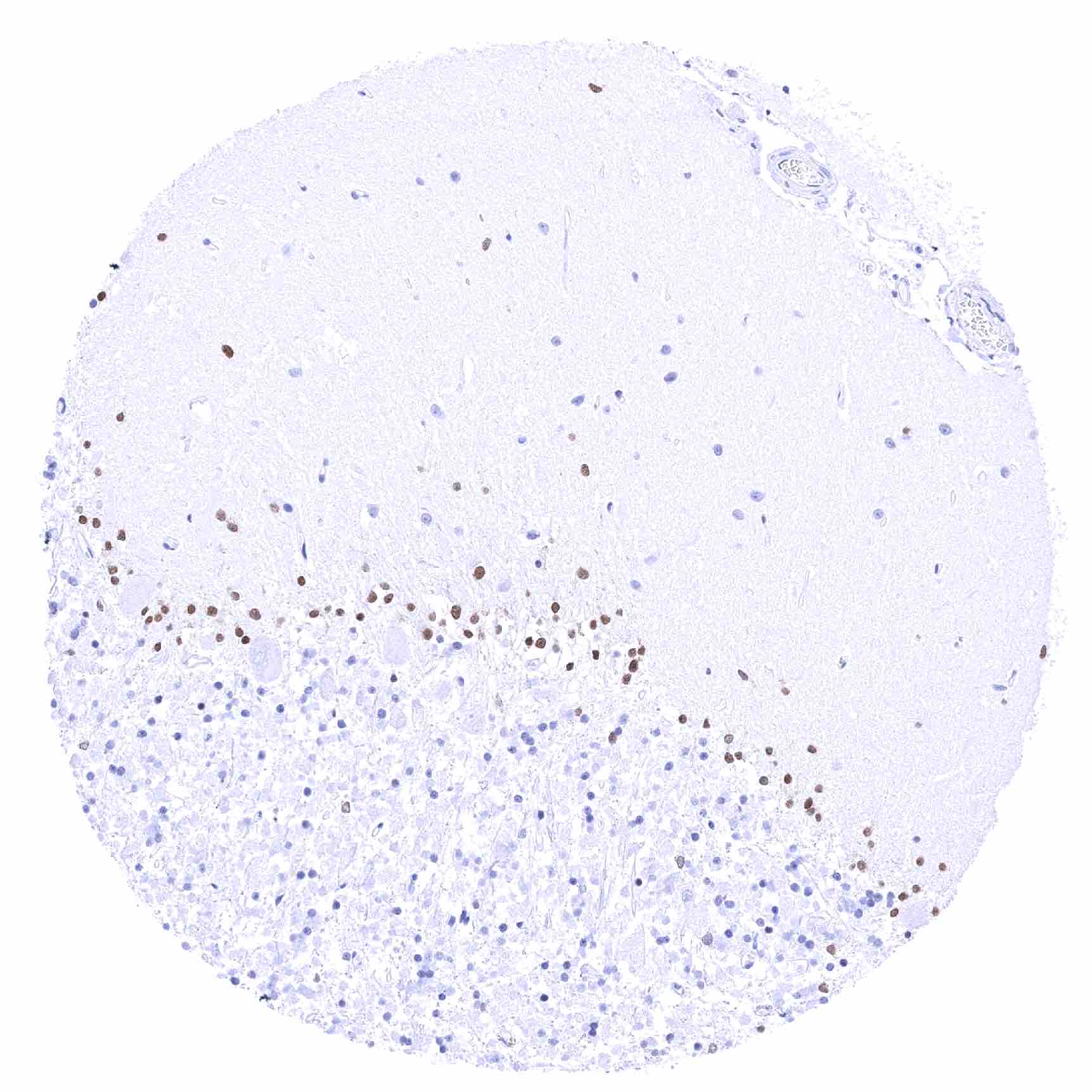
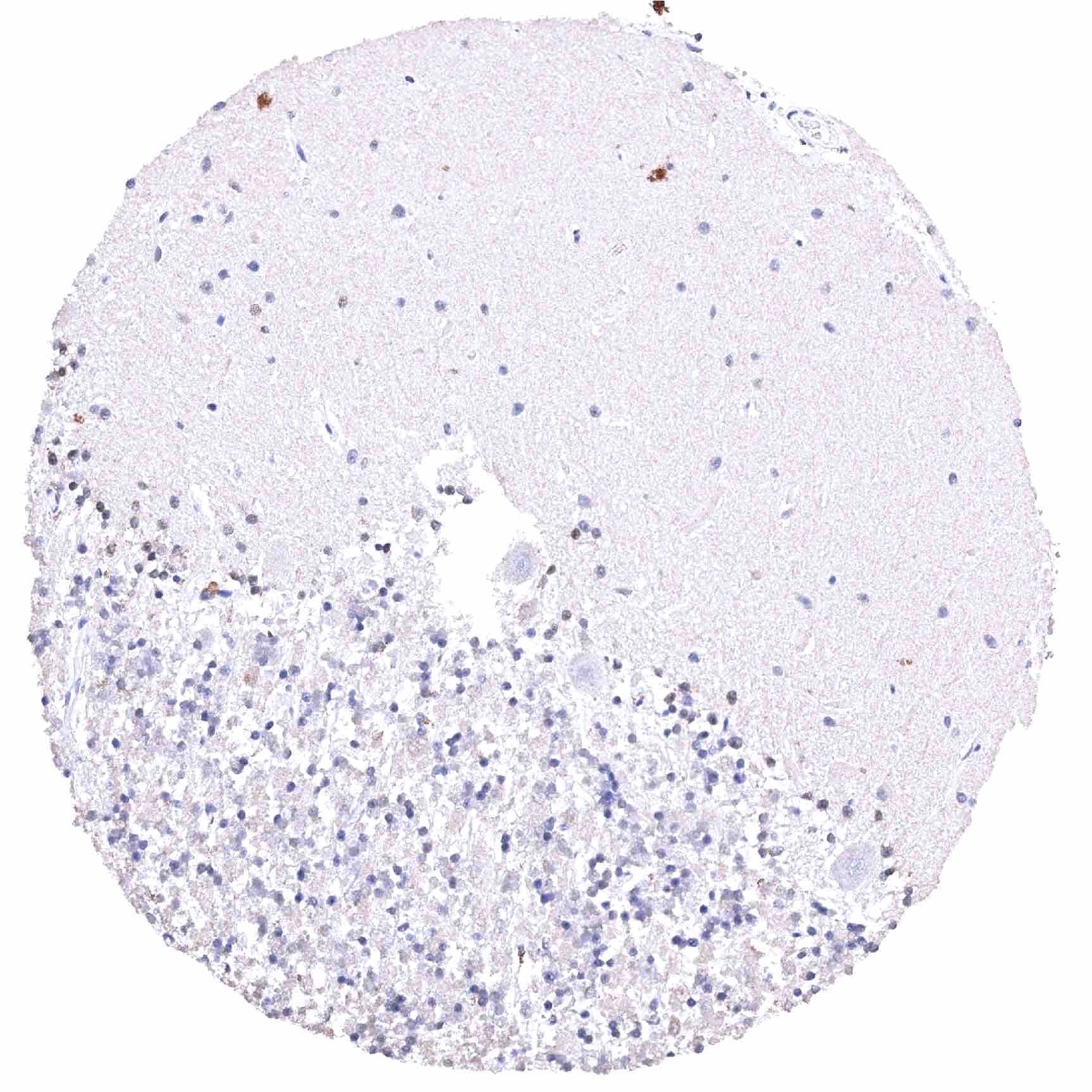
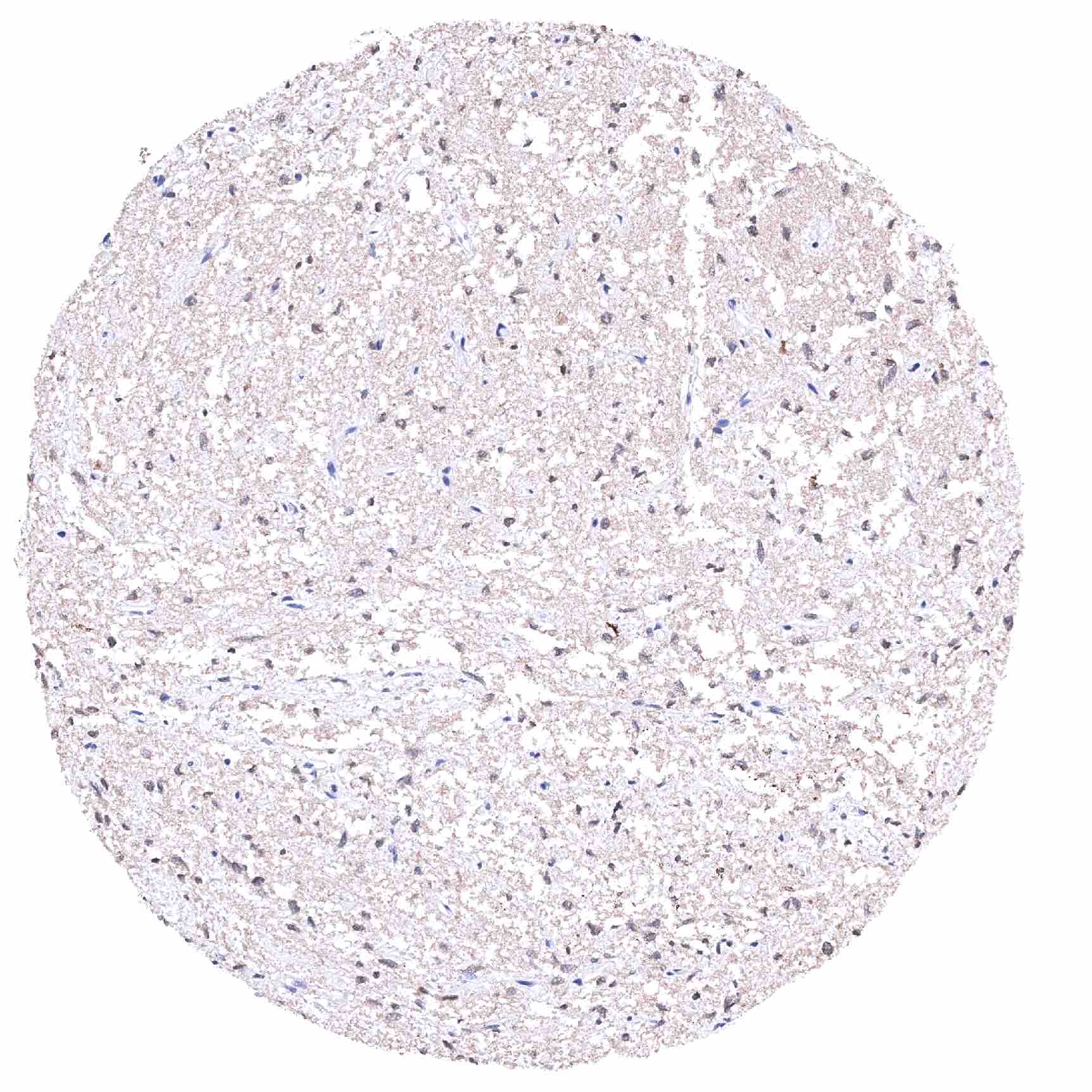
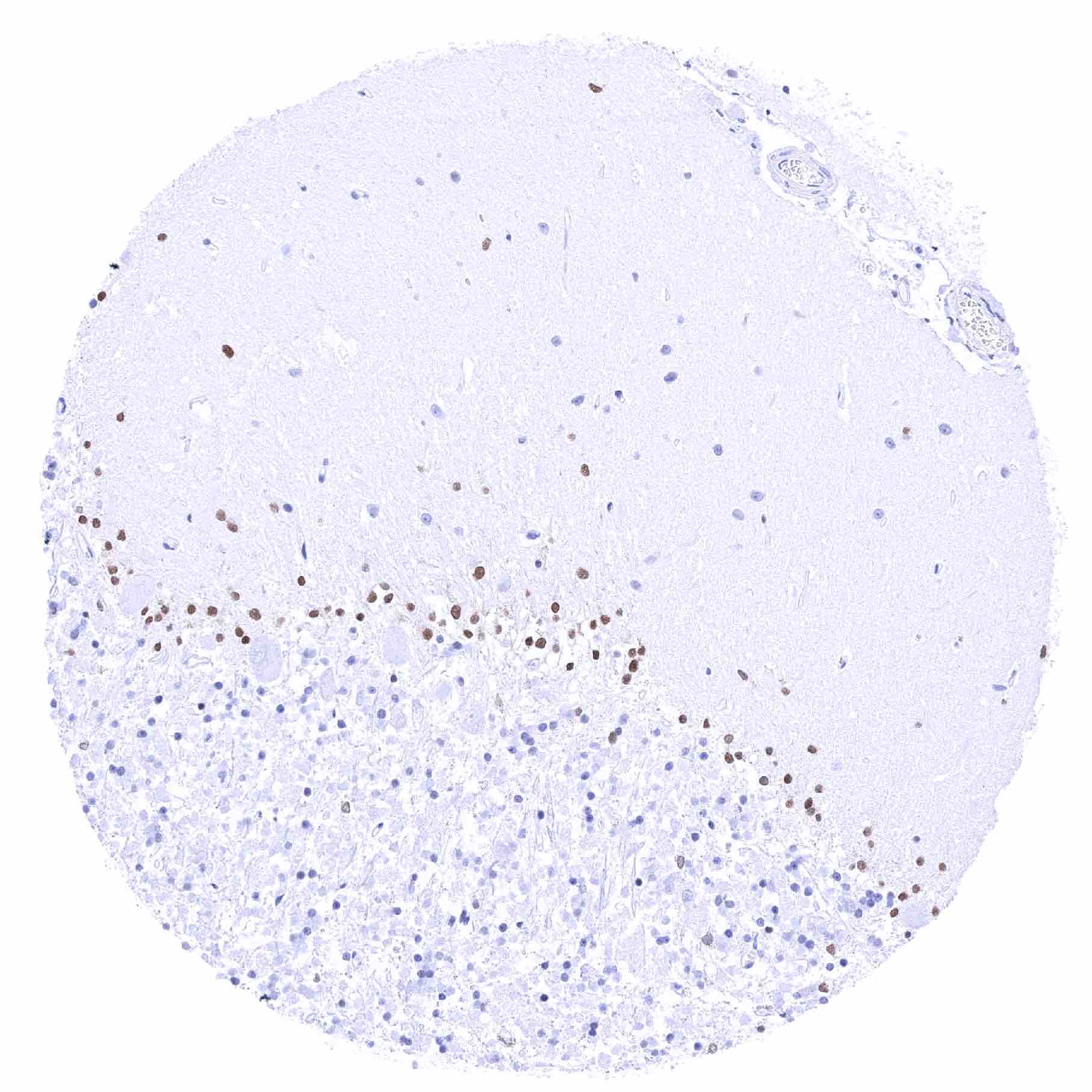
| Brain | Cerebrum | Moderate to strong SOX2 positivity of a fraction of glial cells. |
| Cerebellum | Moderate to strong SOX2 positivity of a fraction of glial cells. | |
| Endocrine Tissues | Thyroid | Negative. |
| Parathyroid | Negative. | |
| Adrenal gland | Negative. | |
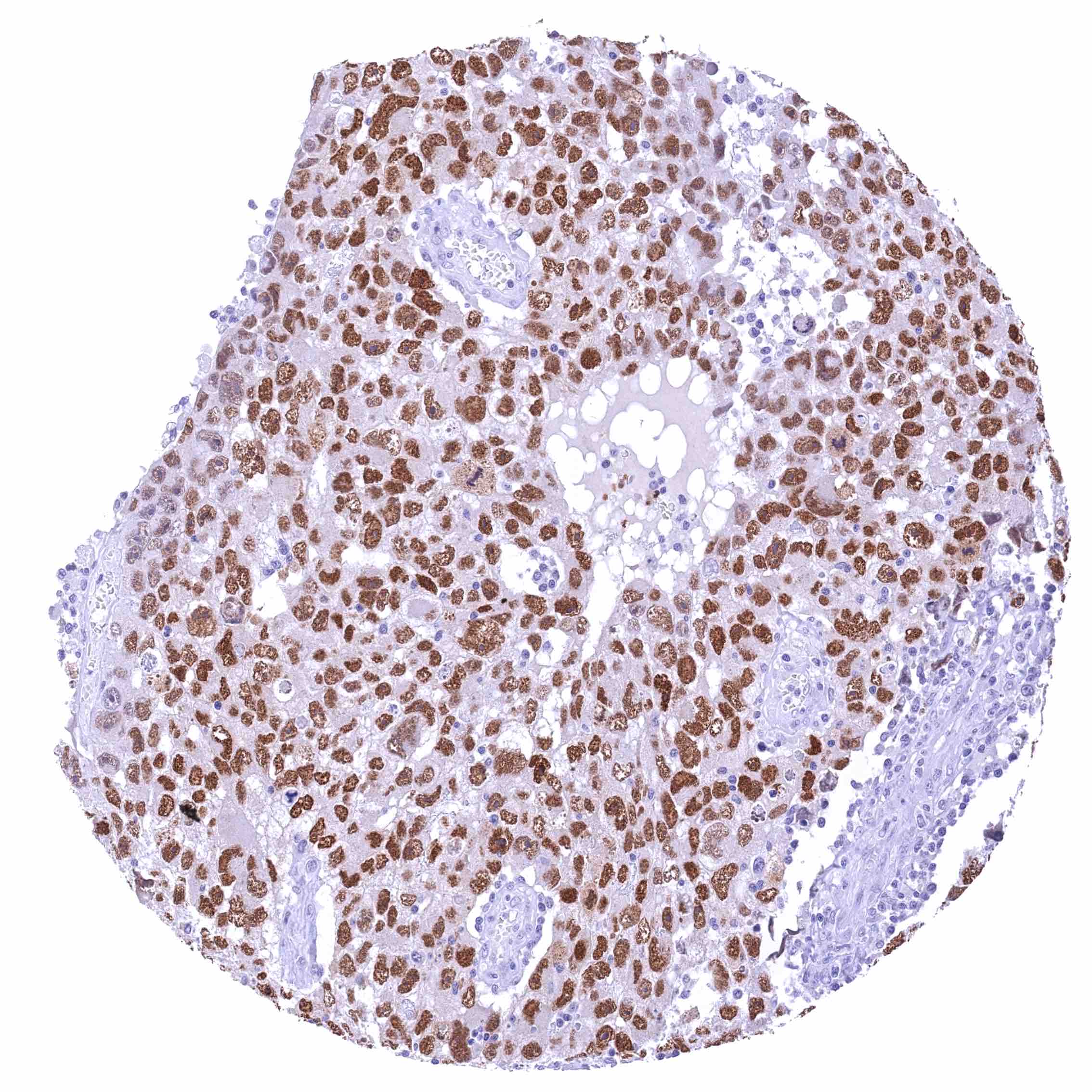
| Pituitary gland | Weak to strong SOX2 positivity of most pituicytes and of a fraction of glandular cells. | |
| Respiratory system | Respiratory epithelium | Strong SOX2 positivity of respiratory epithelial cells. Weak to moderate SOX2 positivity of bronchial glands. |
| Lung | Negative. | |
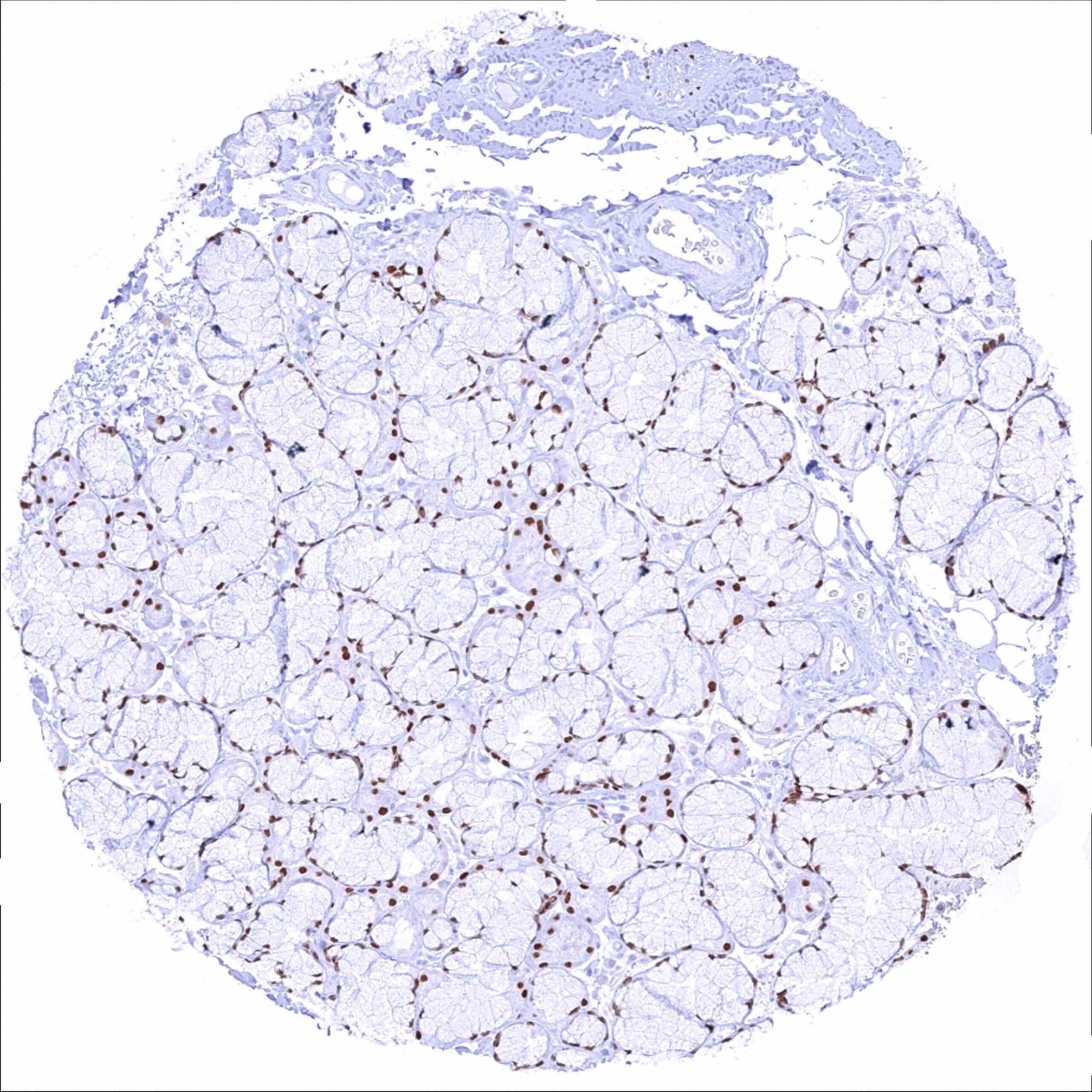
| Gastrointestinal Tract | Salivary glands | Weak to moderate SOX2 positivity in a fraction of glandular and excretory duct cells. |
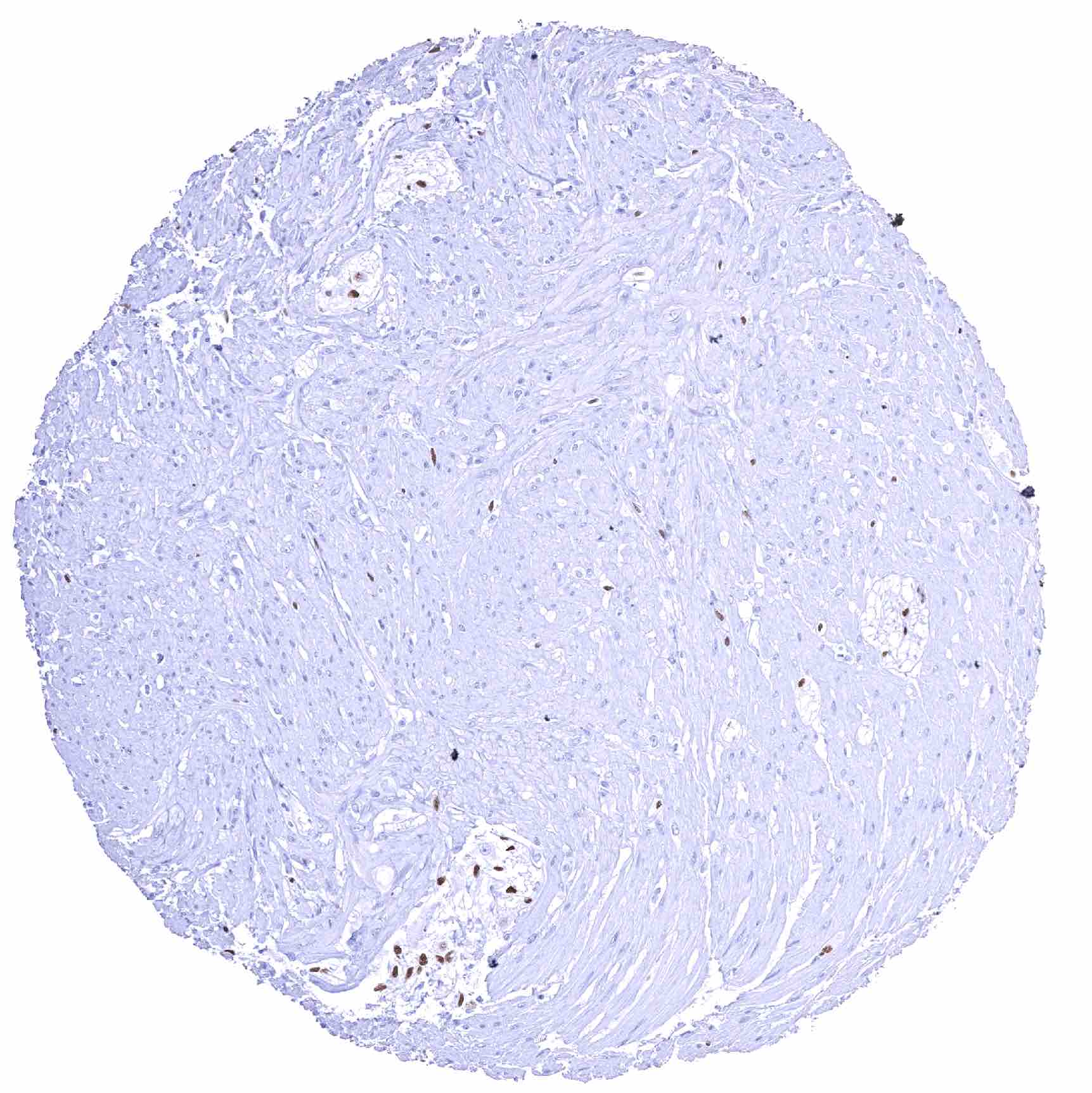
| Esophagus | Strong SOX2 positivity of a large fraction of ganglion cells of the muscular wall. | |
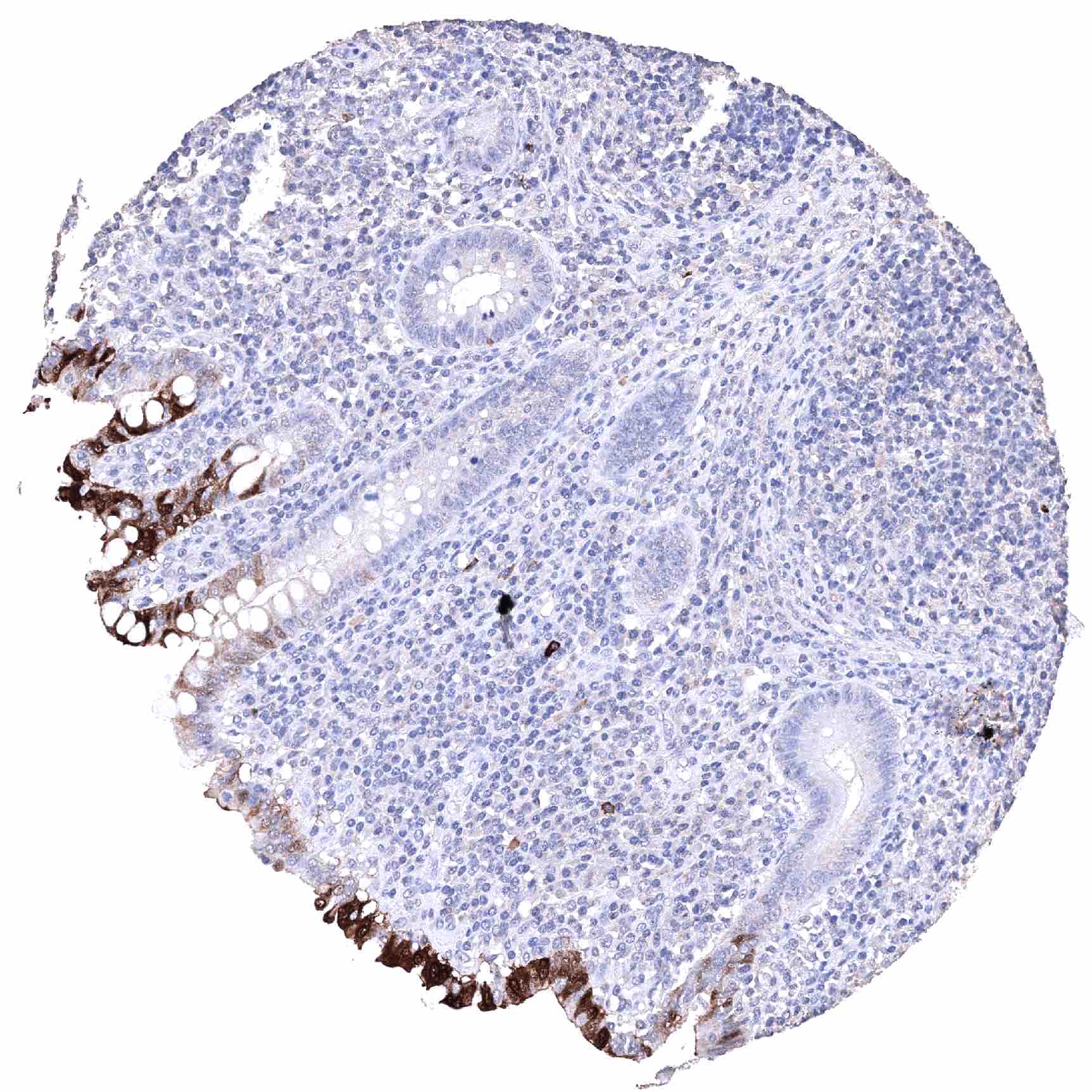
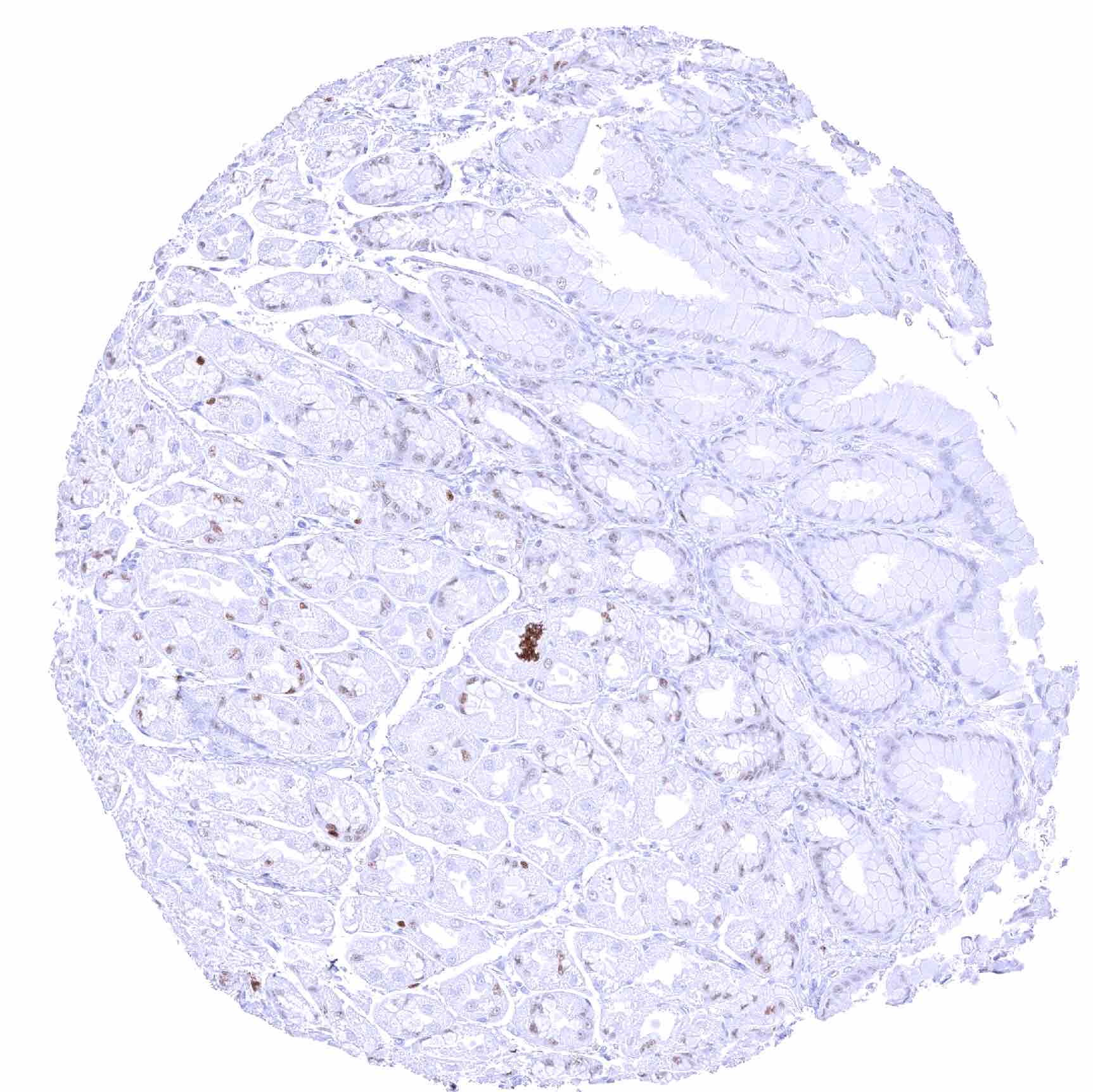
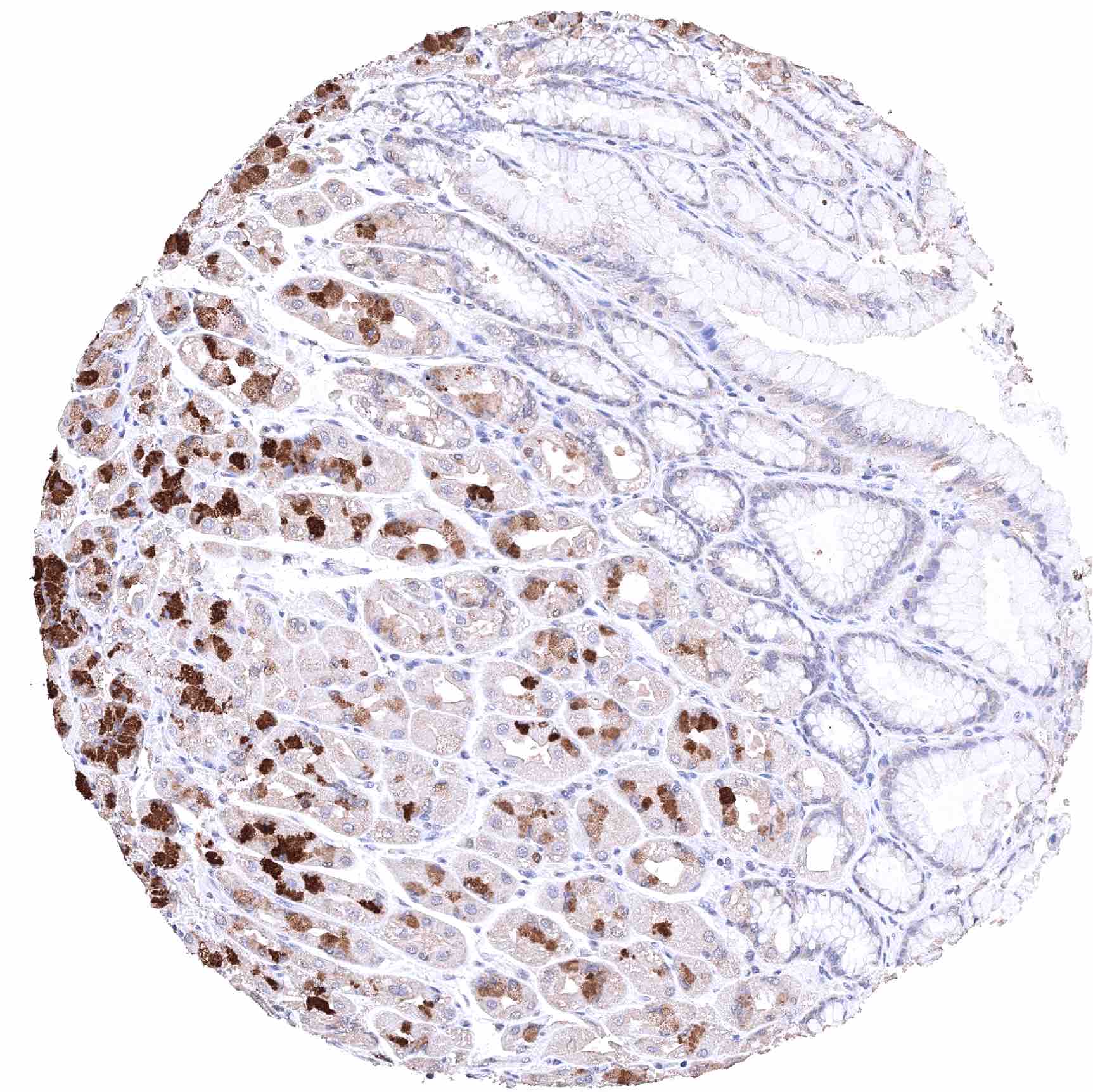
| Stomach | Significant SOX2 staining of a fraction of glandular cells. Strong SOX2 positivity of few spindle shaped (neural?) cells in the muscular wall. | |
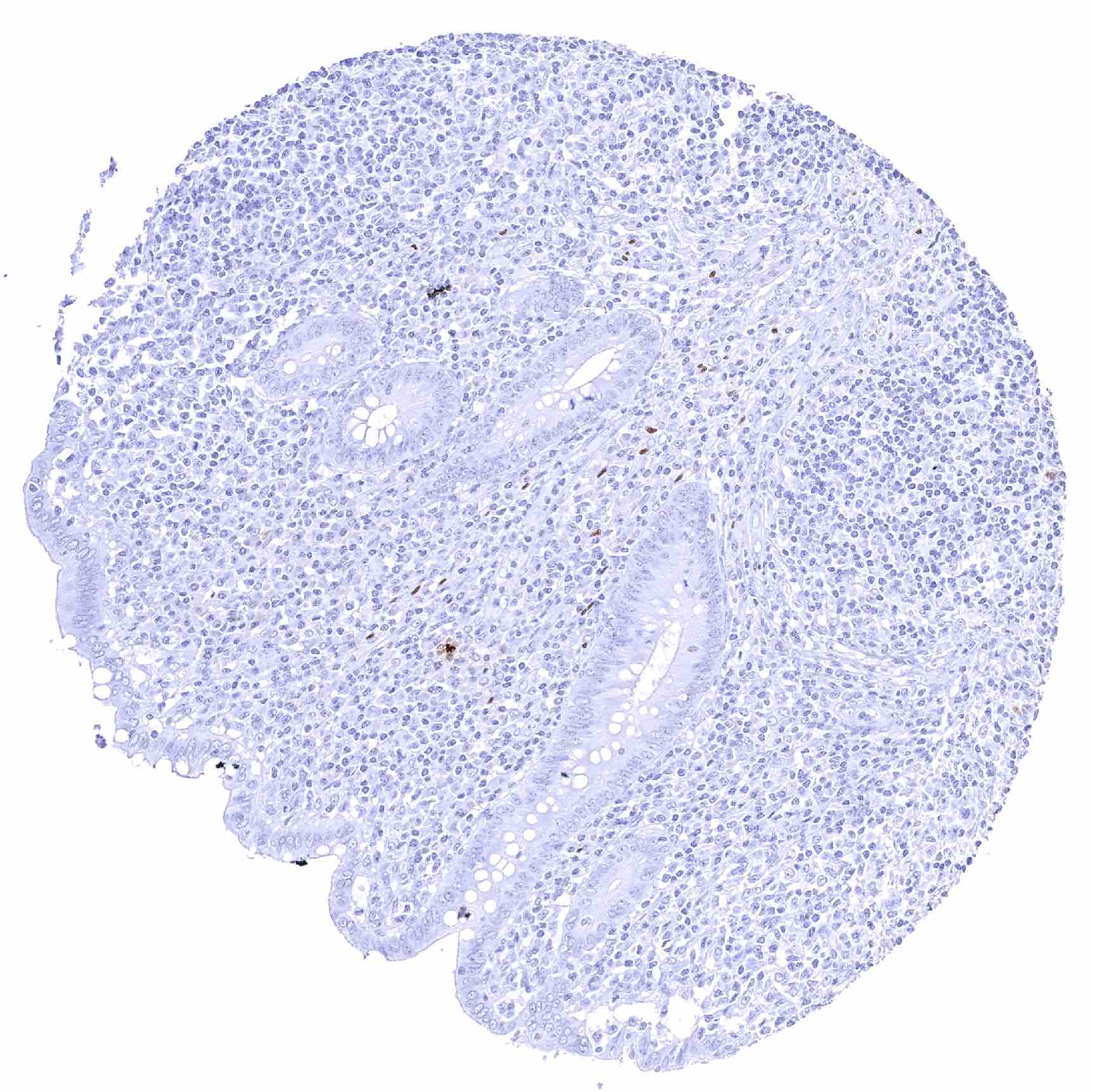
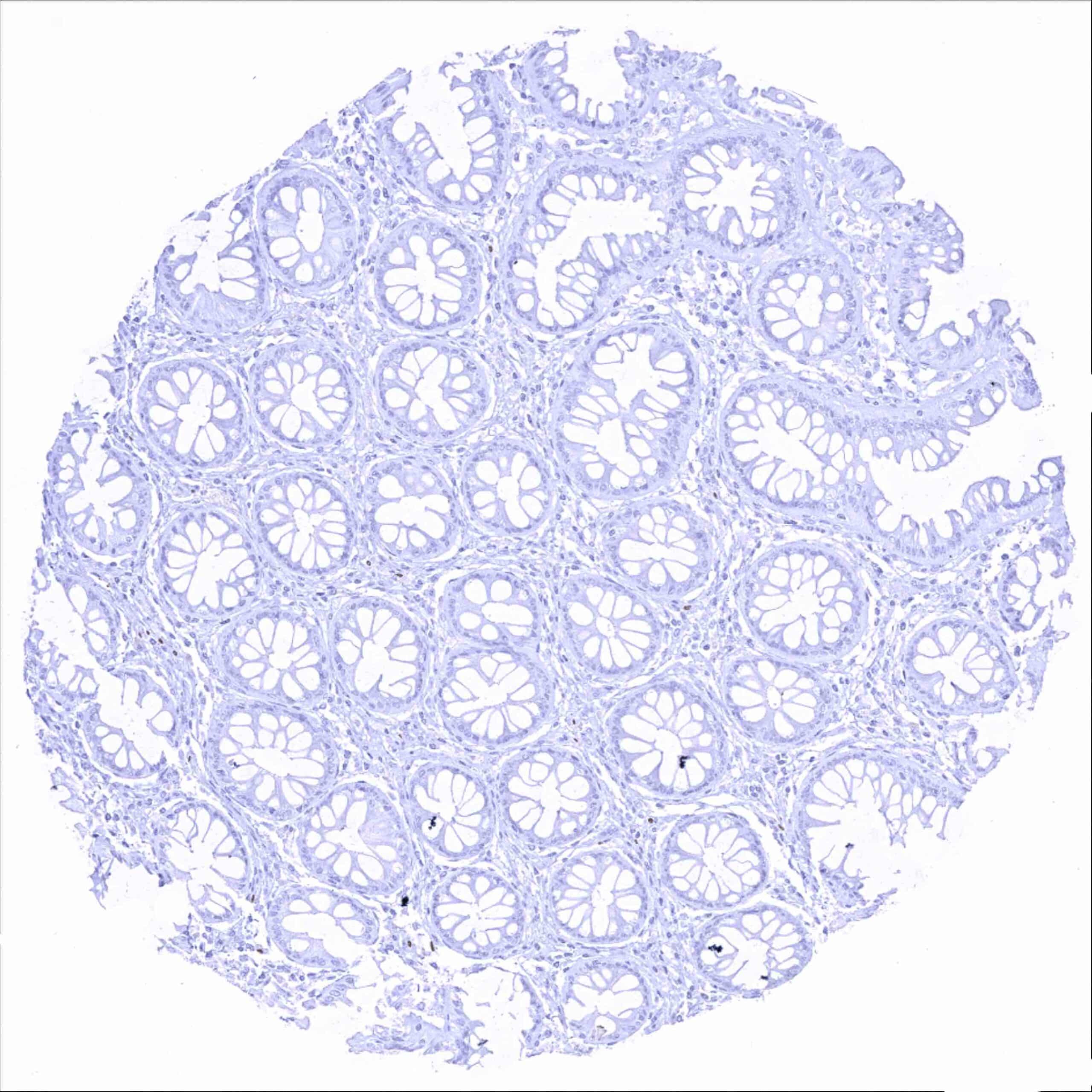
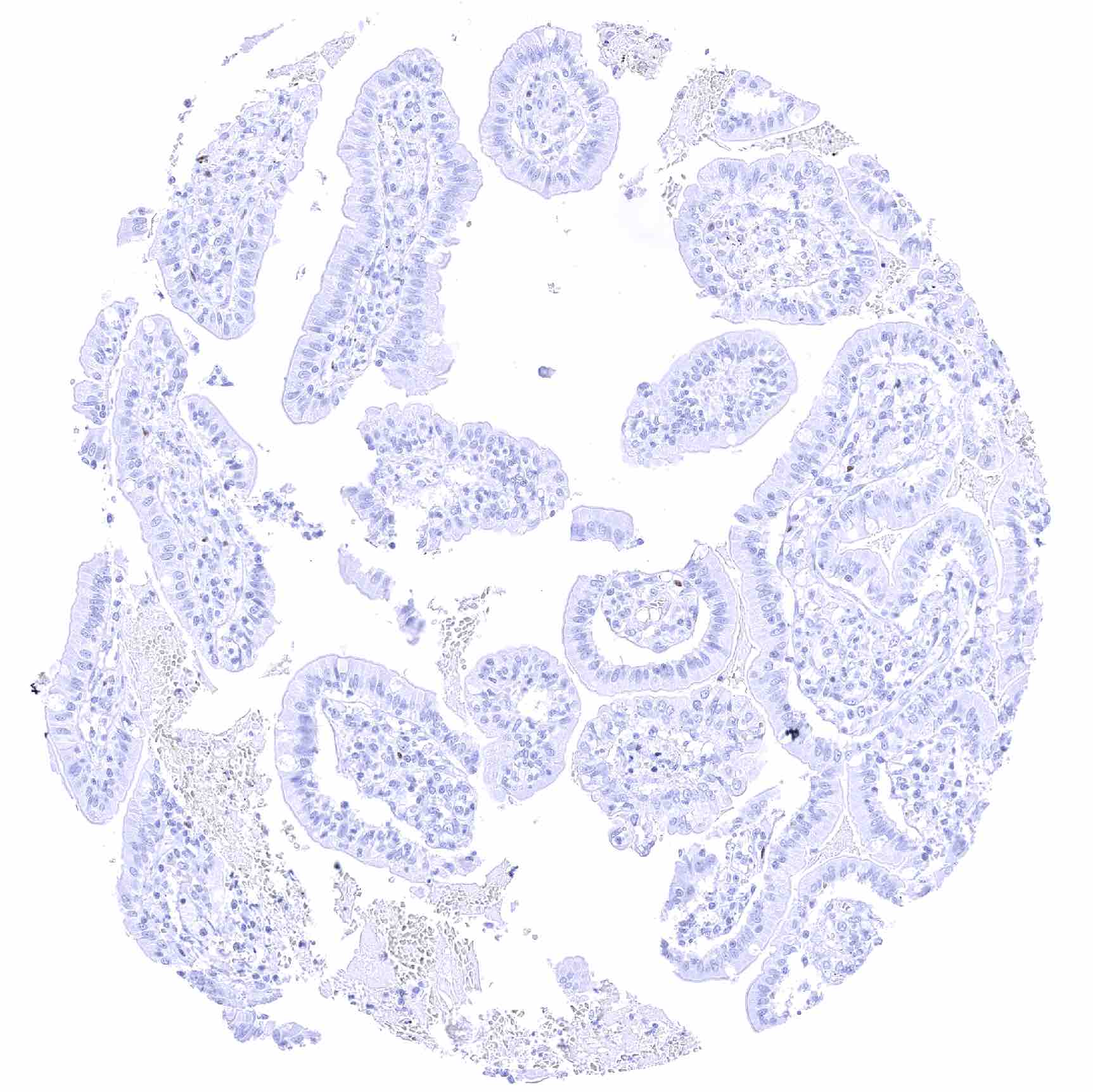
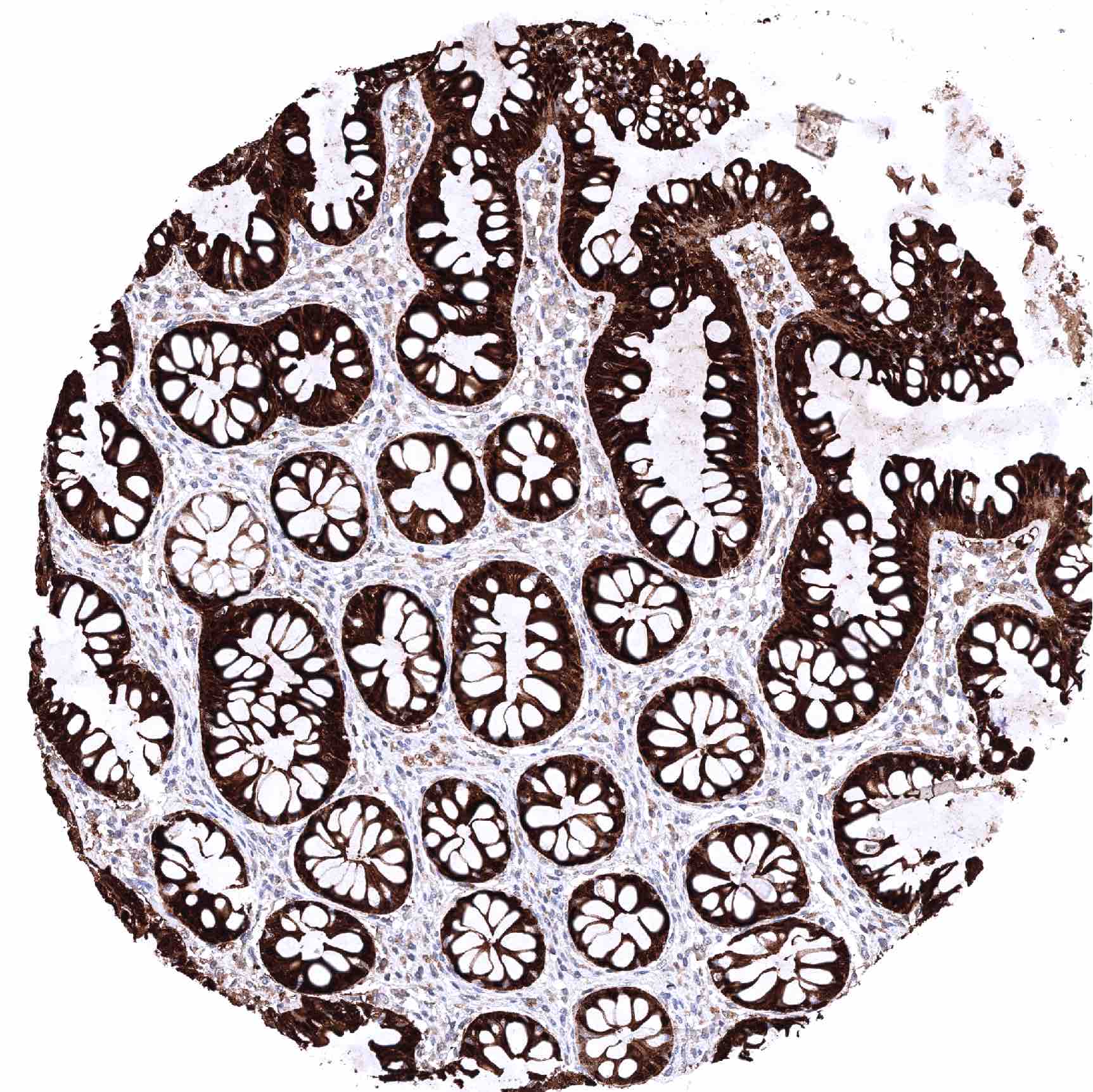
| Duodenum | Epithelial cells are SOX2 negative. | |
| Small intestine | Epithelial cells are SOX2 negative. | |
| Appendix | Strong SOX2 positivity of a large fraction of ganglion cells as well as of few spindle shaped (neural?) cells in the muscular wall. | |
| Colon | Strong SOX2 positivity of a large fraction of ganglion cells as well as of few spindle shaped (neural?) cells in the muscular wall. | |
| Rectum | Epithelial cells are SOX2 negative. | |
| Liver | Negative. | |
| Gallbladder | Negative. | |
| Pancreas | Negative. | |
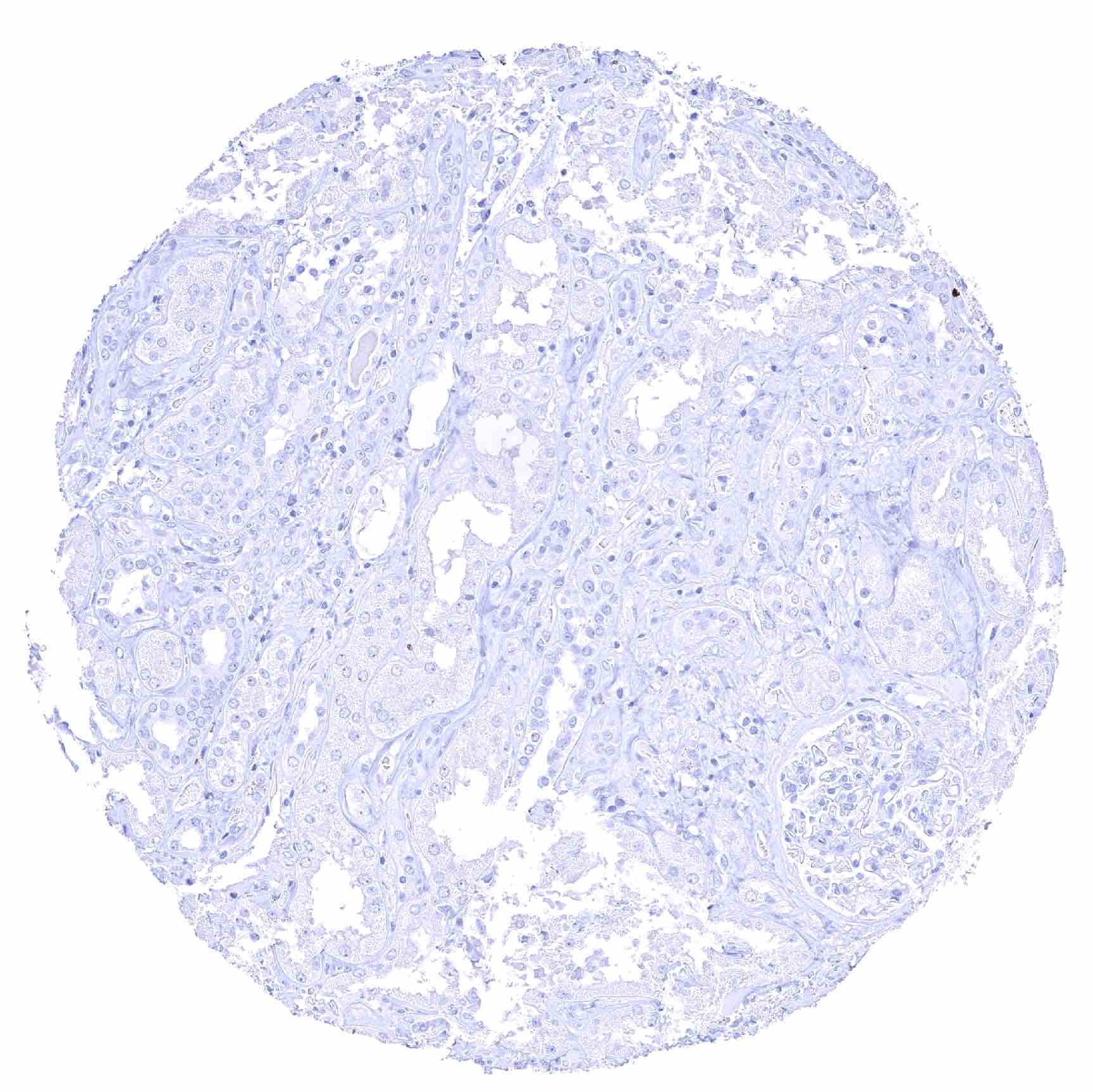
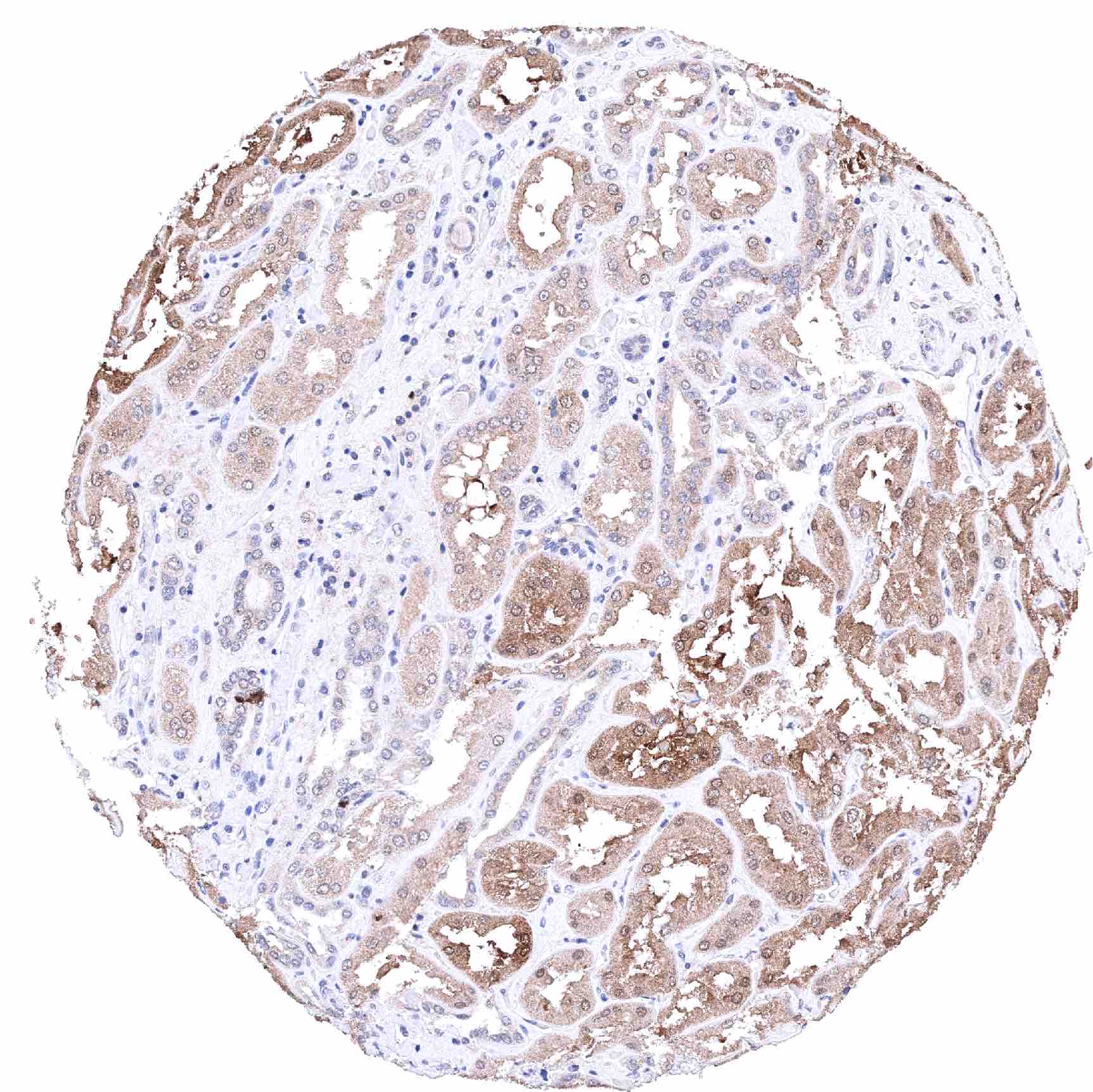
| Genitourinary | Kidney | Negative. |
| Urothelium | Negative. | |
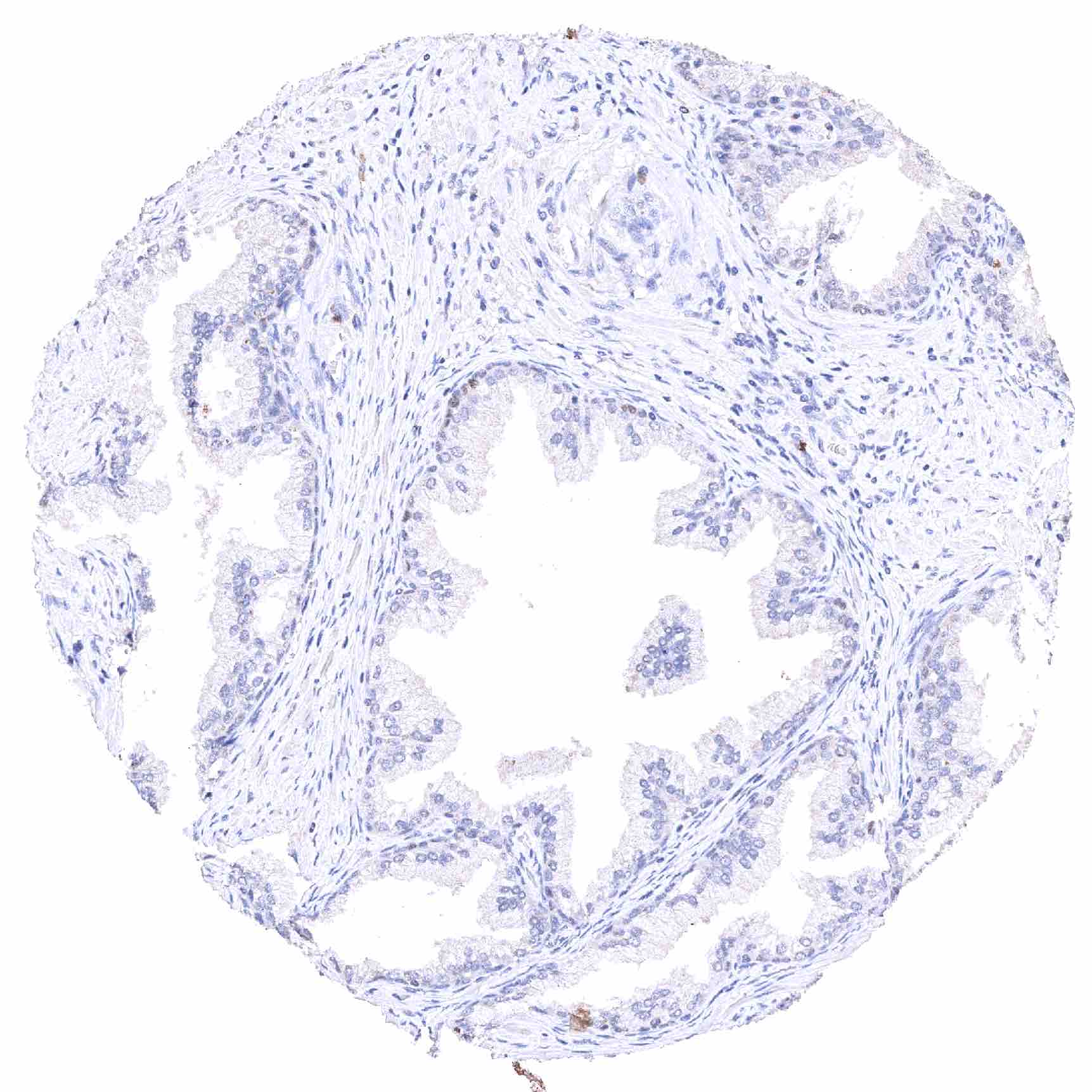
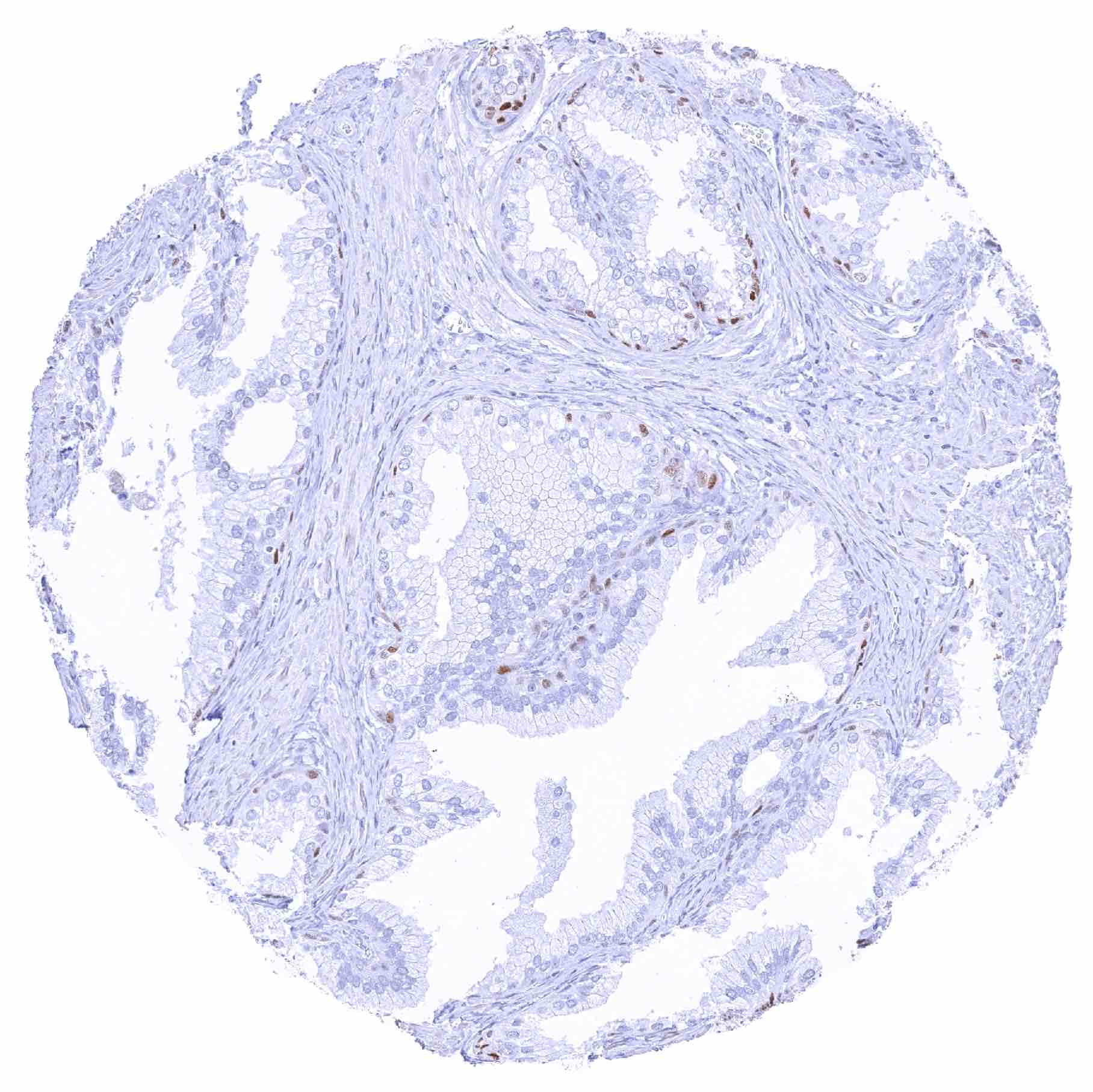
| Male genital | Prostate | Strong SOX2 positivity of a fraction of basal cells. |
| Seminal vesicles | Negative. | |
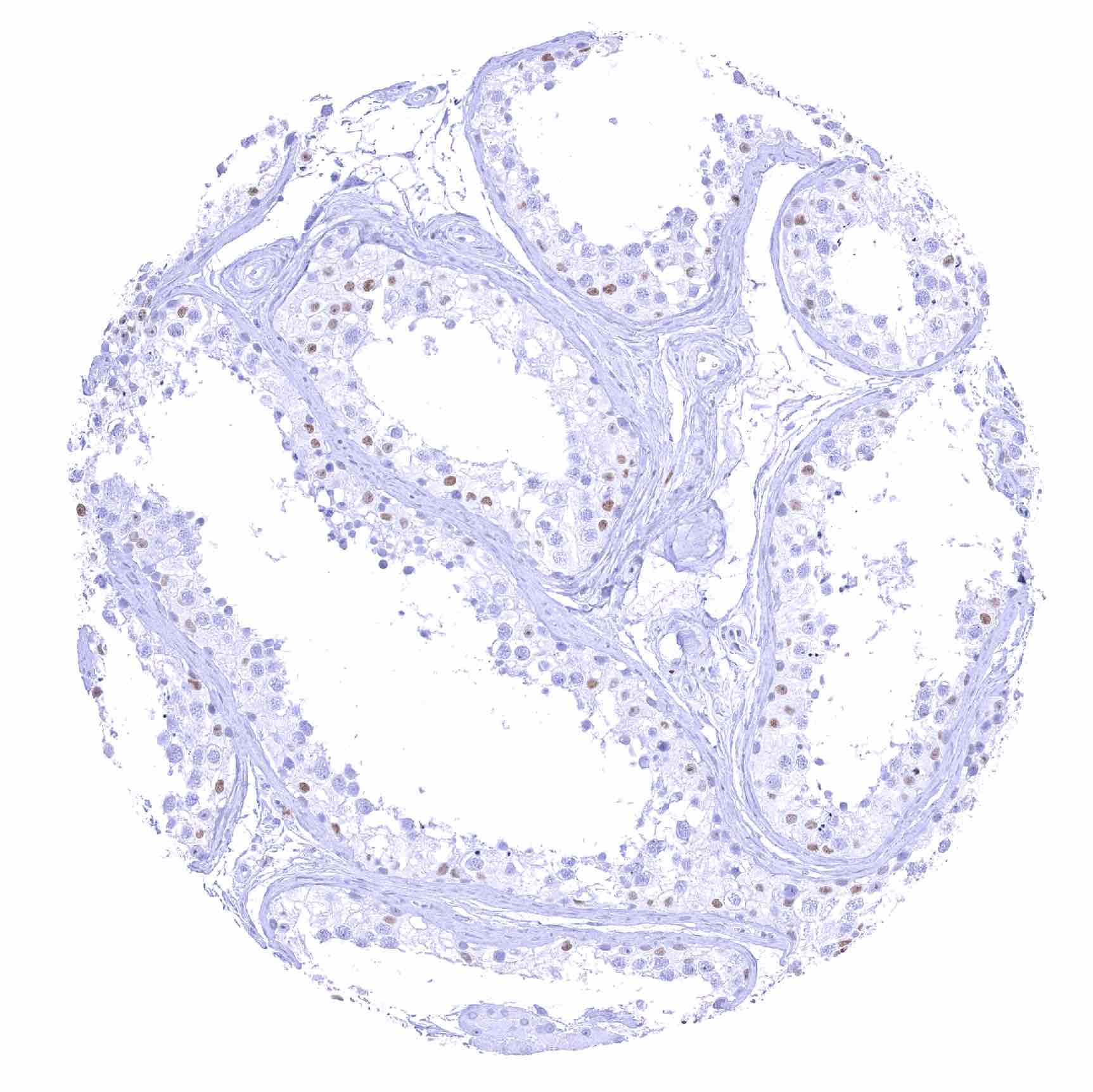
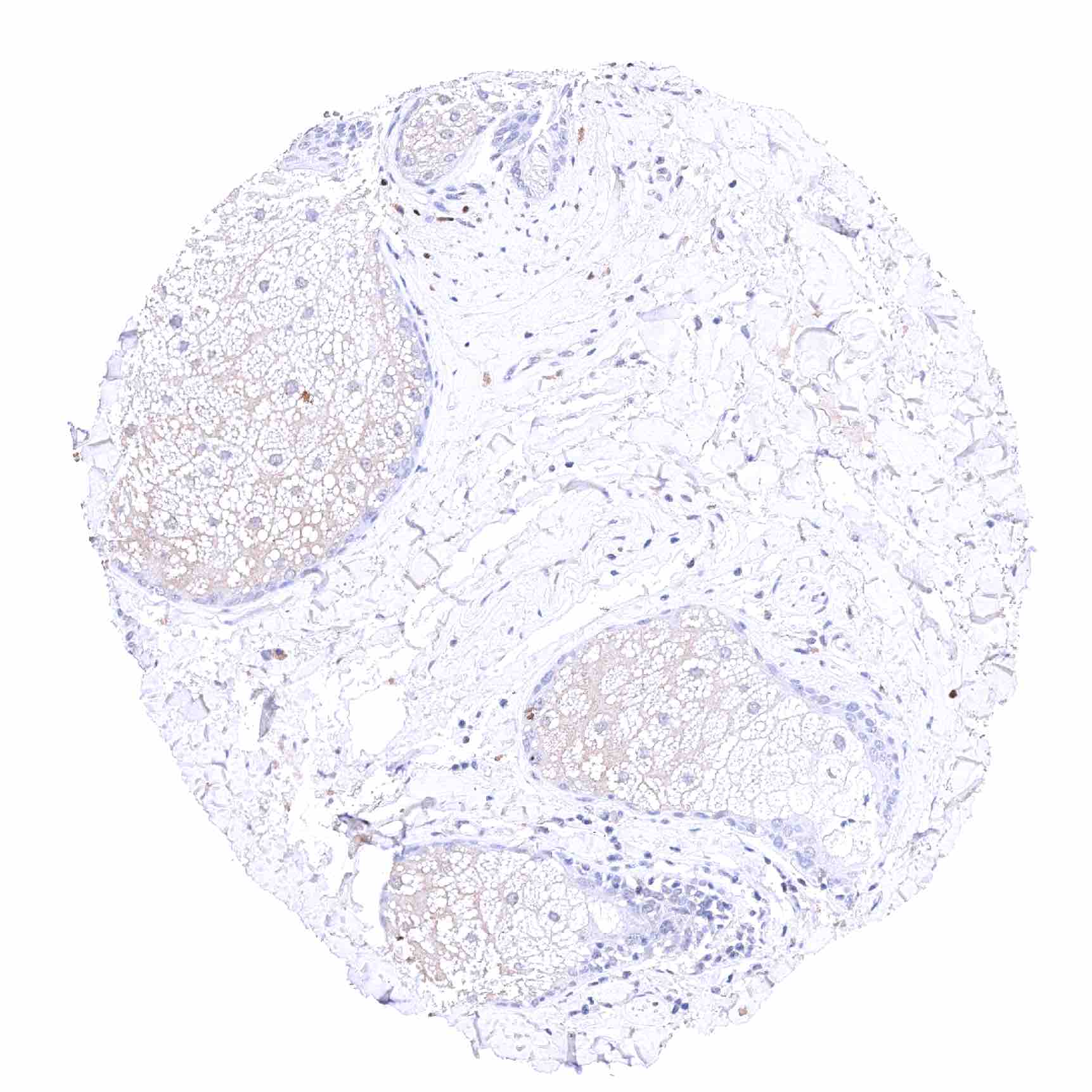
| Testis | Weak to moderate SOX2 positivity of spermatocytes. | |
| Epididymis | Negative. | |
| Female genital | Breast | Very faint positivity of acinar breast epithelial cells. |
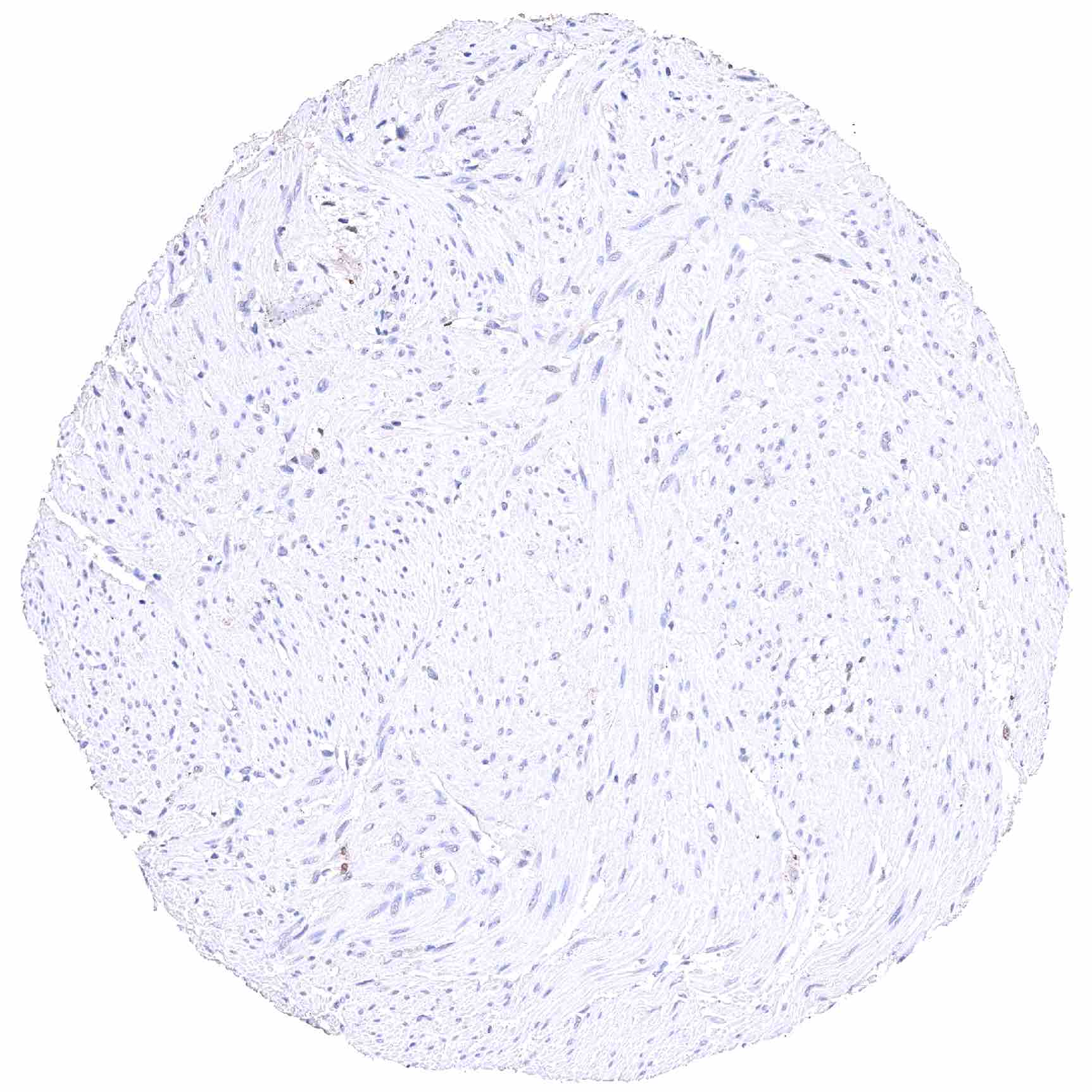
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Weak to moderate SOX2 positivity of squamous epithelial cells, especially in the lower 2/3. | |
| Uterus endocervix | Weak to moderate SOX2 positivity of endocervical cells (not in all samples). | |
| Uterus, endometrium | Negative. | |
| Fallopian Tube | Weak to strong SOX2 positivity of a large subset of epithelial cells. | |
| Ovary | Negative. | |
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | Negative. | |
| Chorion | Negative. | |
| Skin | Epidermis | Strong SOX2 positivity few epidermis-adjacent spindle shaped (neural?) cells in the dermis. Squamous epithelial cells are SOX2 negative. |
| Sebaceous glands | Strong SOX2 positivity few hair follicle-adjacent spindle shaped (neural?) cells in the dermis. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/ lymphoid tissue | Bone marrow | Negative. |
| Lymph node | Negative. | |
| Spleen | Negative. | |
| Thymus | Weak to strong SOX2 staining of a fraction of cells of corpuscles of Hassall’s. Lymphocytes and other immune cells are SOX2 negative. | |
| Tonsil | Weak to strong SOX2 positivity of squamous epithelial cells, especially in the lower 2/3. Lymphocytes and other immune cells are SOX2 negative. | |
| Remarks |
These findings are largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression SOX2). SOX2 staining by HMV338 is most prominent in tissues covered by non-keratinizing squamous epithelium, pituitary gland, brain, stomach, but also occurs in selected cell types of other organs.
Positive control = Tonsil: A moderate to strong SOX2 staining should be seen in the bottom 2/3 of squamous epithelial cells.
Negative control = Tonsil: SOX2 staining should be absent in lymphocytes and in other immune cells.
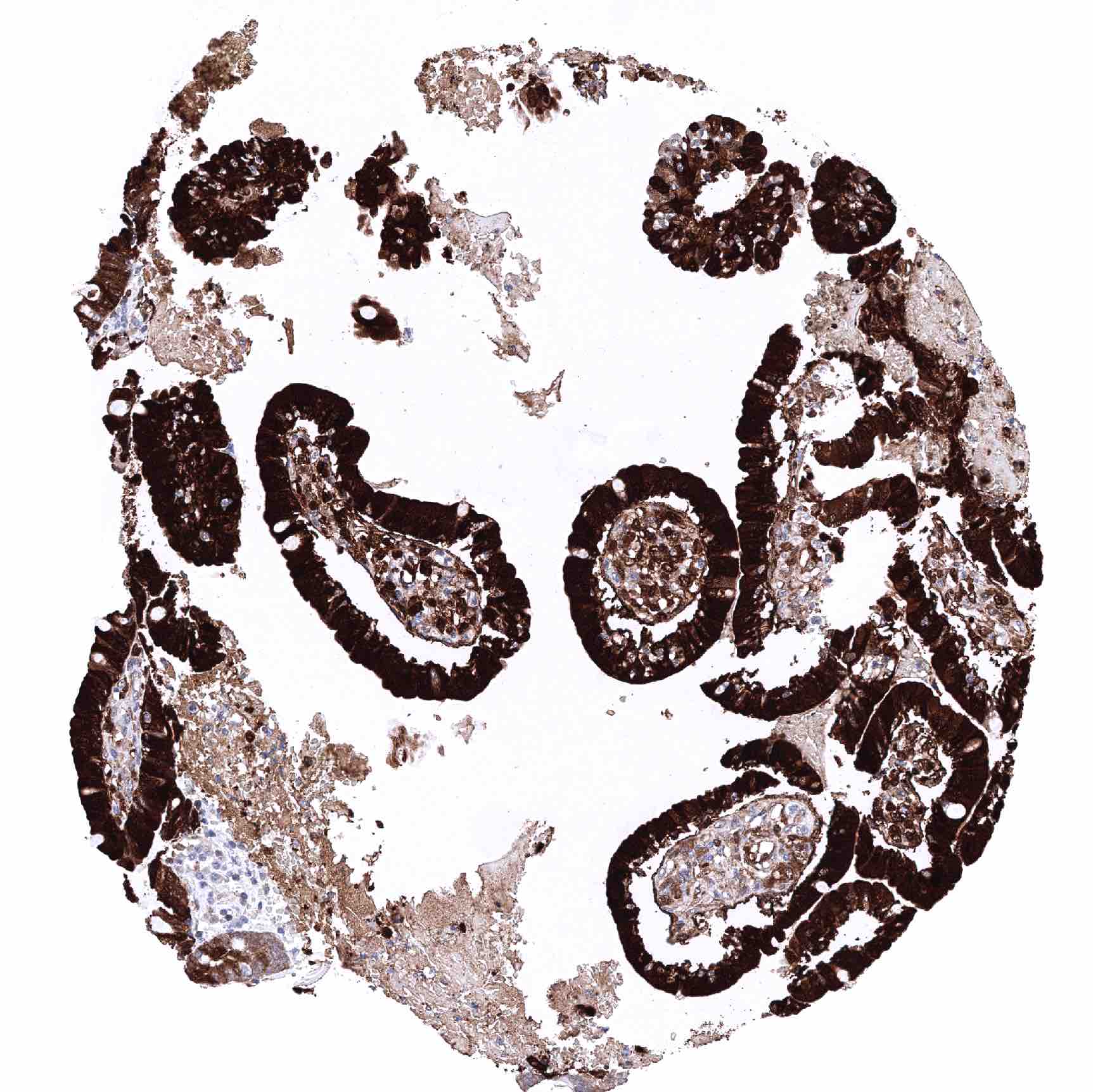
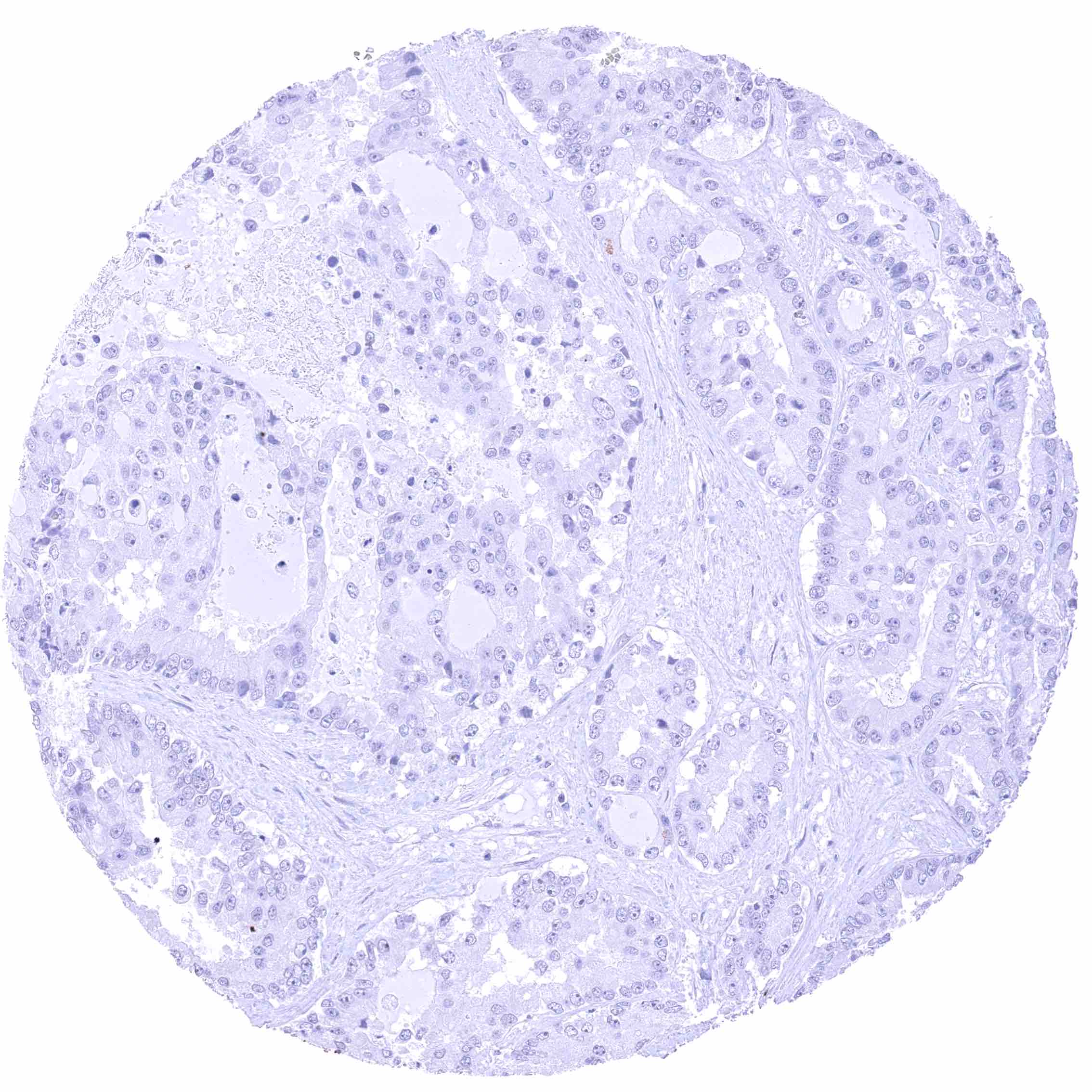
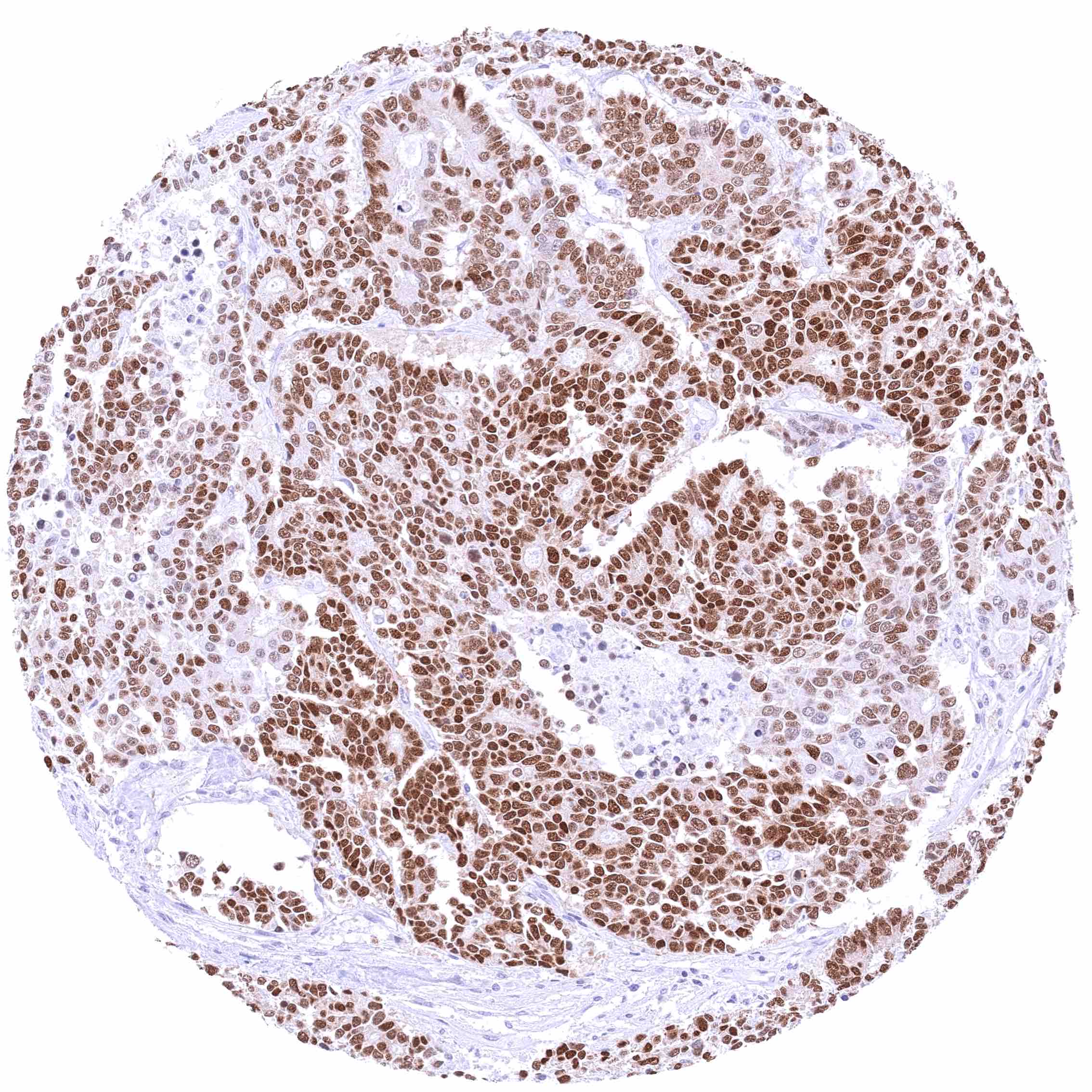
Staining Pattern in Relevant Tumor Types
SOX2 is primarily expressed in squamous cell carcinomas of various organs of origin. Less frequently, SOX2 expression also occurs in other tumor types.
The TCGA findings on SOX2 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply HMV338 at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The diagnostic, prognostic, and predictive relevance of SOX2 expression in tumors and in preneoplastic disease needs to be further investigated.
- SOX2 may play a functional role in cancer drug resistance.
- SOX2 represents a promising therapeutic target.
- SOX2 is a critical gene in stem cell research.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody HMV338 specificity is suggested by the good concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression SOX2).
SOX2 positivity by HMV338 is detectable in all tissues with documented SOX2 RNA expression (brain, hypophysis, salivary gland, esophagus, stomach, colon, testis, prostate, cervix uteri, fallopian tube, tonsil). Tissues without previously documented SOX2 RNA expression but SOX2 positivity by HMV338 had either very few positive cells that were probably not detected in RNA studies (corpuscles of Hassall’s in the thymus) or were previously not analyzed on the RNA level (respiratory epithelium, bronchial glands, paranasal sinus).
Comparison of antibodies: True expression of SOX2 in all cell types found SOX2 positive by HMV338 (including corpuscles of Hassall’s in the thymus, respiratory epithelium in the bronchus and the paranasal sinus, bronchial glands) is corroborated by the staining of all these cell types by another commercially available independent antibody (termed “validation antibody”). Independence of the validation antibody is demonstrated by substantial cytoplasmic staining in various tissues by the validation antibody.