295,00 € – 995,00 €
Product details
Synonyms = GCP2, FOLH1, NAALADase I, PGGCP, FGGCP, FGCP
Antibody type = Mouse monoclonal
Clone = ARX-752
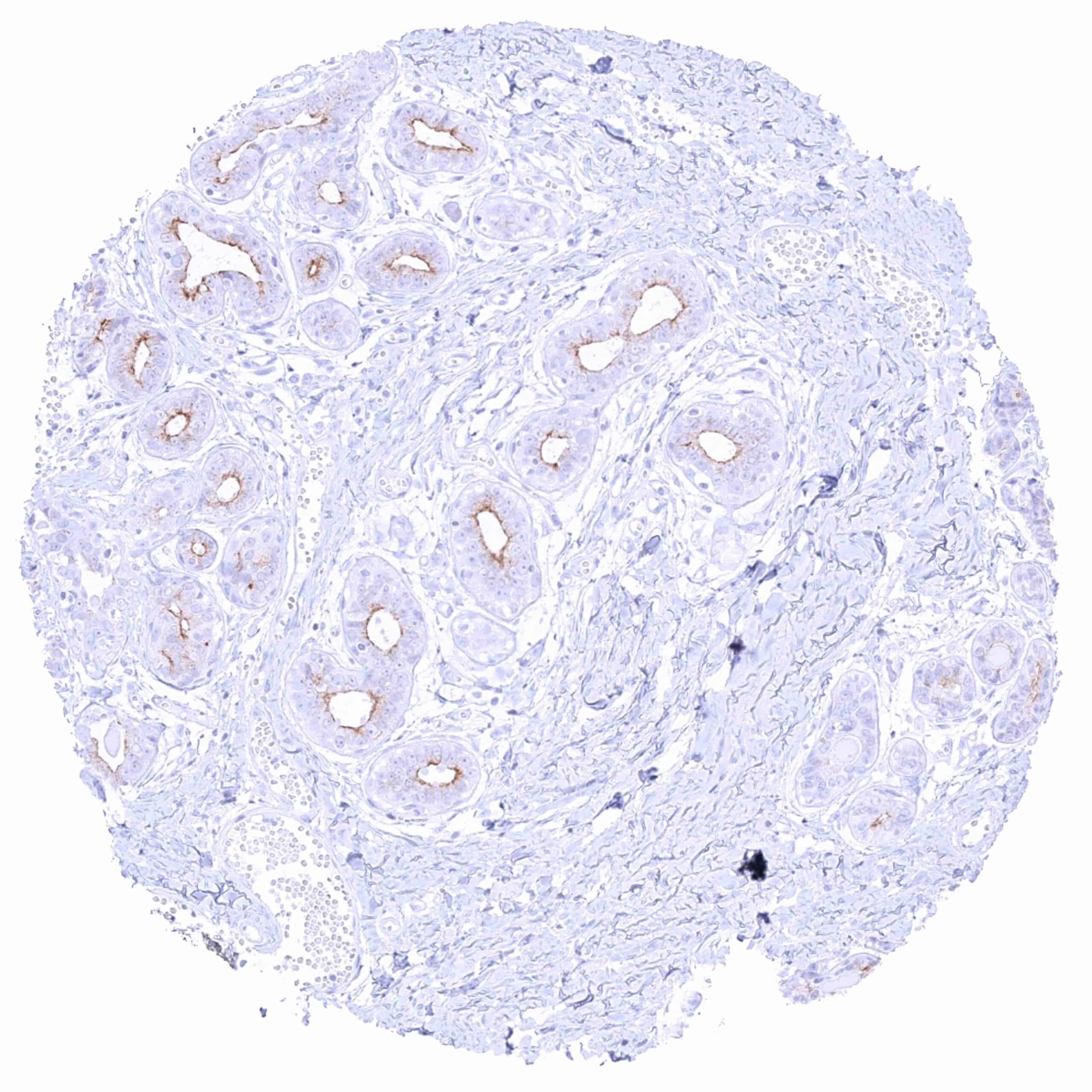
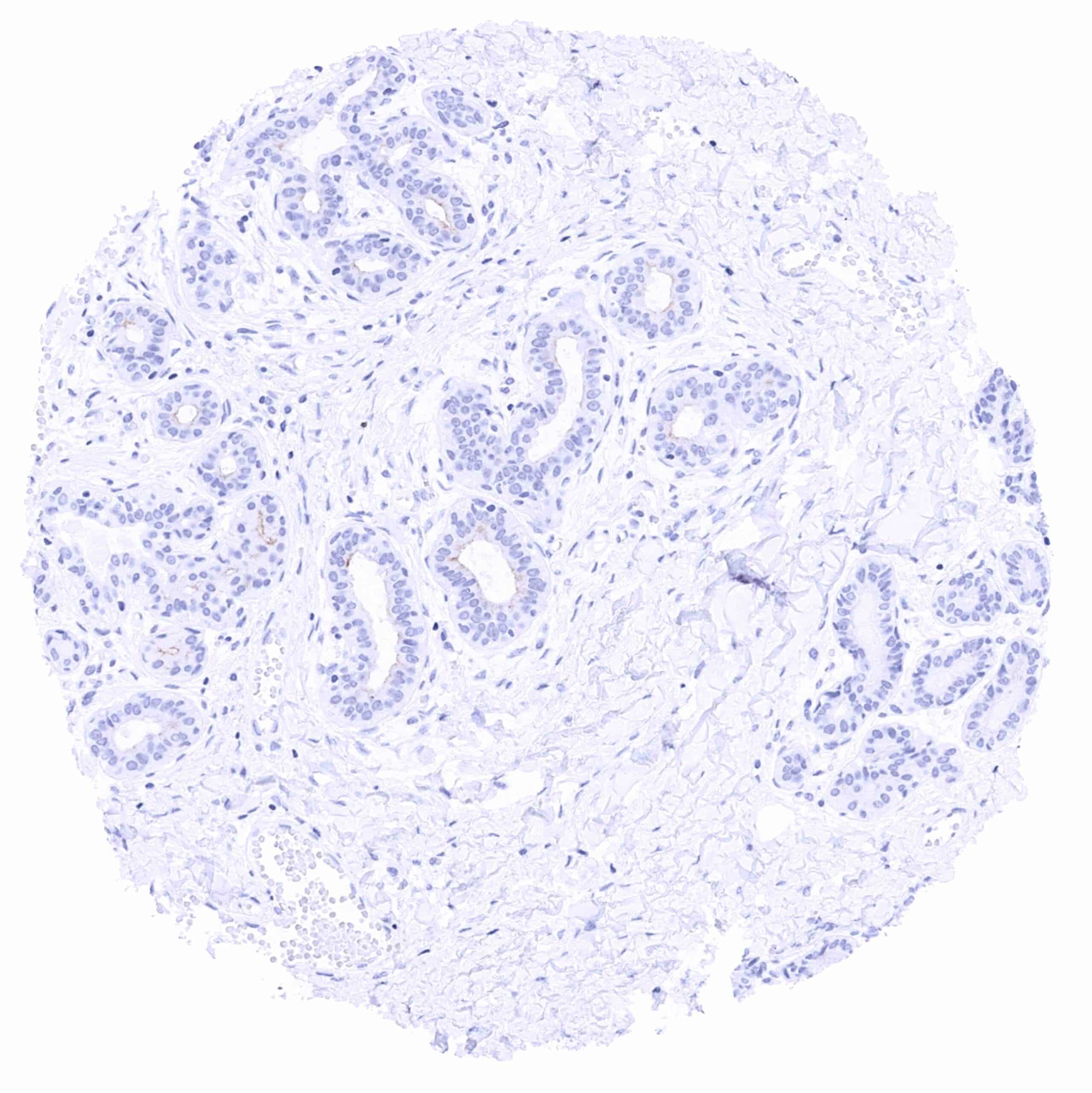
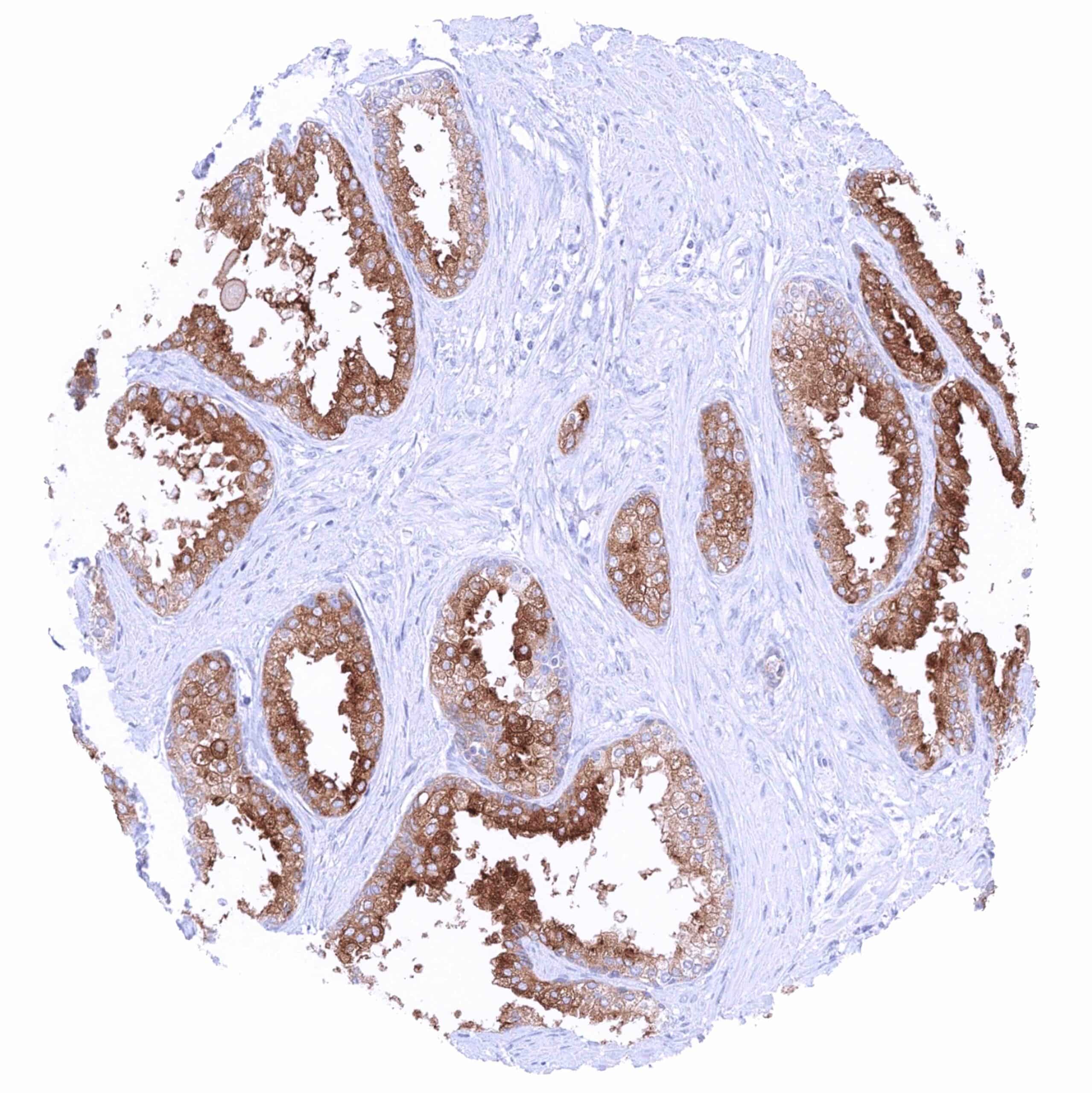
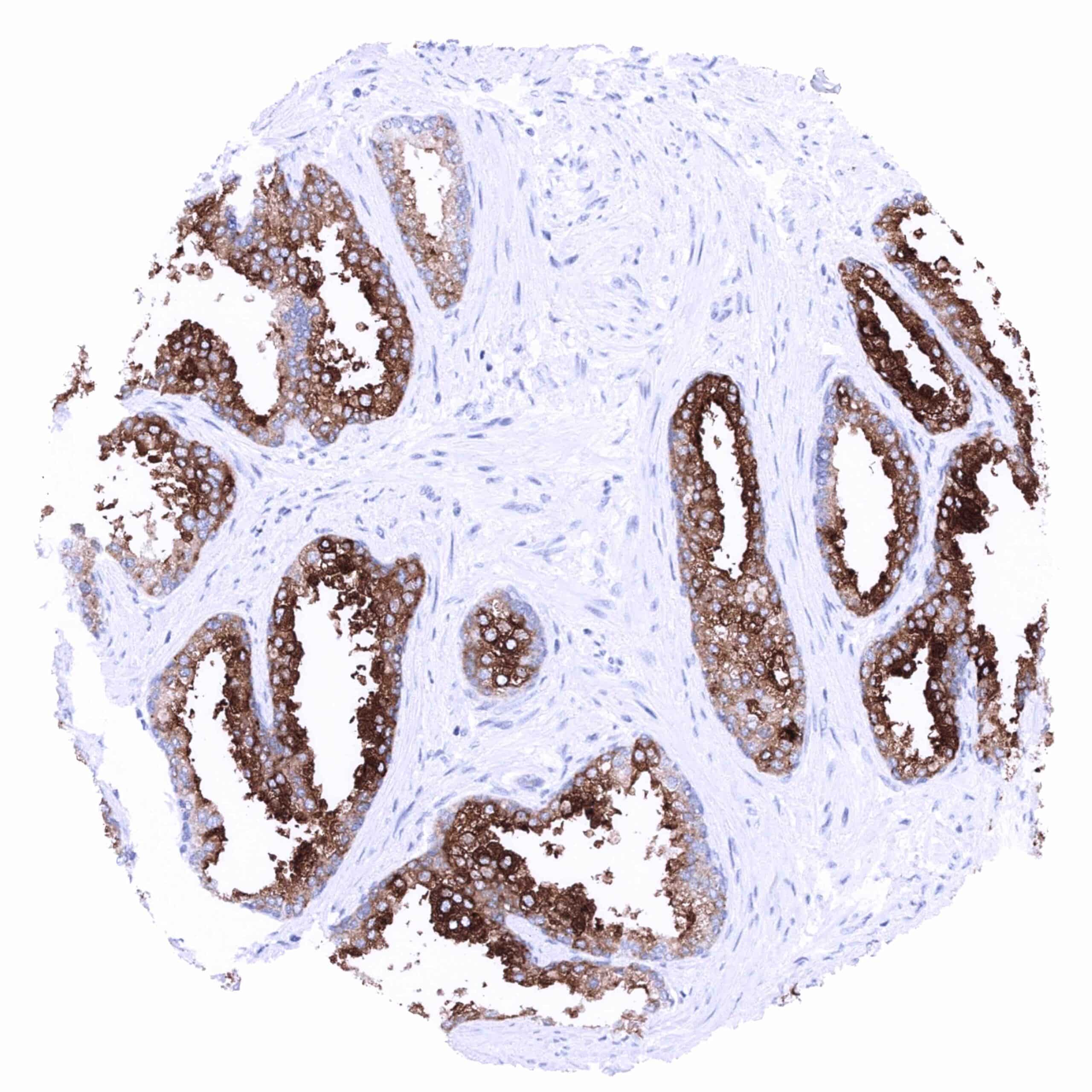
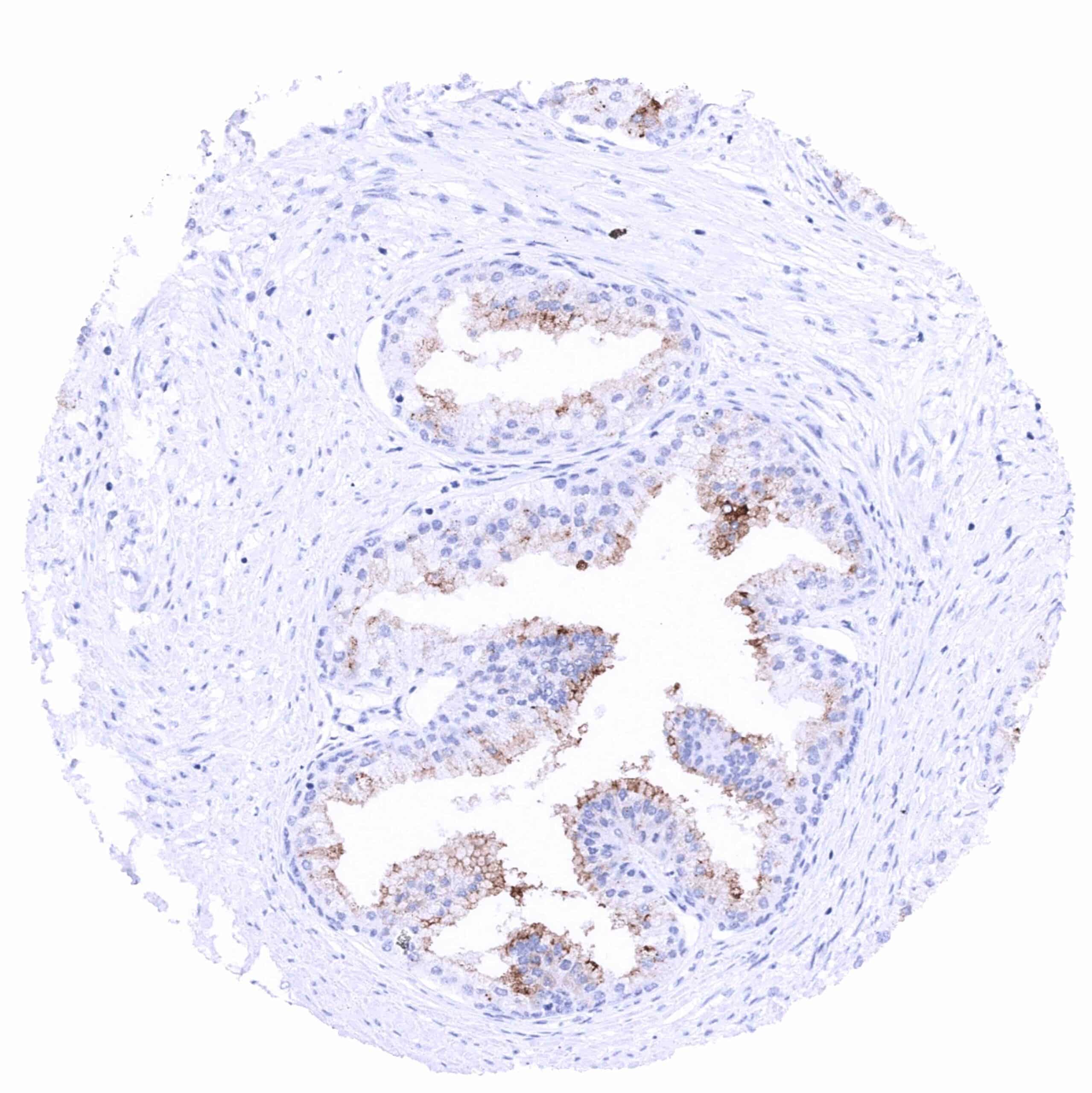
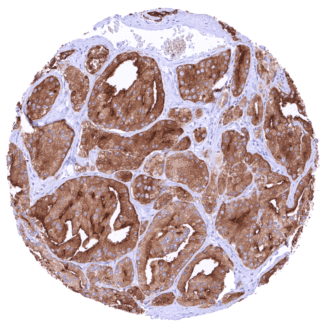
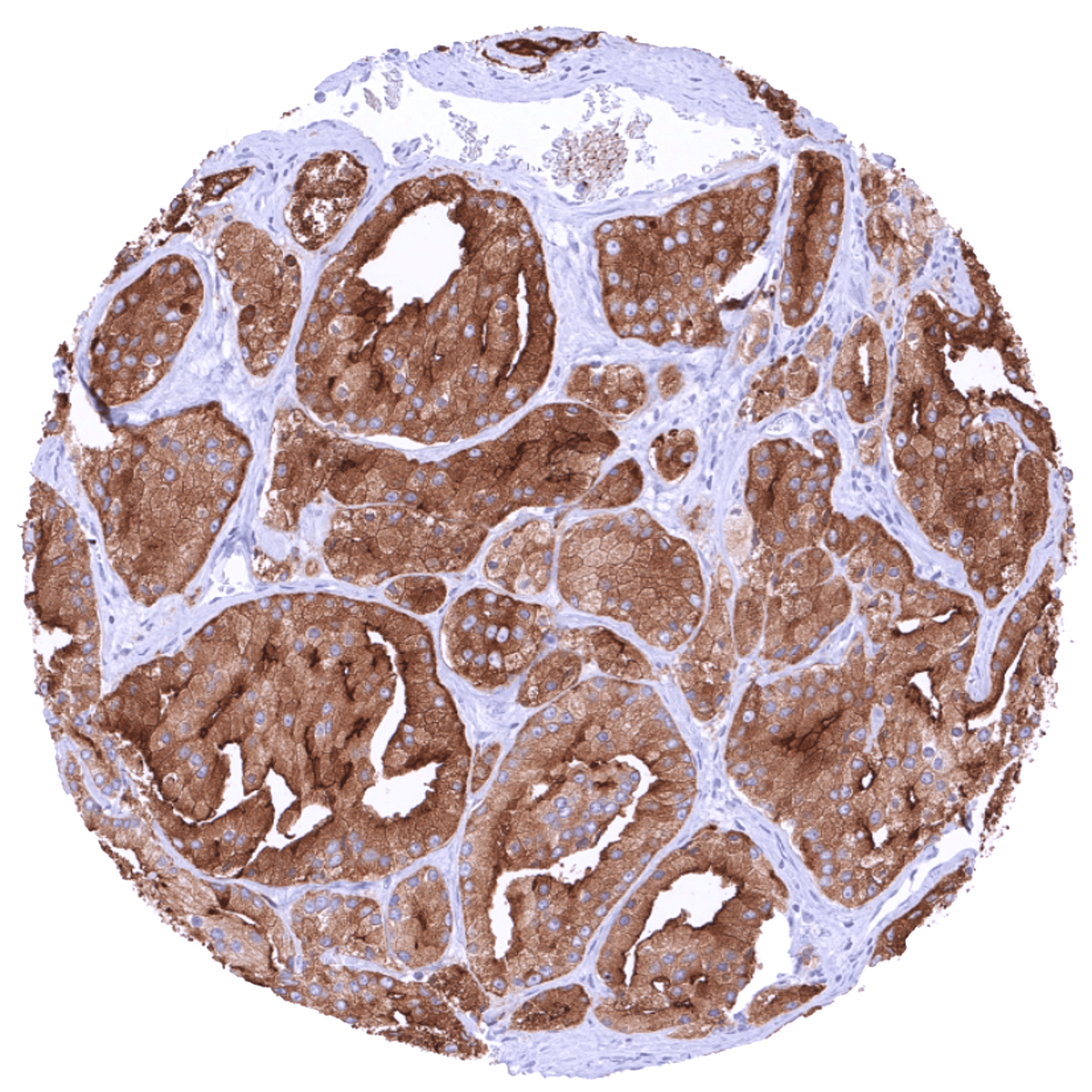
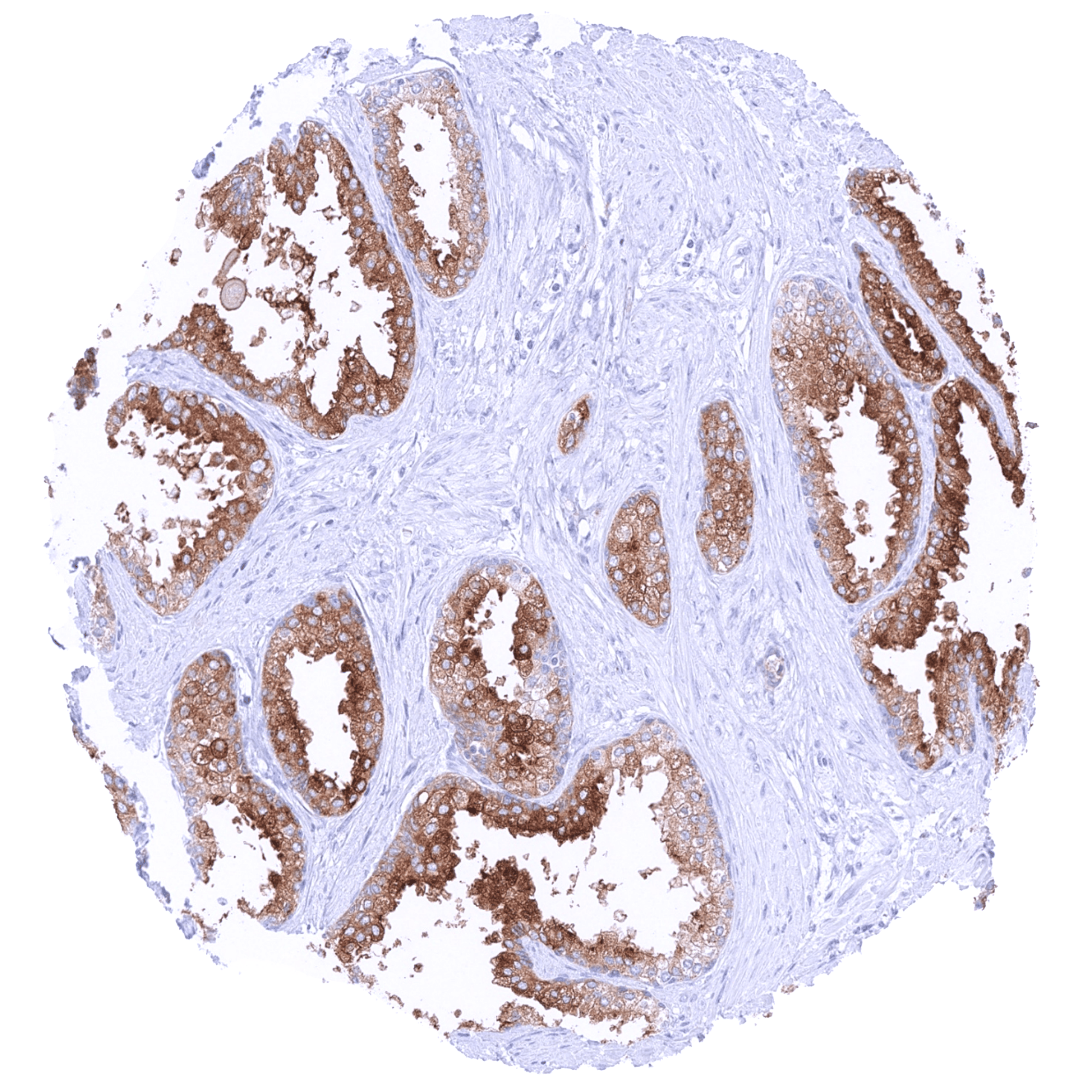
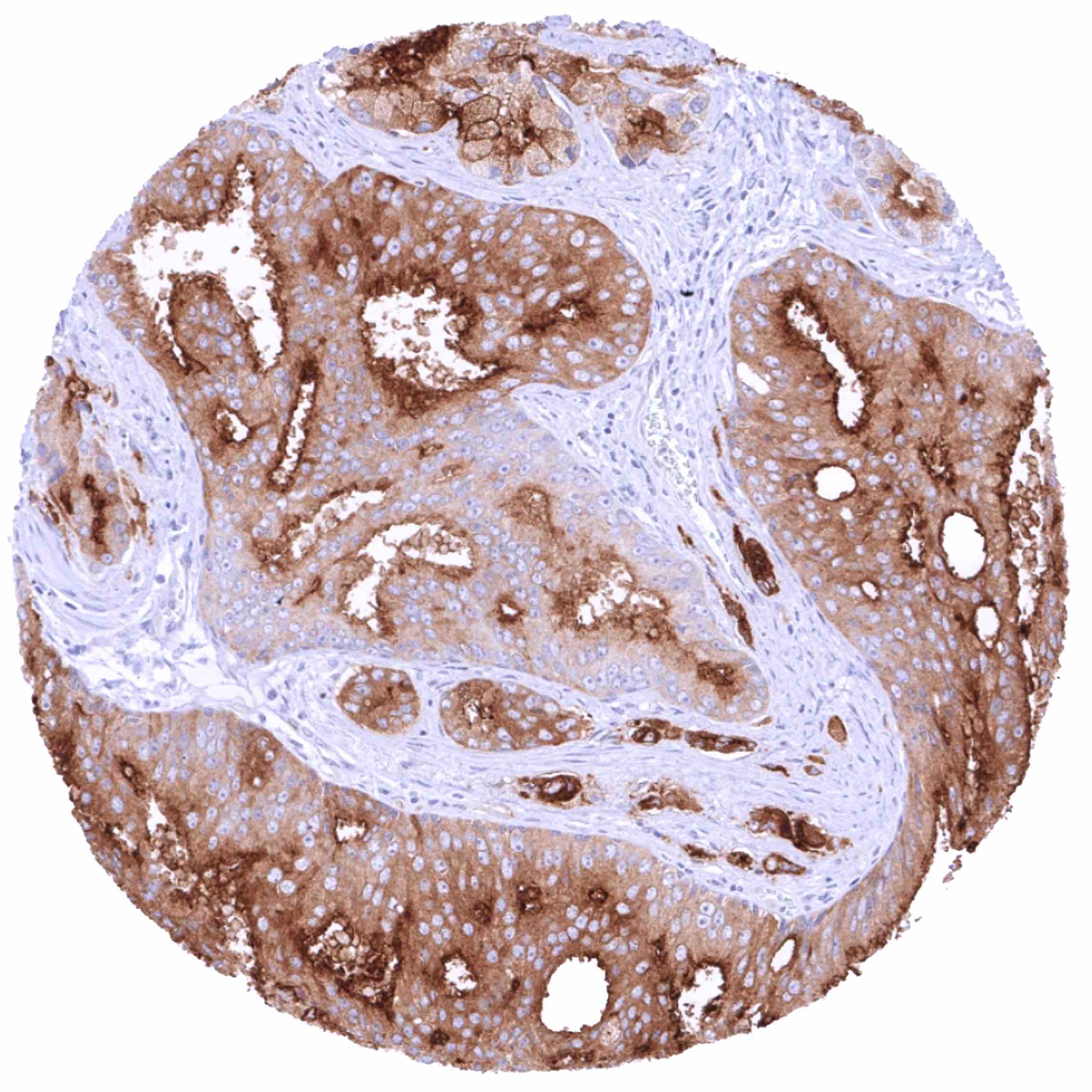
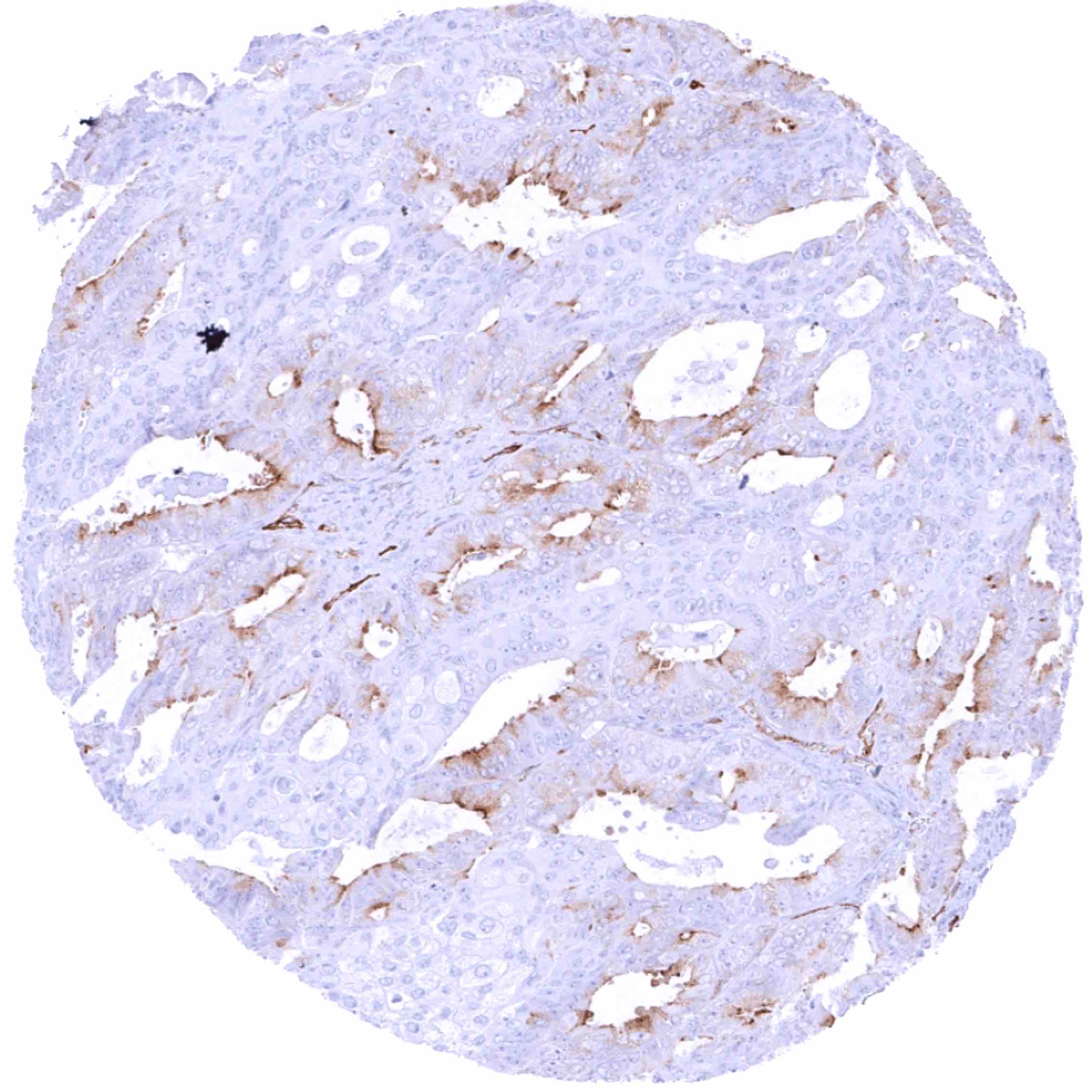
Positive control = Prostate: A moderate to strong PSMA staining should be seen in the cytoplasm and at the apical/luminal membrane of acinar epithelial cells.
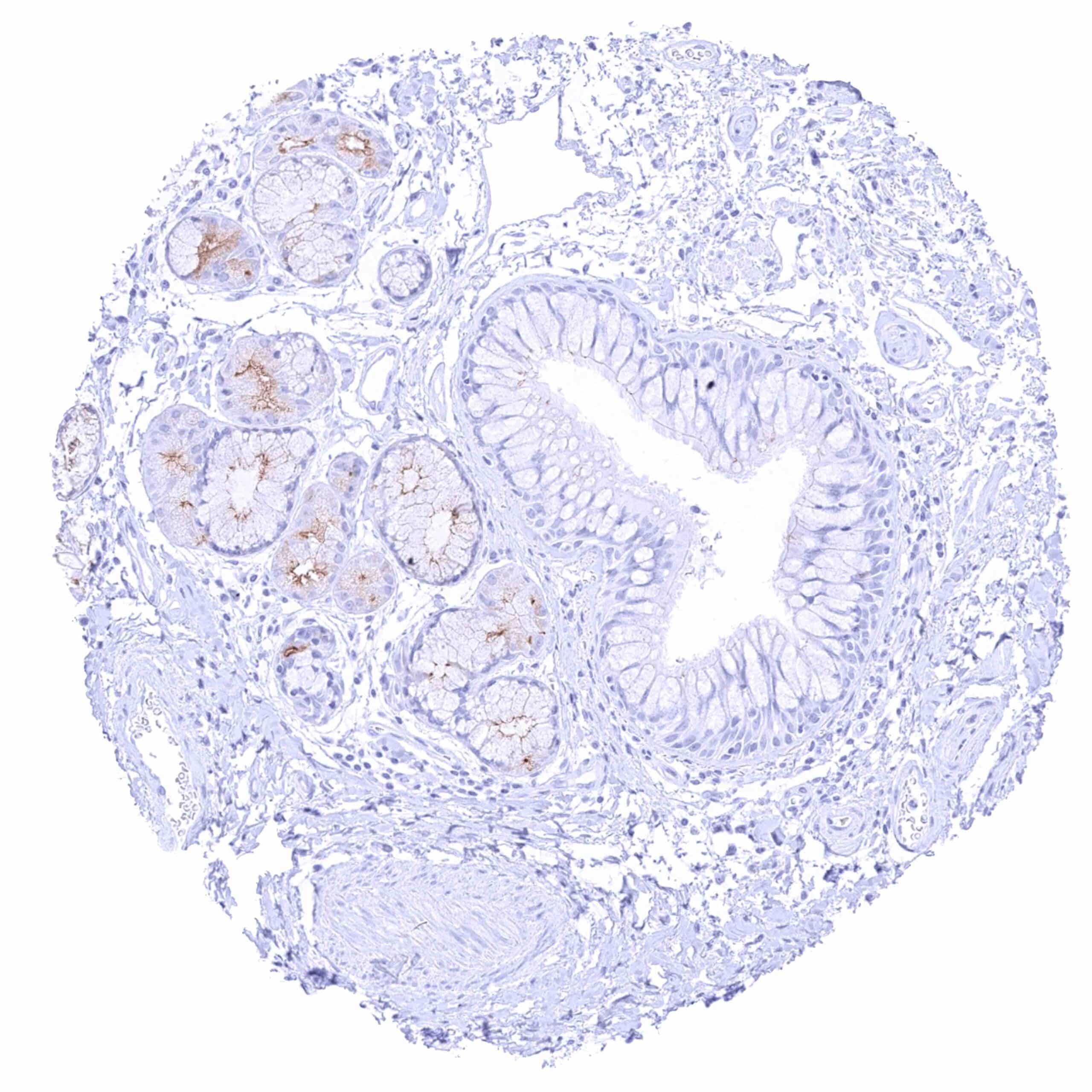
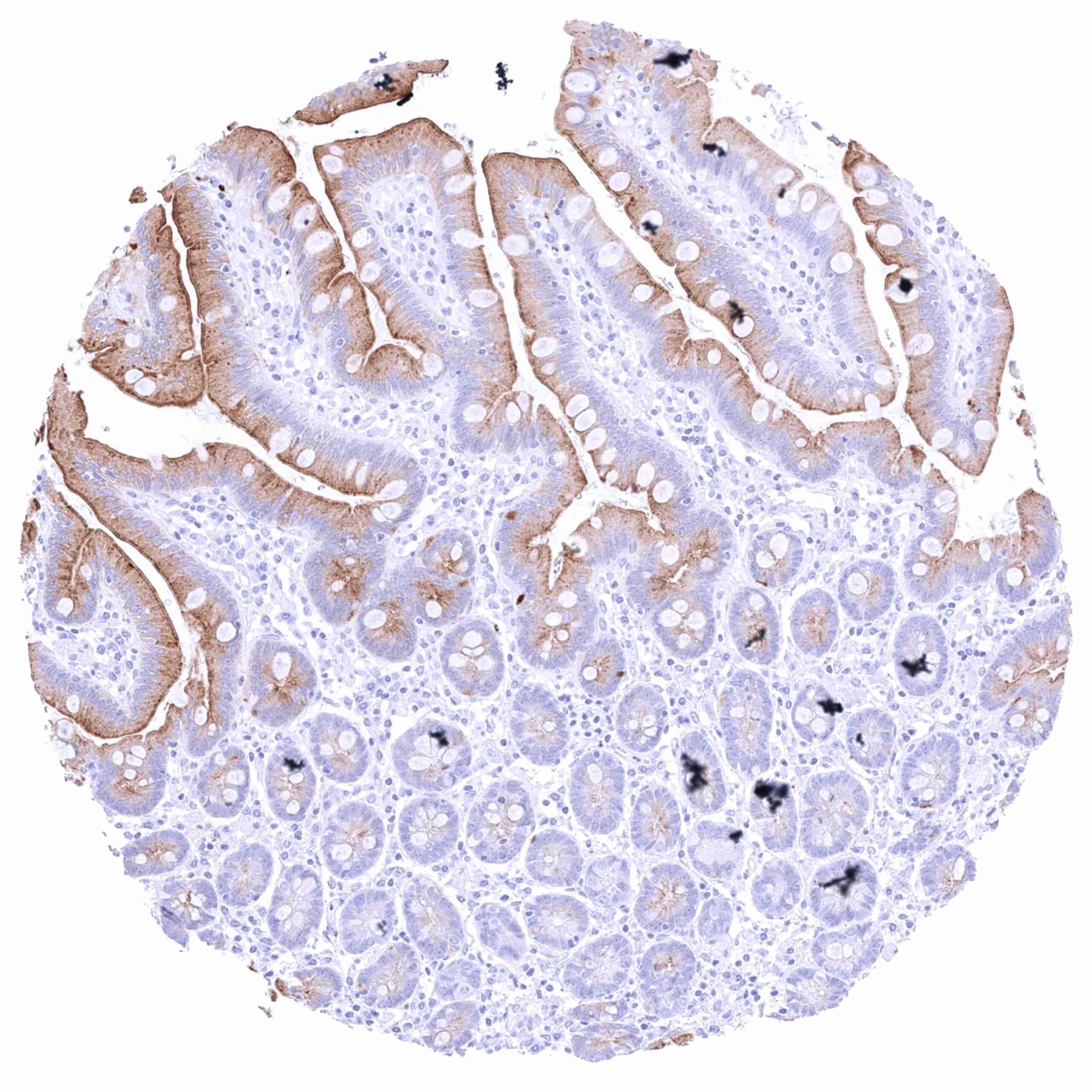
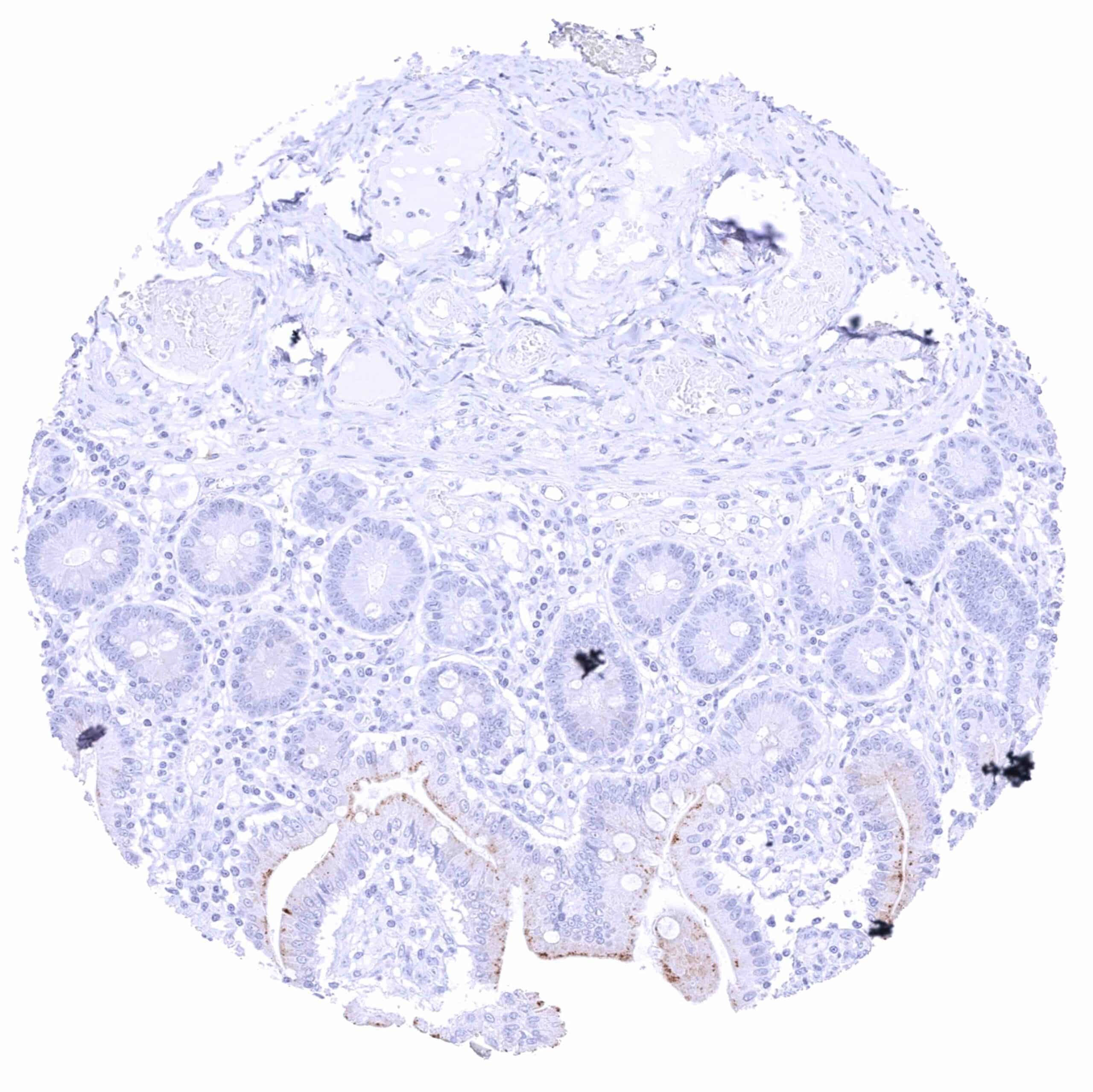
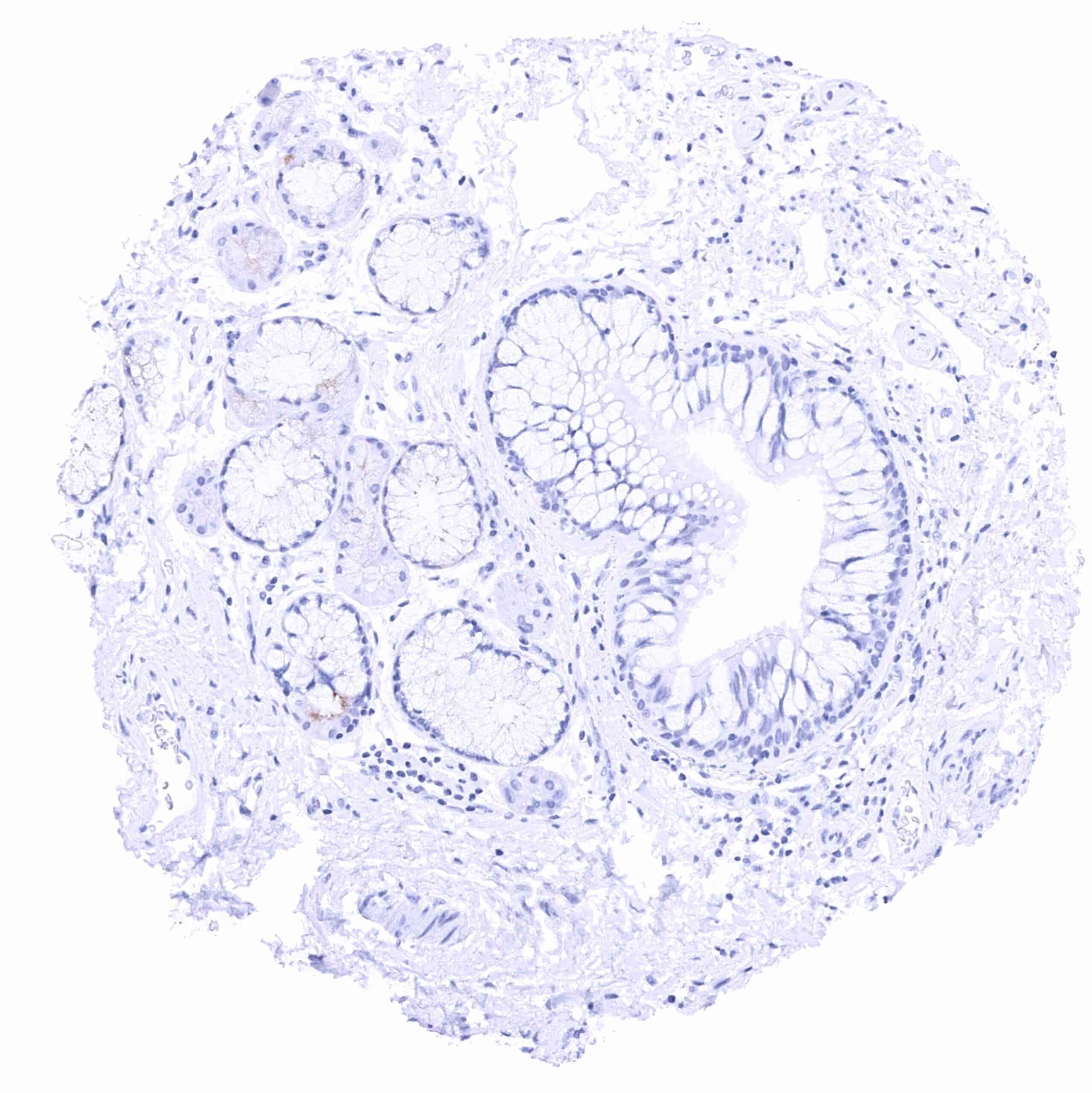
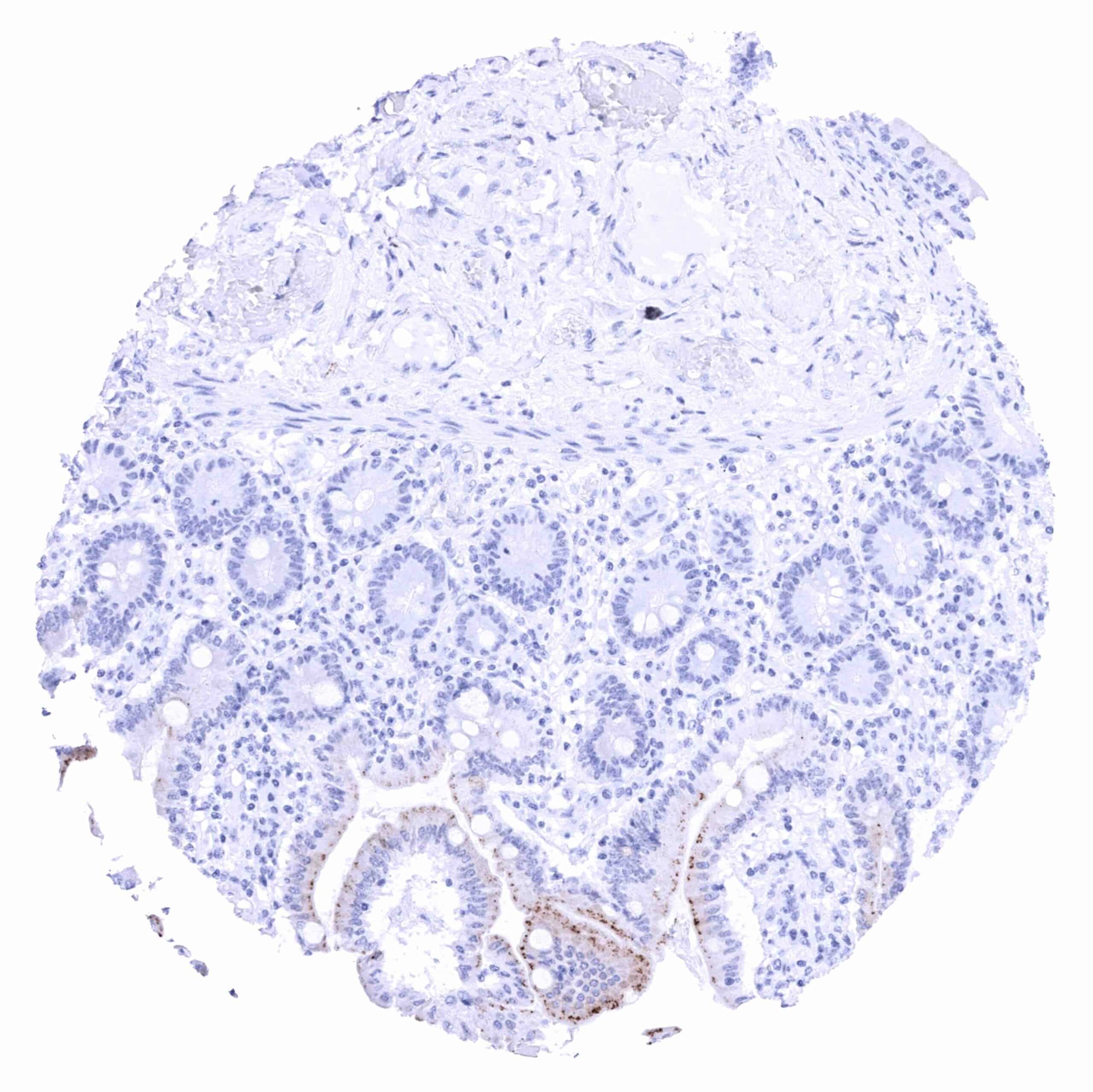
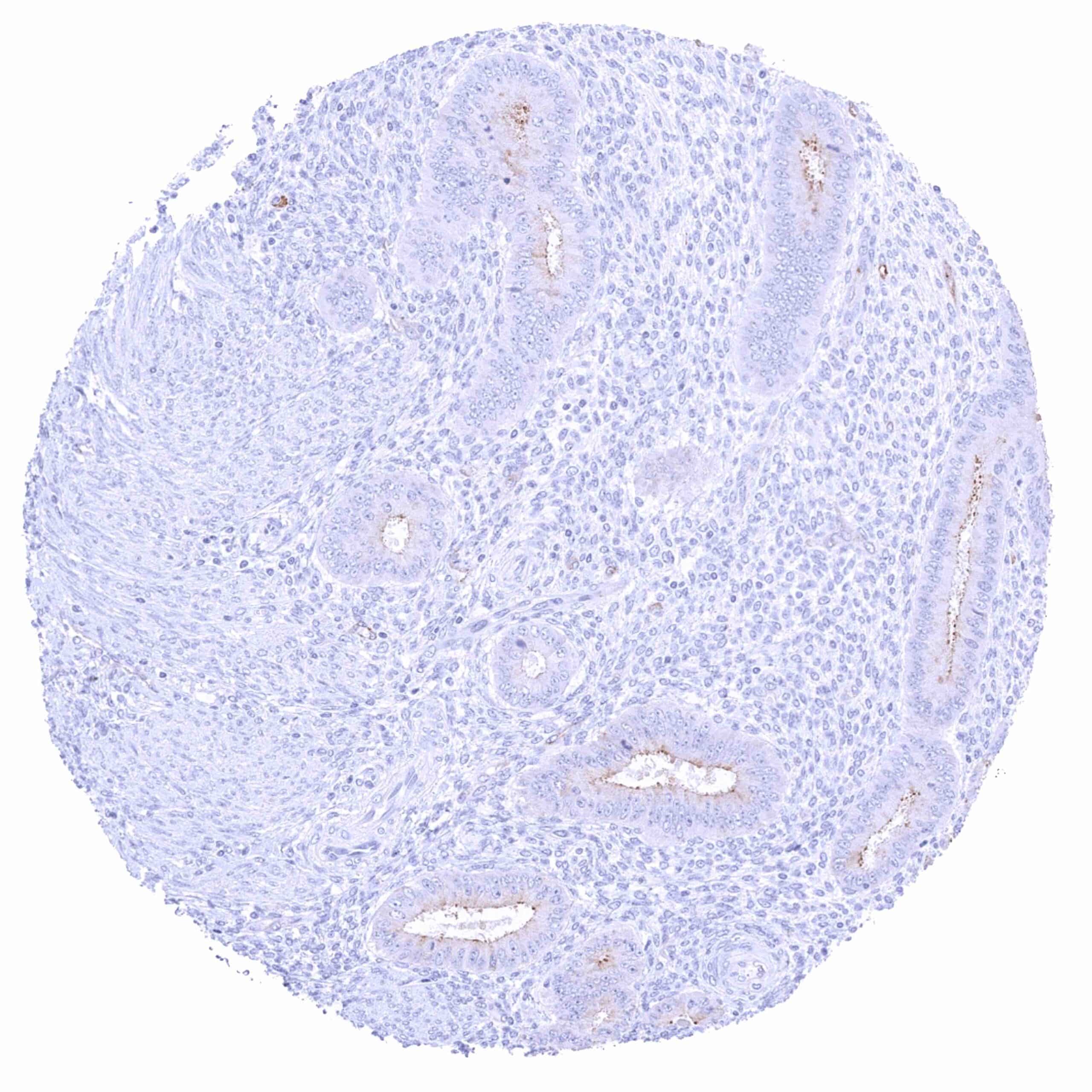
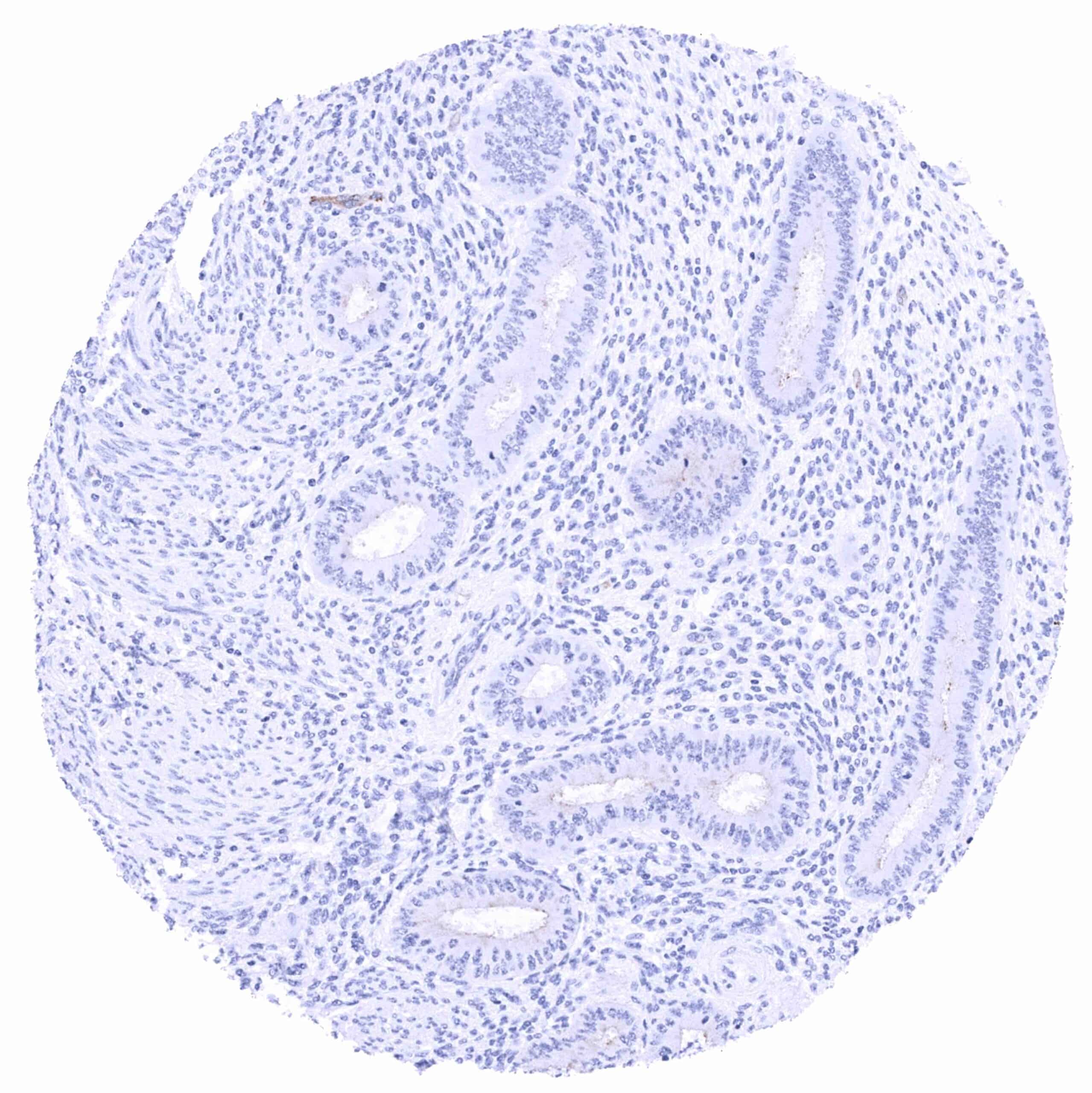
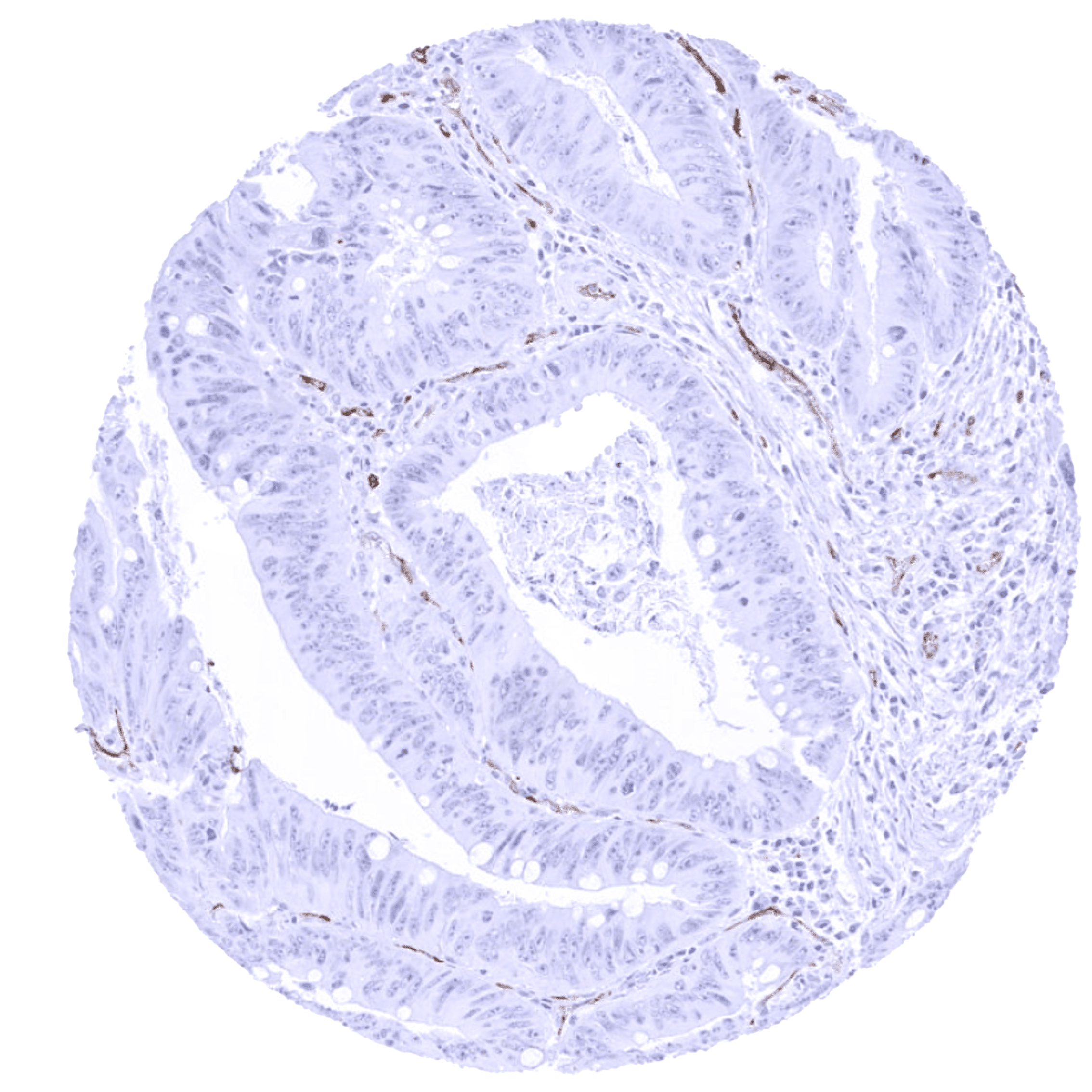
Negative control = Colon: PSMA staining must be completely absent in all cell types.
Cellular localization = Membranous
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
PSMA is a marker for prostate cancer and therapeutic target.
Biology Behind
Prostate-specific membrane antigen (PSMA), also termed N-acetyl-L-aspartyl-L-glutamate peptidase I (NAALADase I), NAAG peptidase, glutamate carboxypeptidase II (GCPII), or FOLH1 (folate hydrolase 1) is a class II membrane glycoprotein that is encoded by the FOLH1 gene on chromosome 11p11.12. PSMA is a 84kDa zinc metalloenzyme composed of 750 amino acids which is preferentially expressed in the small intestine, the prostate, the kidney, and the brain. Its role is tissue specific. In the brain, it is needed for degradation of the neurotransmitter N-acetylaspartylglutamate (NAAG) into NAA and glutamate another excitatory neurotransmitter. As a high PSMA activity may result in neuronal glutamate-mediated excitotoxicity, PSMA inhibiting molecules have been proposed to improve the disease course in several neurological and psychiatric diseases. At the jejunal brush border, PSMA is responsible for folate absorption. PSMA in the prostate and the kidney may also be needed for processing folates as a reuptake of folate occurs in the kidney and monoglutamated folates are released into the seminal fluid. Most of the current interest in PSMA comes from its role in prostate cancer. Because of its frequent upregulation (up to 1000 fold as compared to normal prostatic epithelium), PSMA is rapidly gaining importance as a diagnostic and a therapeutic target protein. In particular, PSMA small molecule radioligands are now well established for diagnostic imaging and increasingly used for radiotherapy of prostate cancer. Also in other tumor types, PSMA appears to be involved in cancer-related angiogenesis by degrading the extracellular matrix and participating in integrin signal transduction.
Staining Pattern in Normal Tissues
PSMA is expressed in the small intestine, salivary glands, the prostate, the kidney, the brain as well as in several other tissue types.
Images describing the PSMA staining pattern in normal tissues obtained by the antibody ARX-752 are shown in our “Normal Tissue Gallery”.
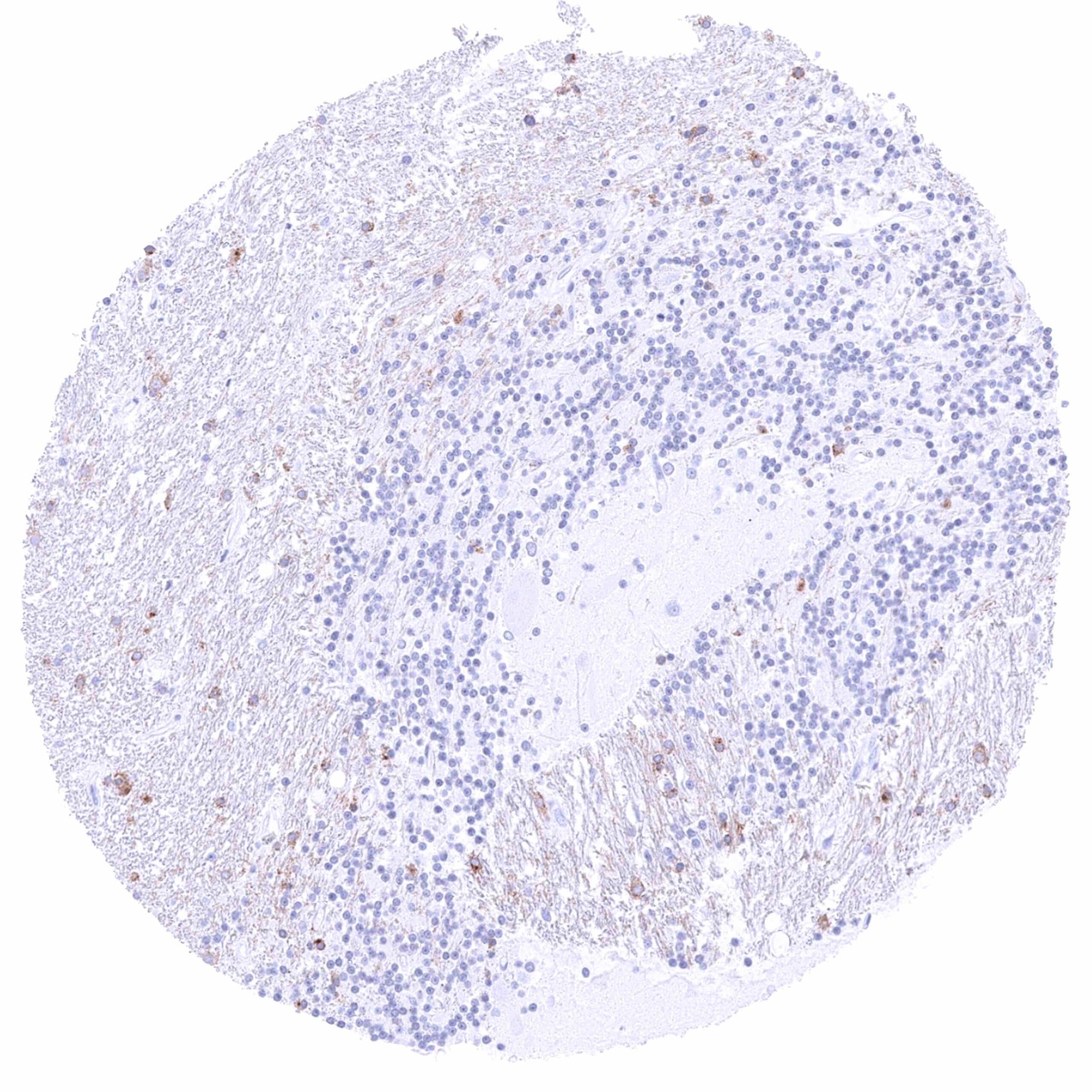
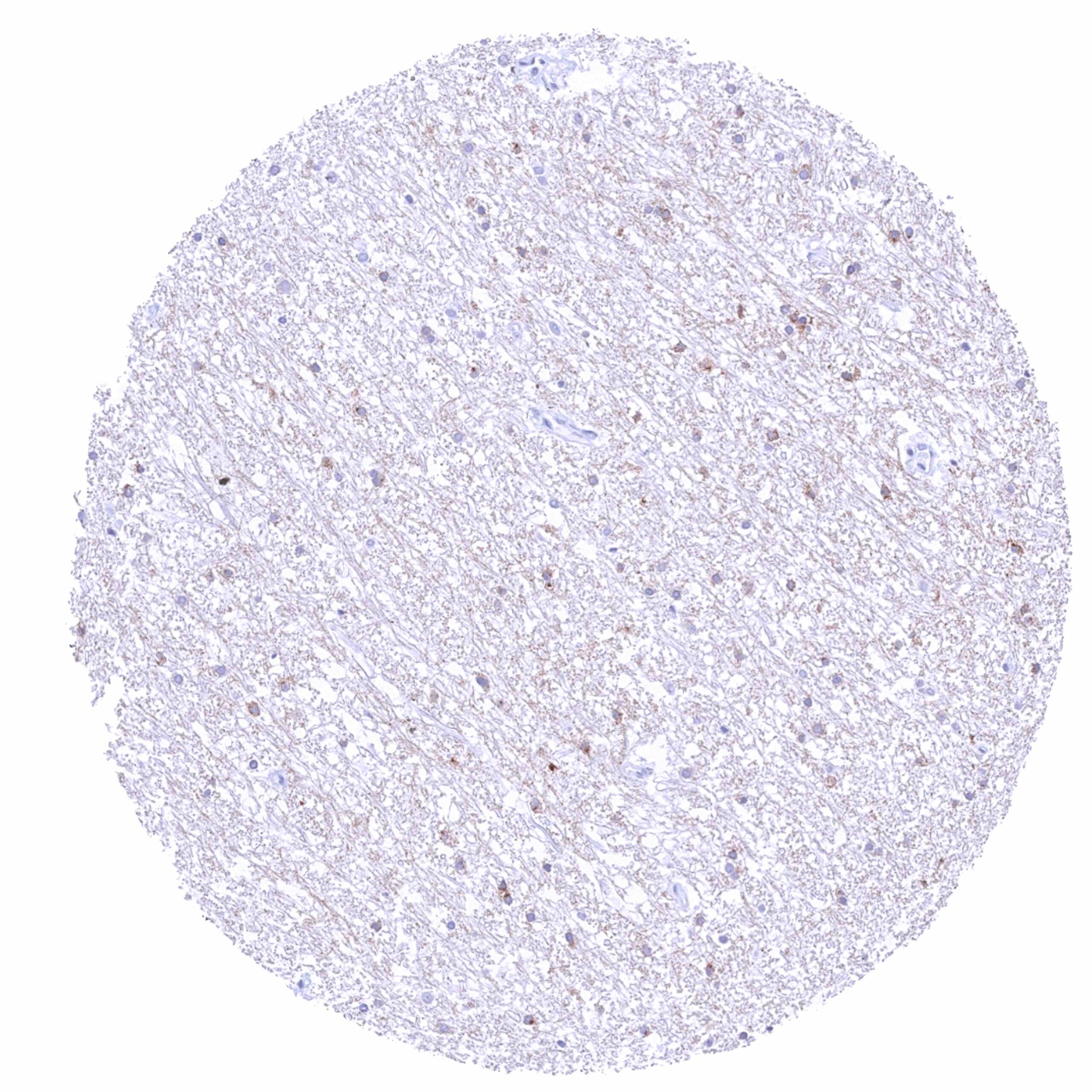
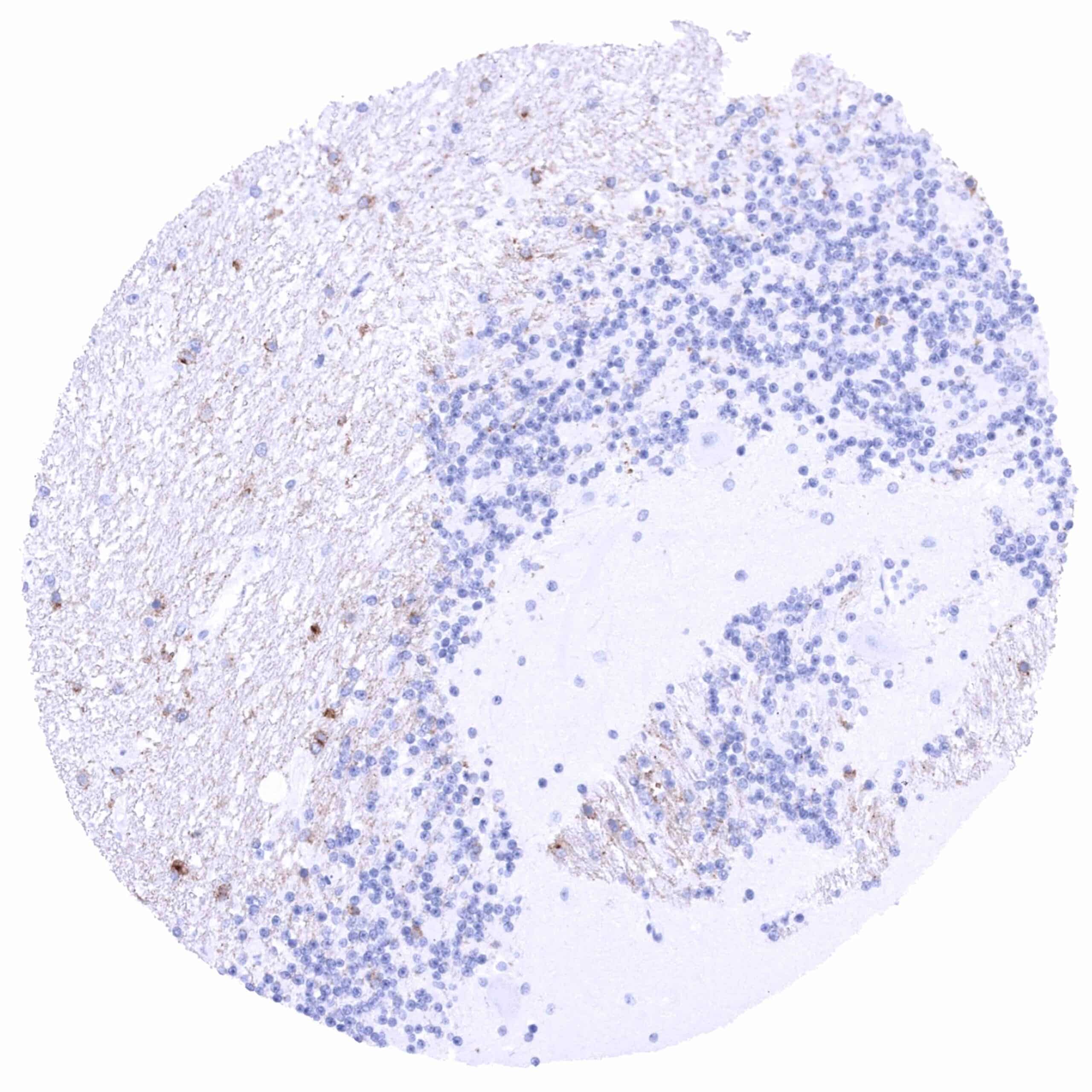
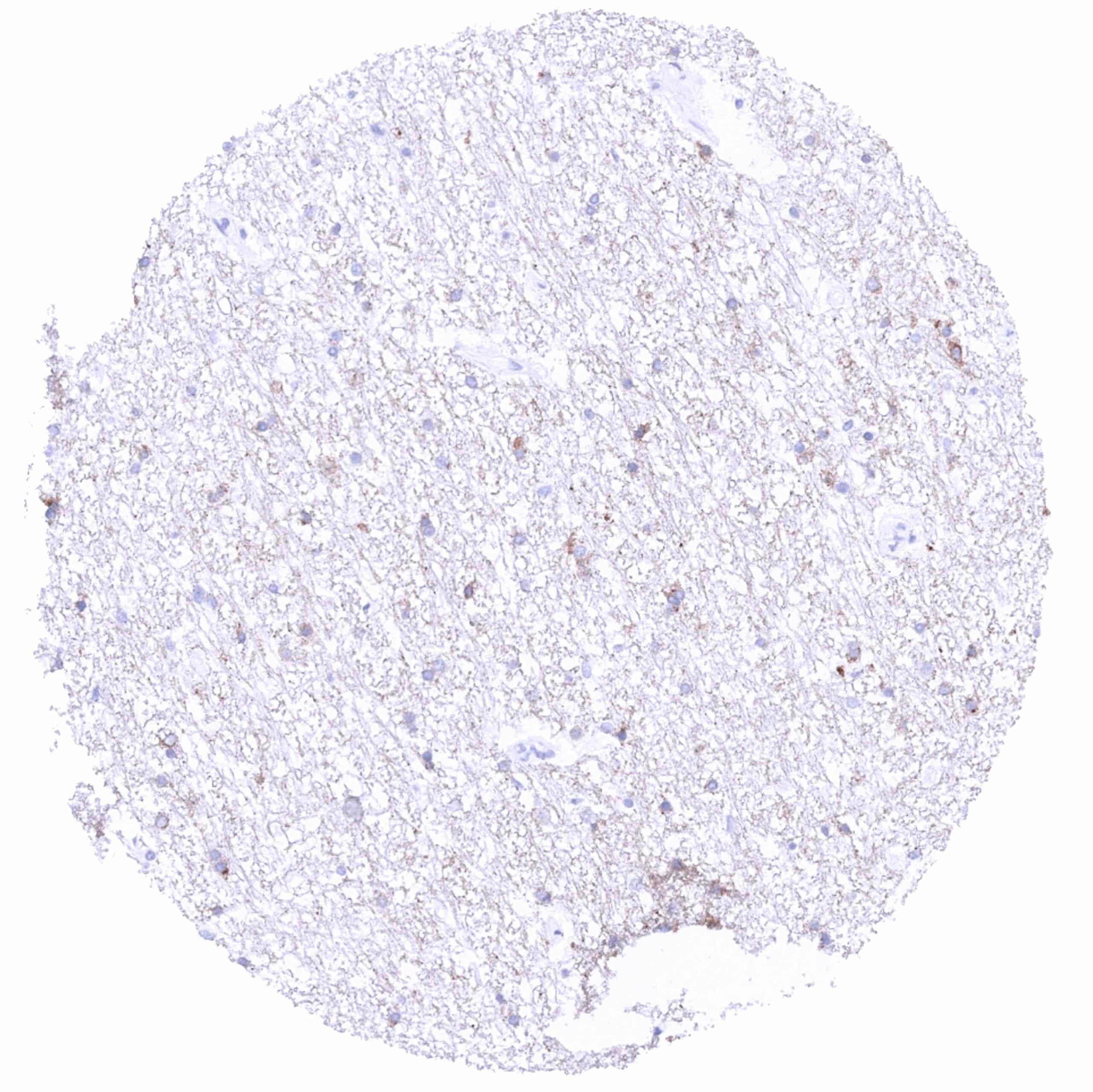
| Brain | Cerebrum | Distinct membranous staining of at least a fraction of glia cells in the white layer. Weak to moderate fibrillar PSMA staining in the white matter. The grey matter is PSMA negative. |
| Cerebellum | Distinct membranous staining of at least a fraction of glia cells in the white matter. Weak to moderate fibrillar PSMA staining in the white matter. Molecular layer, Purkinje cells, and the granule cell layer are PSMA negative. | |
| Endocrine Tissues | Thyroid | Negative. |
| Parathyroid | Negative. | |
| Adrenal gland | Negative. | |
| Pituitary gland | Negative. | |
| Respiratory system | Respiratory epithelium | Negative. Bronchial glands and glands of the paranasal sinus are PSMA positive (membranous apical and cytoplasmic). |
| Lung | Negative. | |
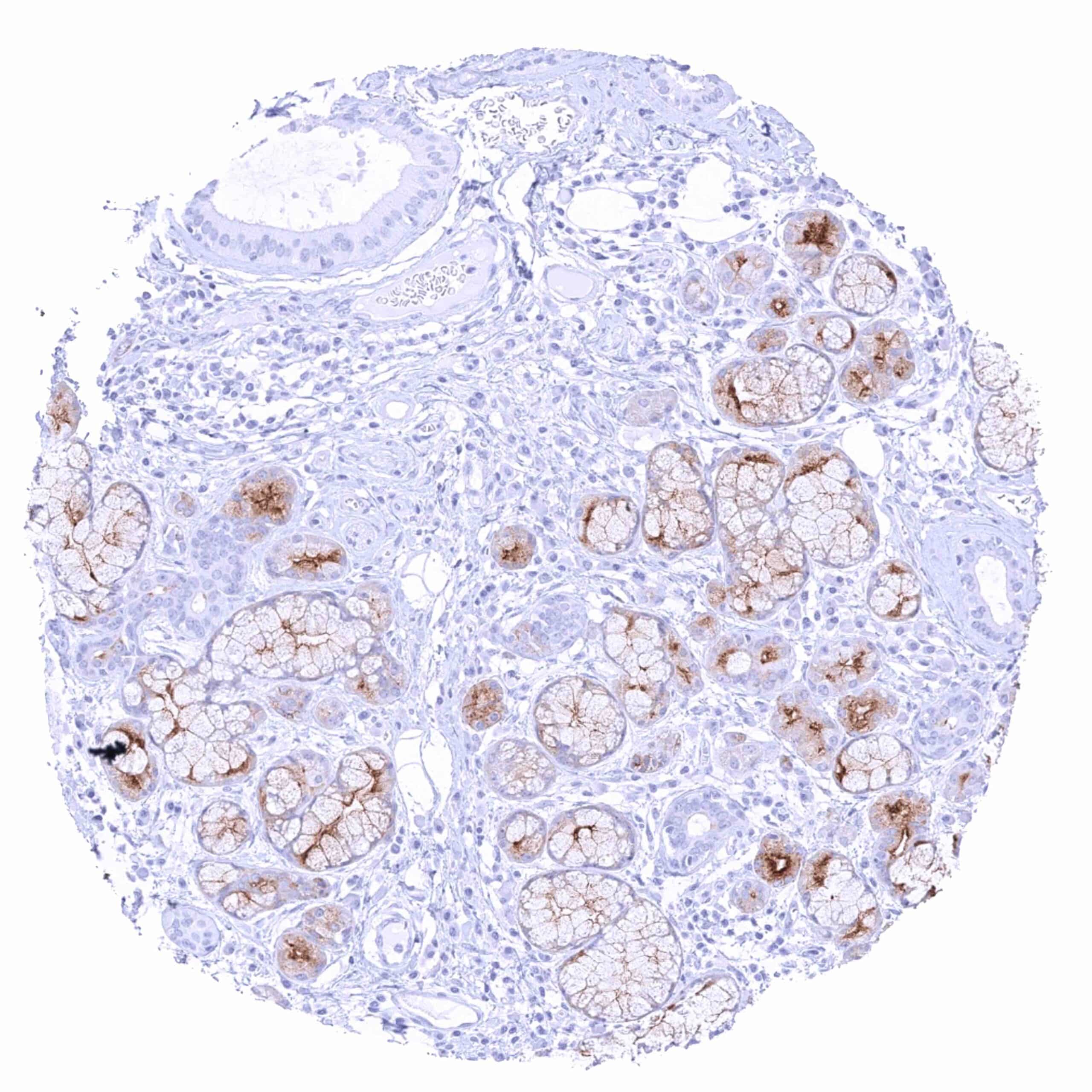
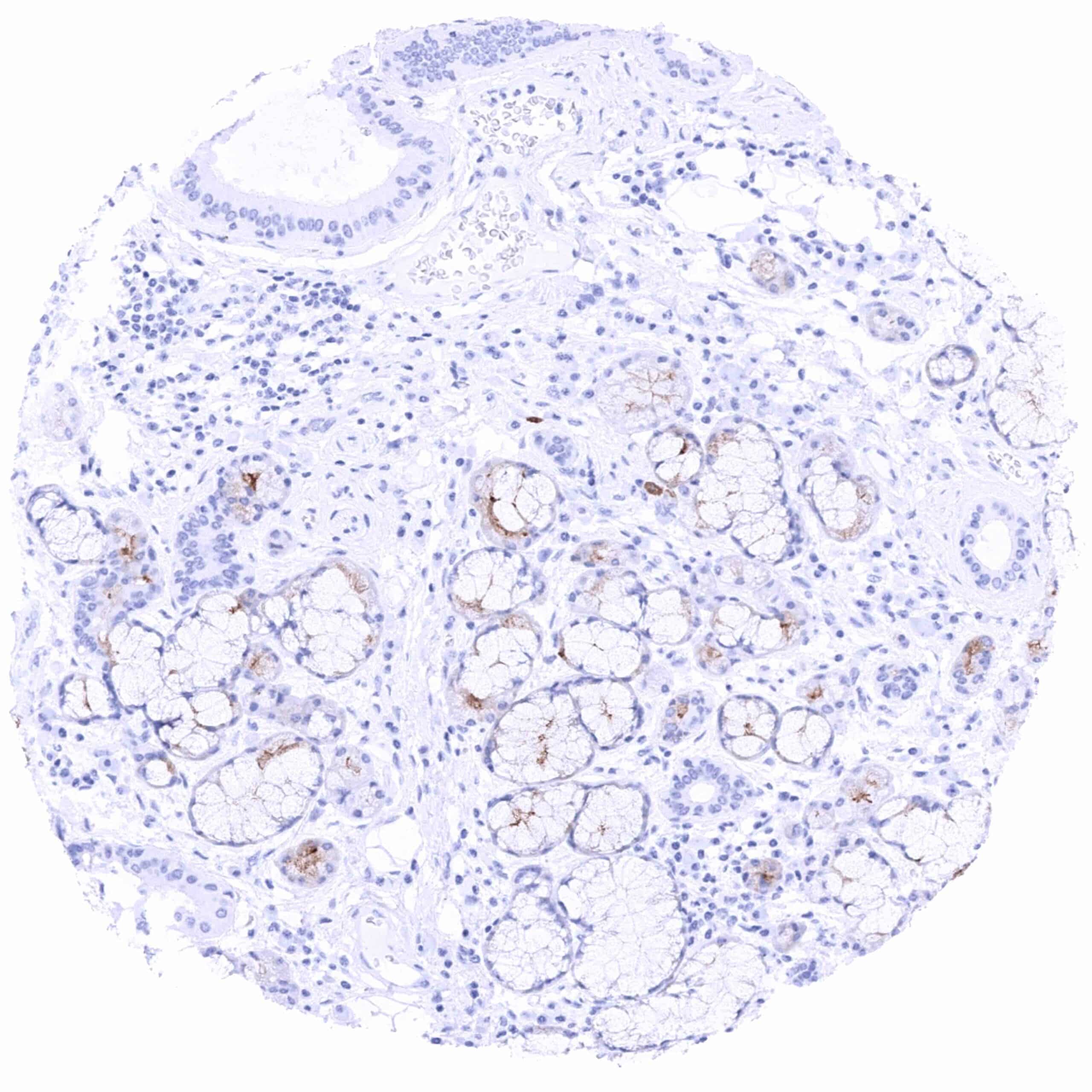
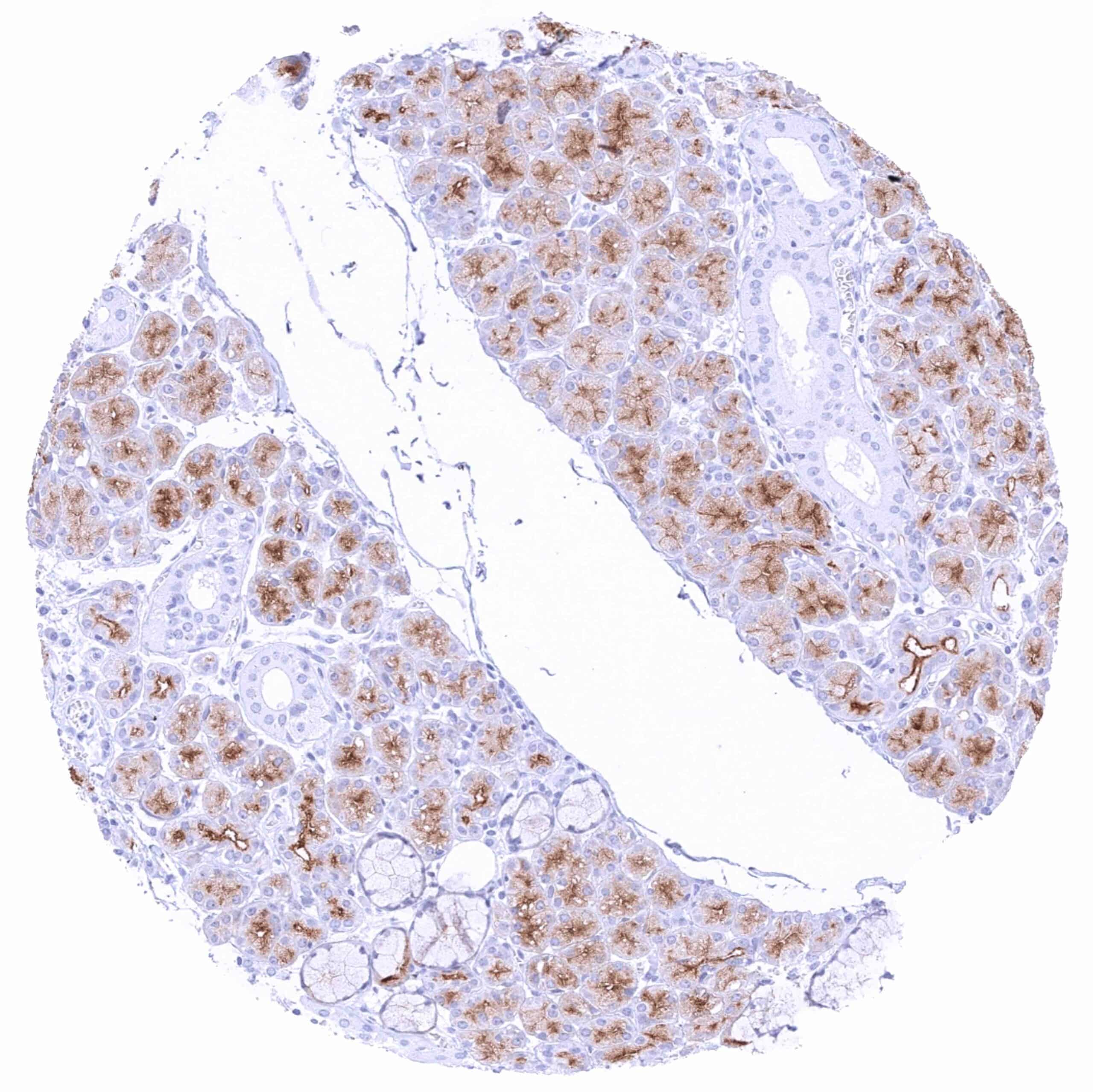
| Gastrointestinal Tract | Salivary glands | Strong apical membranous and weak to moderate diffuse cytoplasmic PSMA staining of serous (and to a lesser extent mucinous) glands. |
| Esophagus | Negative. | |
| Stomach | Negative. | |
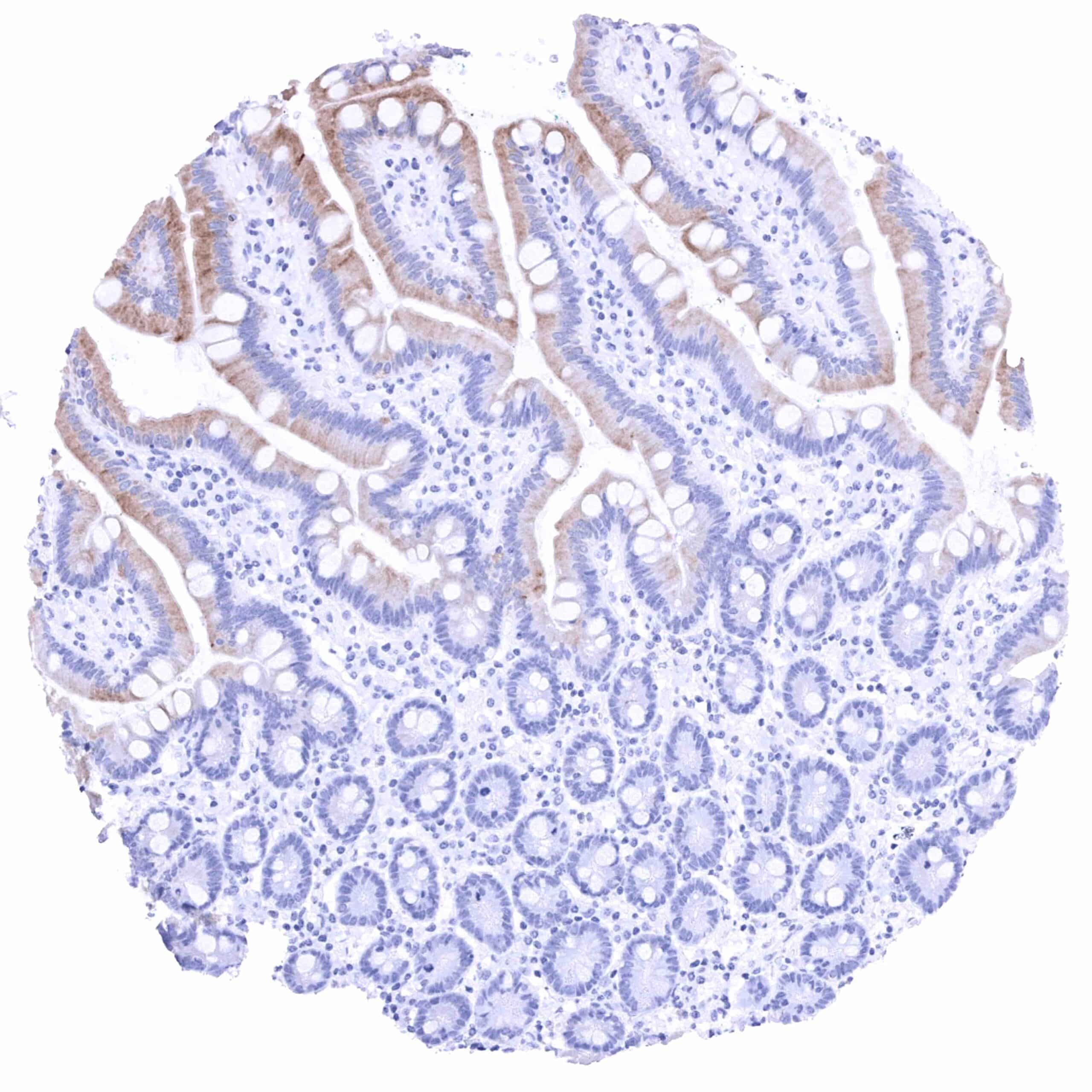
| Duodenum | Intense PSMA staining of the luminal membranes – more intense on villi than in crypts. The cytoplasm is also PSMA positive especially its luminal half. A weak PSMA staining, predominantly at the apical membrane, can also be seen in Brunner glands, especially in areas which are close to the surface. | |
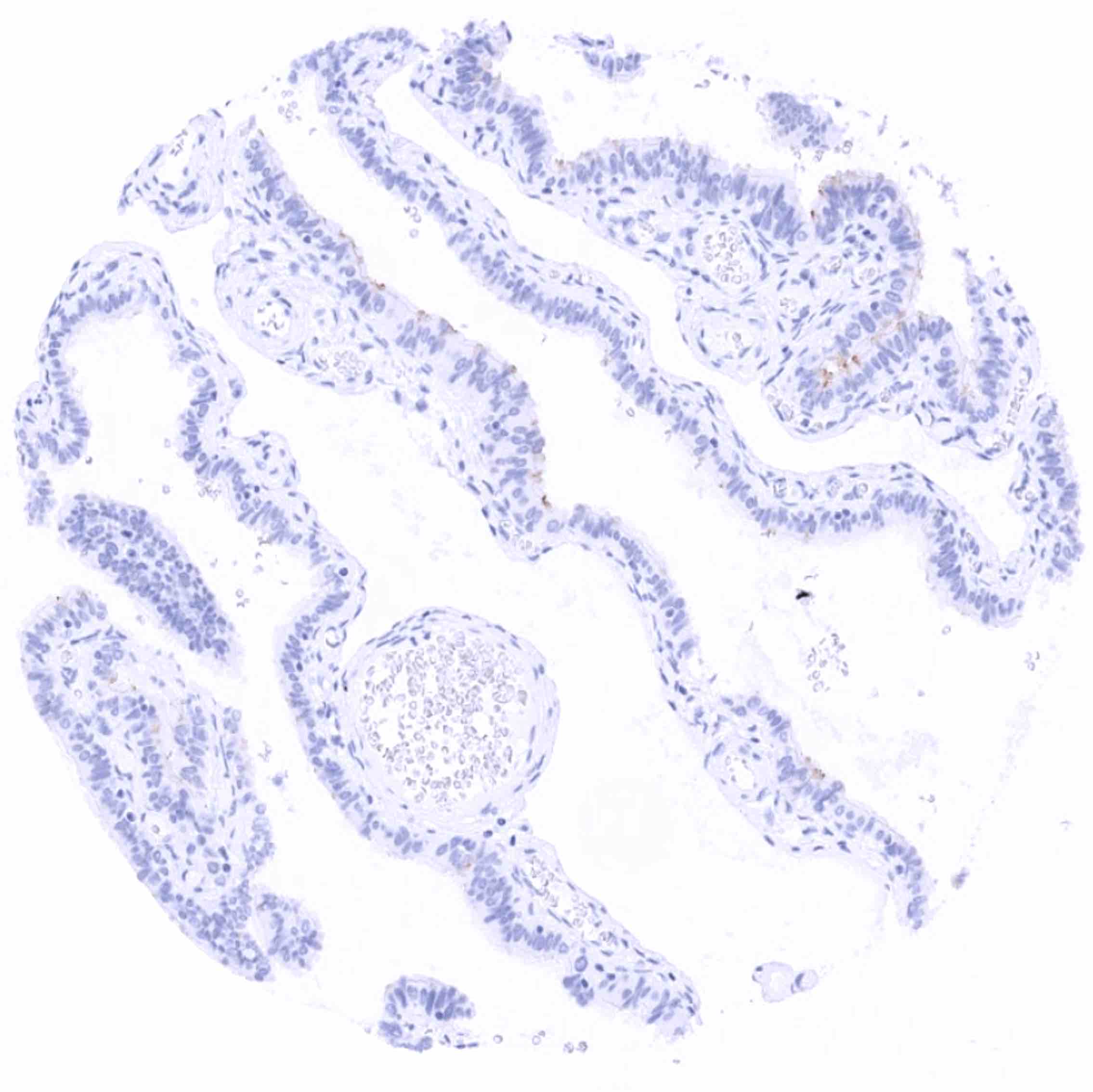
| Small intestine | Weak PSMA staining of the luminal membranes on the surface of villi while it is absent in crypts. | |
| Appendix | Negative. | |
| Colon | Negative. | |
| Rectum | Negative. | |
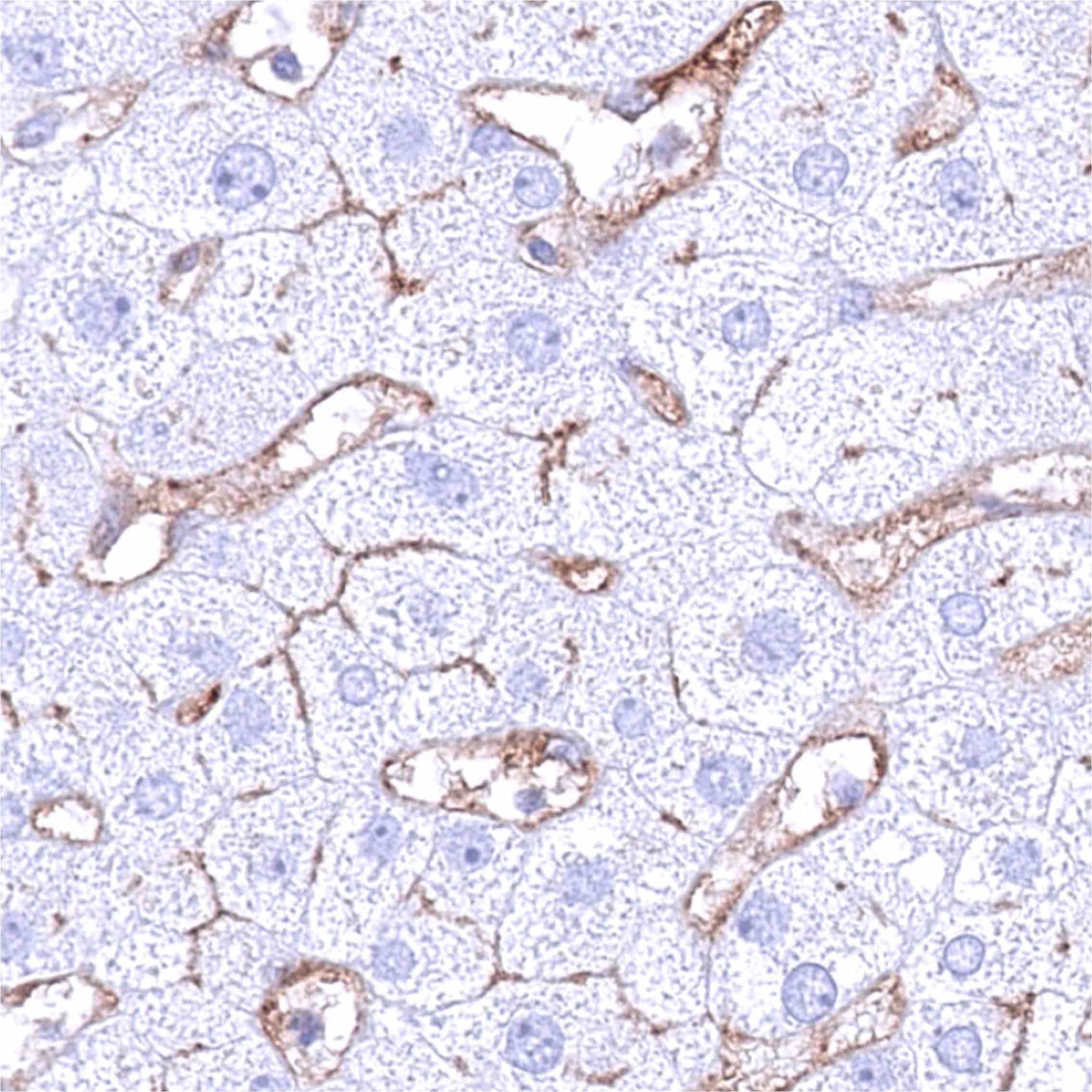
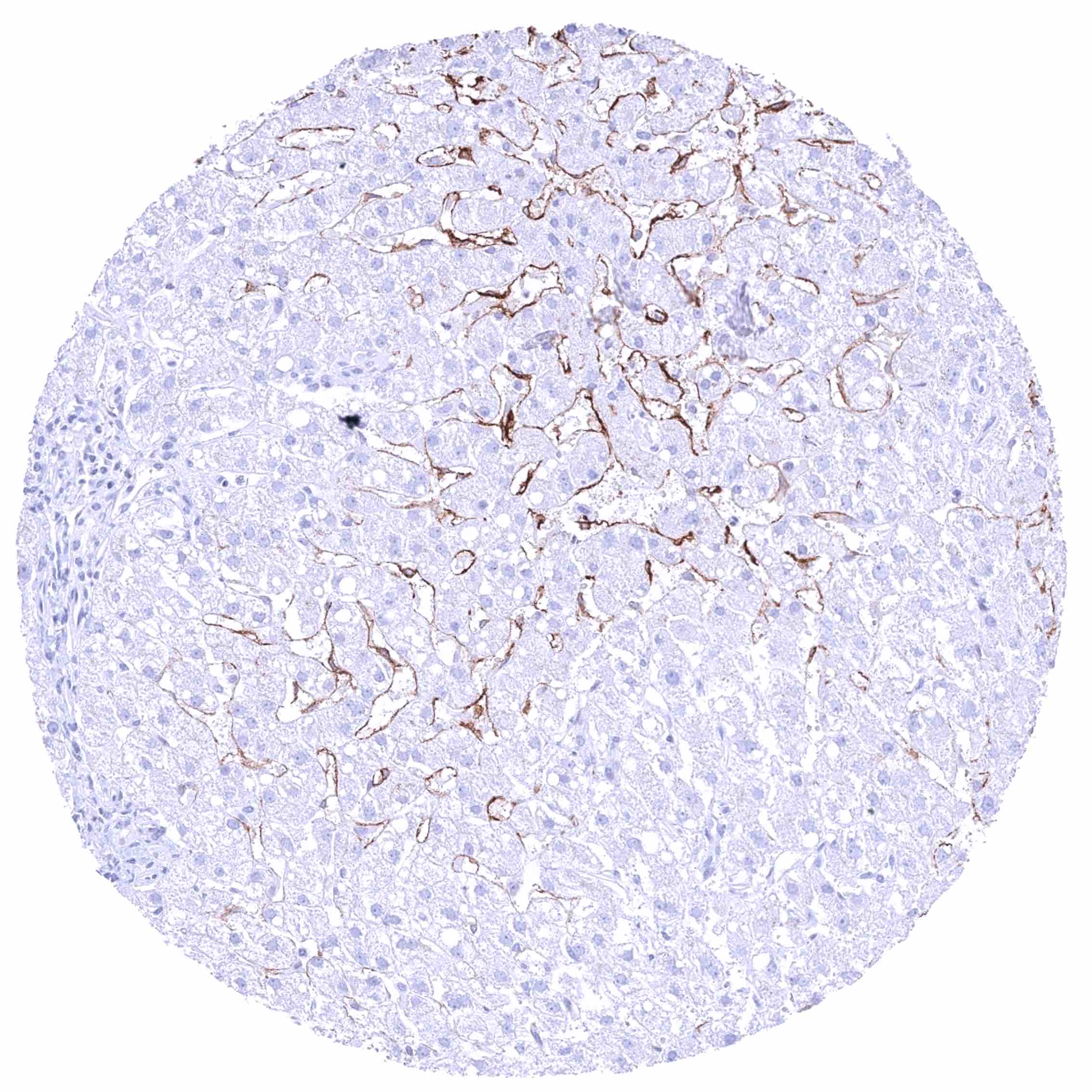
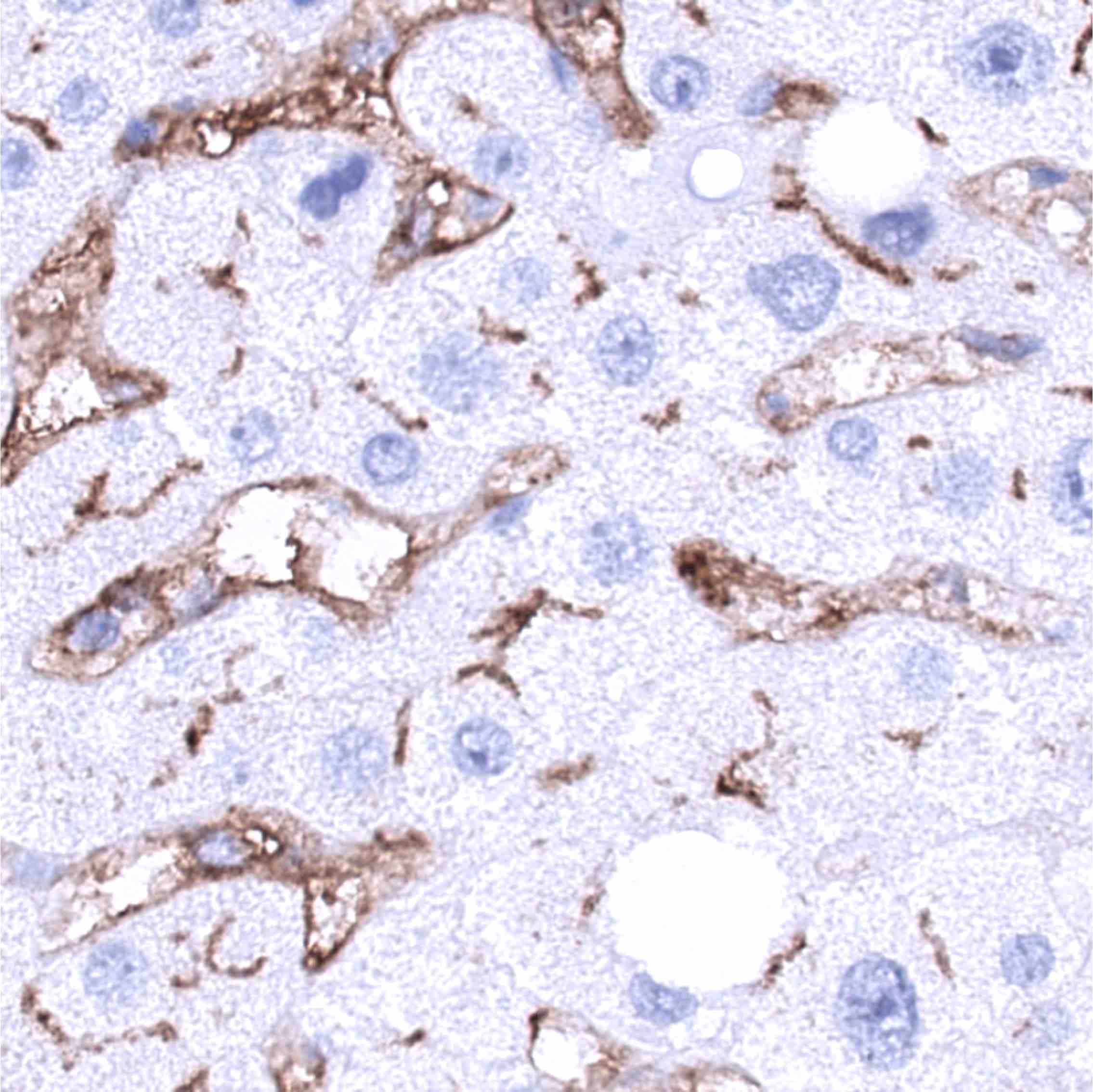
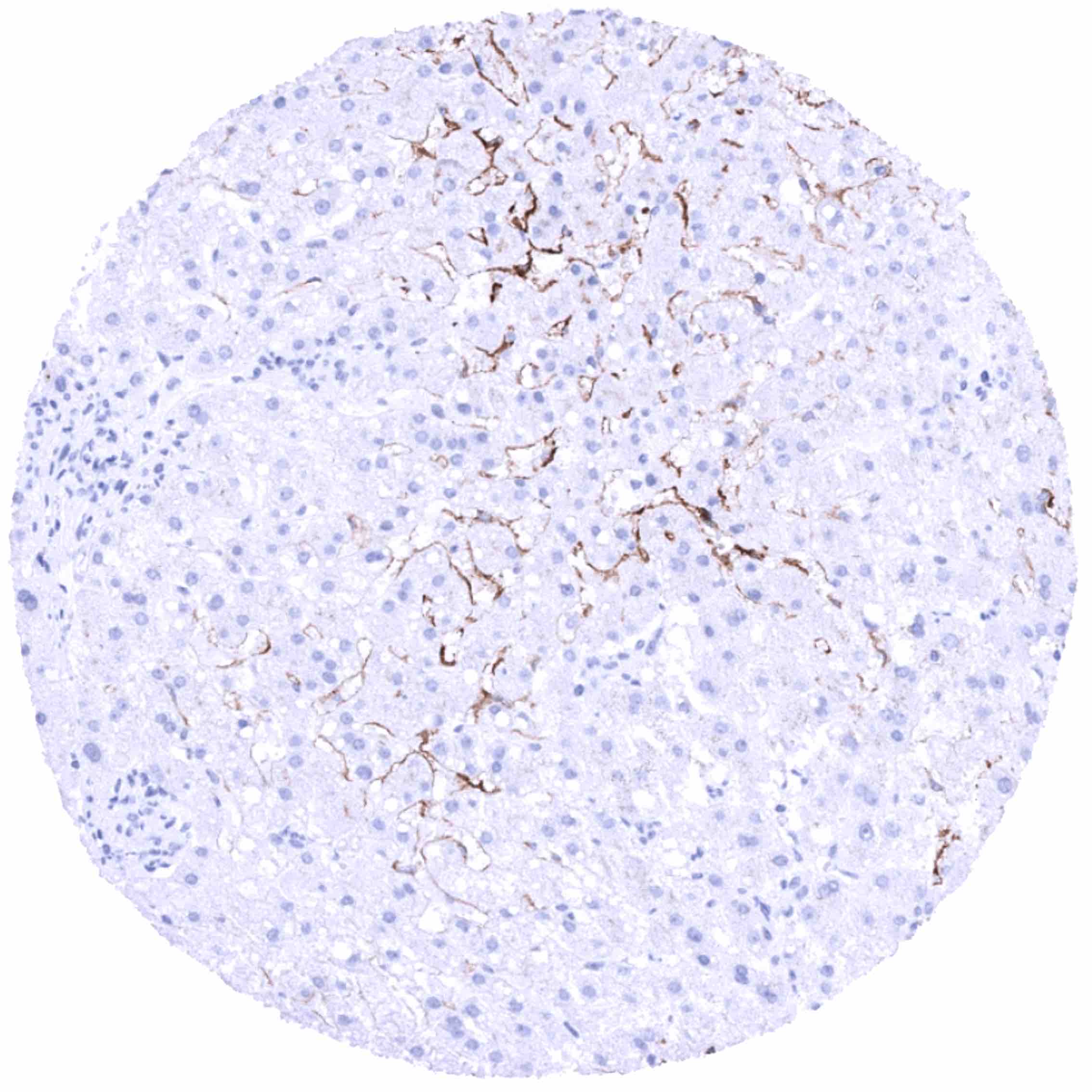
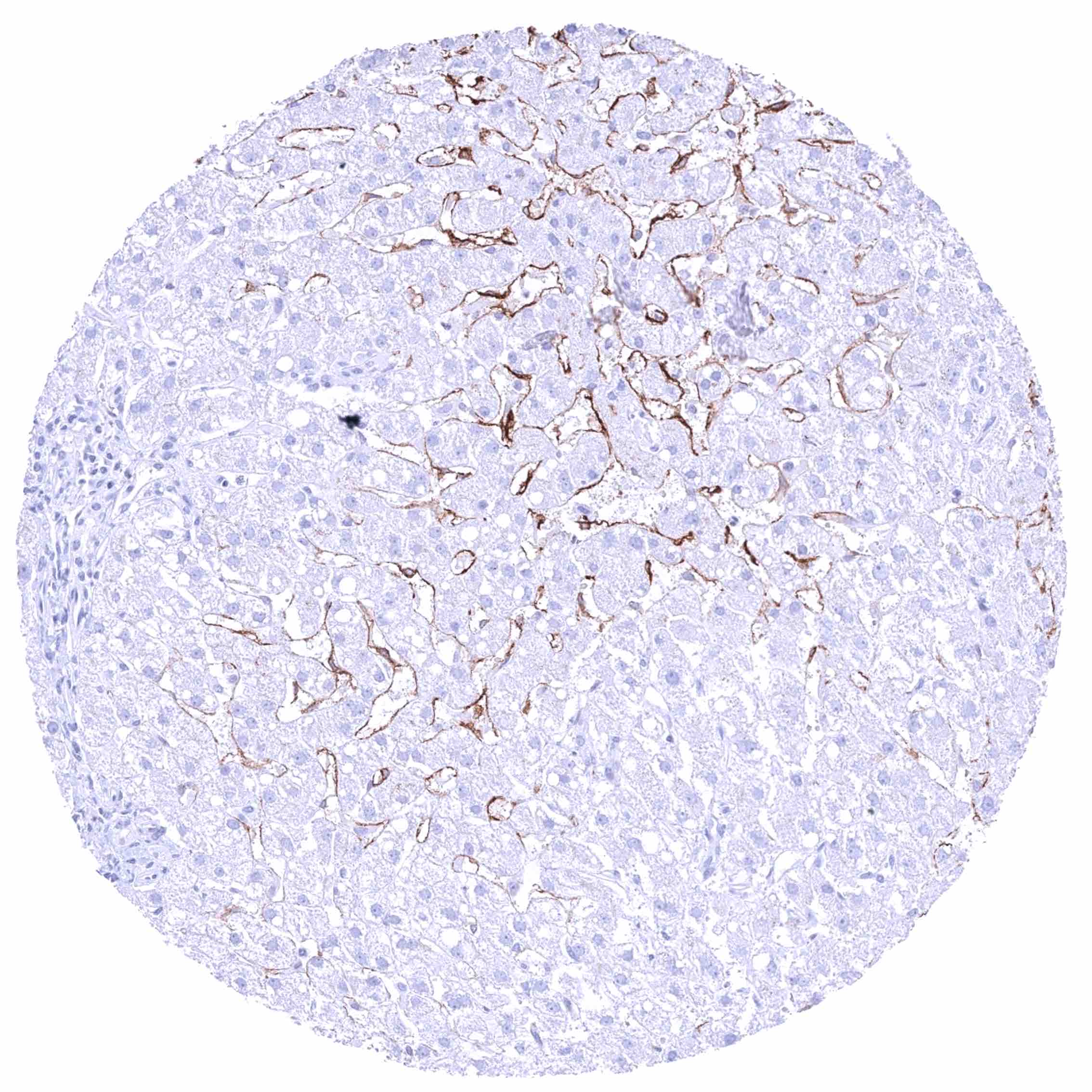
| Liver | Moderate to strong PSMA staining of sinusoid cells (regional differences in the staining intensity). An additional weak to moderate membranous PSMA staining of hepatocytes (especially at the bile secreting pole) is seen in some samples. | |
| Gallbladder | Weak to moderate PSMA staining of the apical membranes of epithelial cells. | |
| Pancreas | Negative. | |
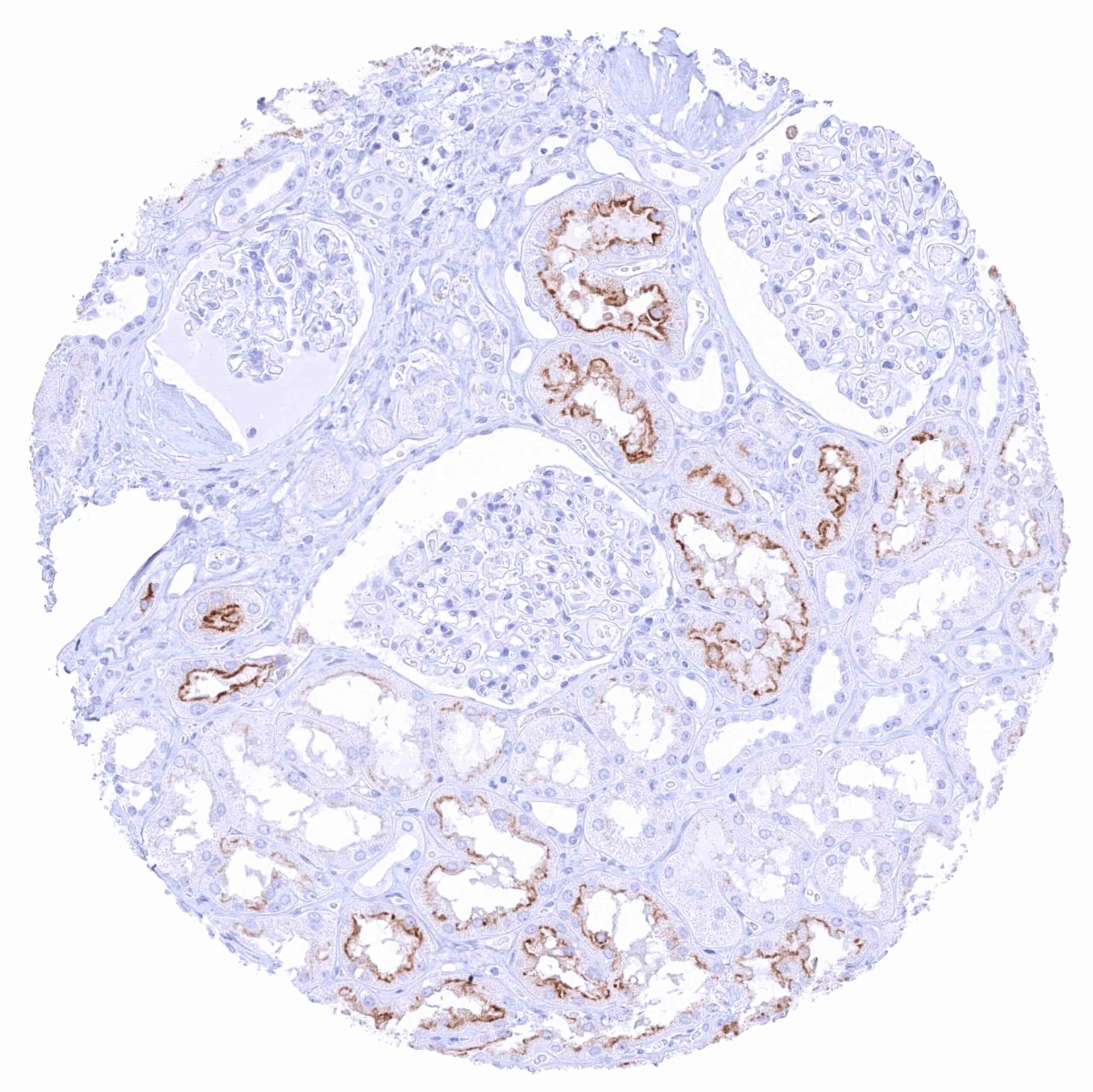
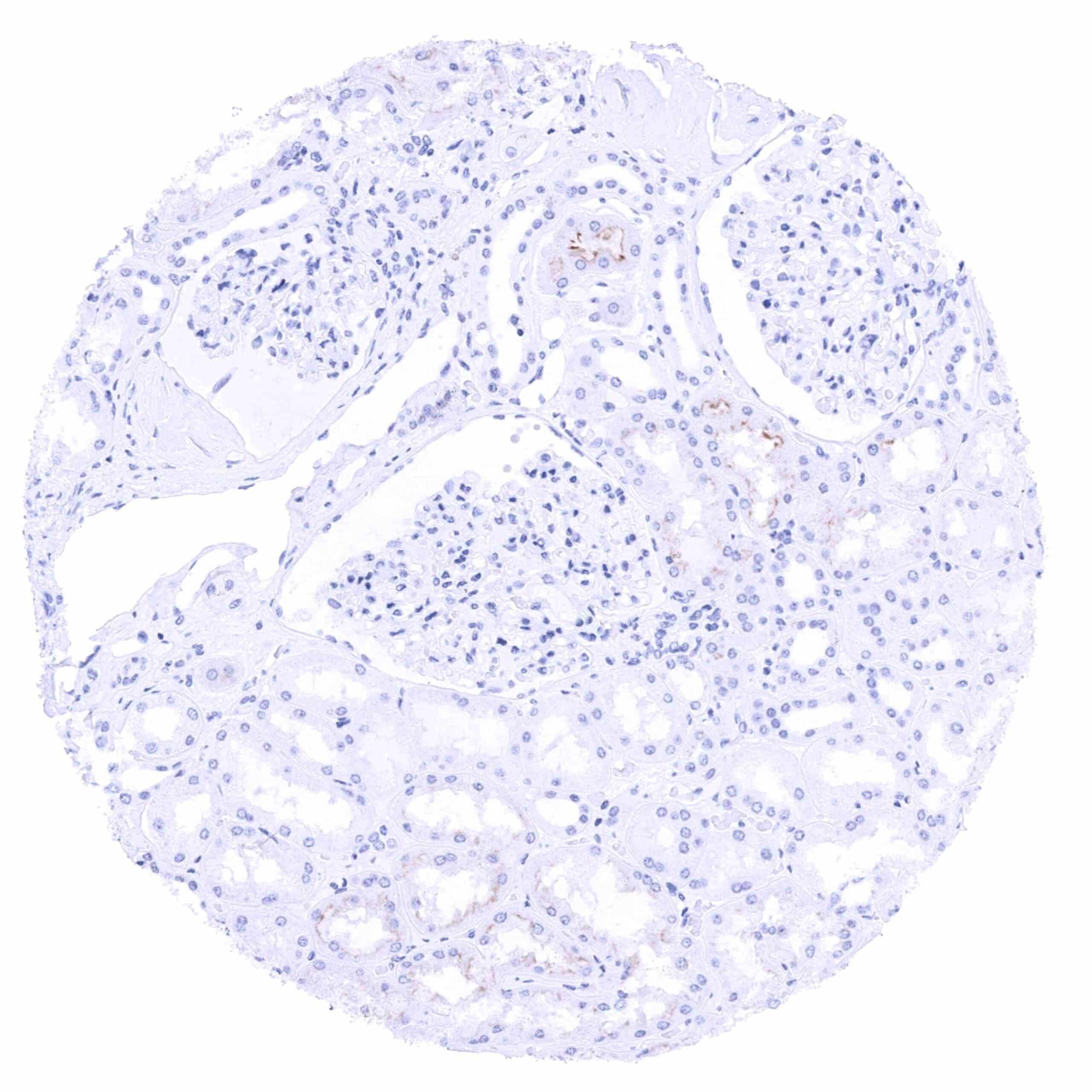
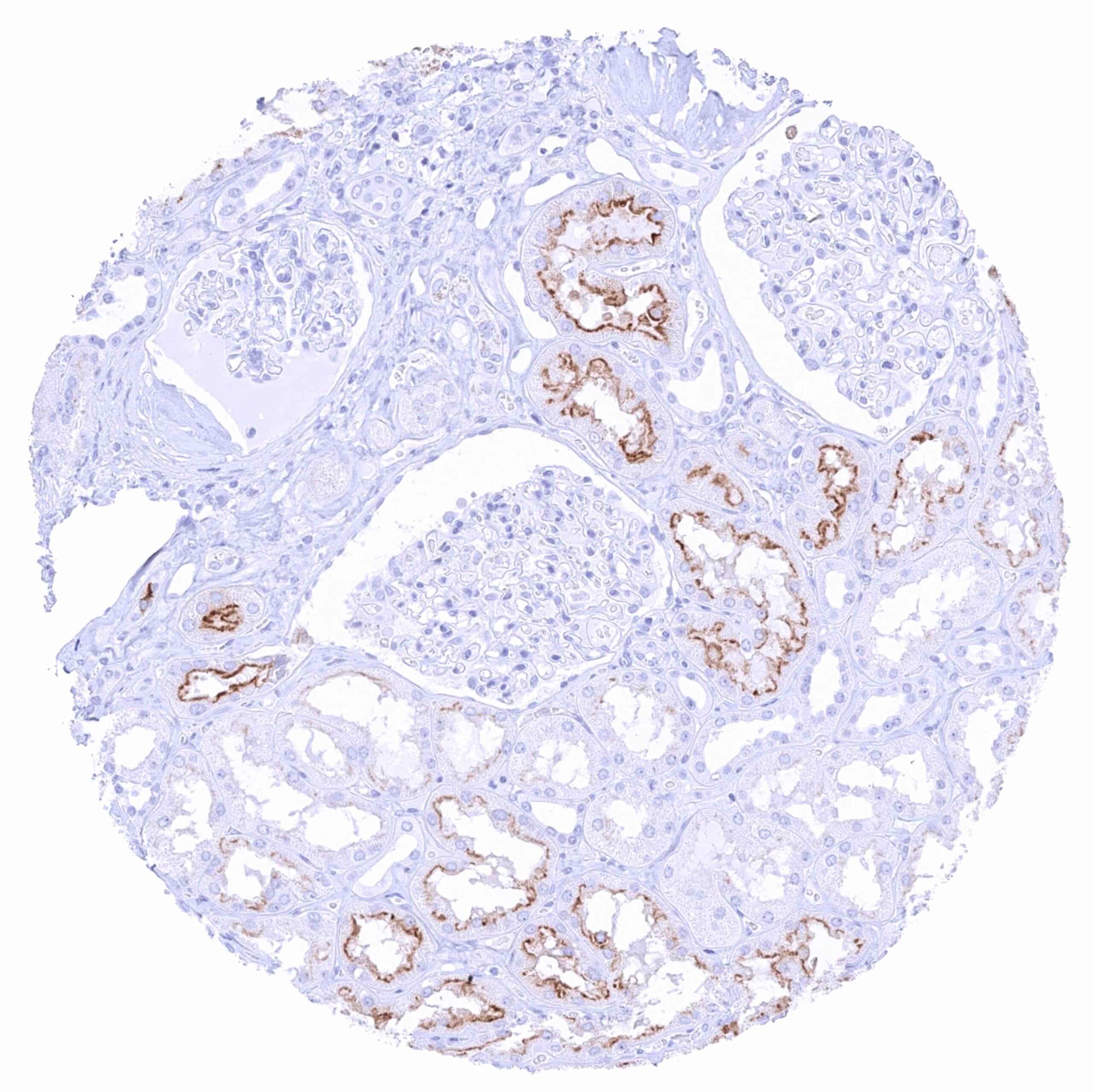
| Genitourinary | Kidney | Intense PSMA staining of luminal membranes of proximal tubules while staining is markedly less intense in distal tubuli and absent in collecting ducts. |
| Urothelium | Negative. | |
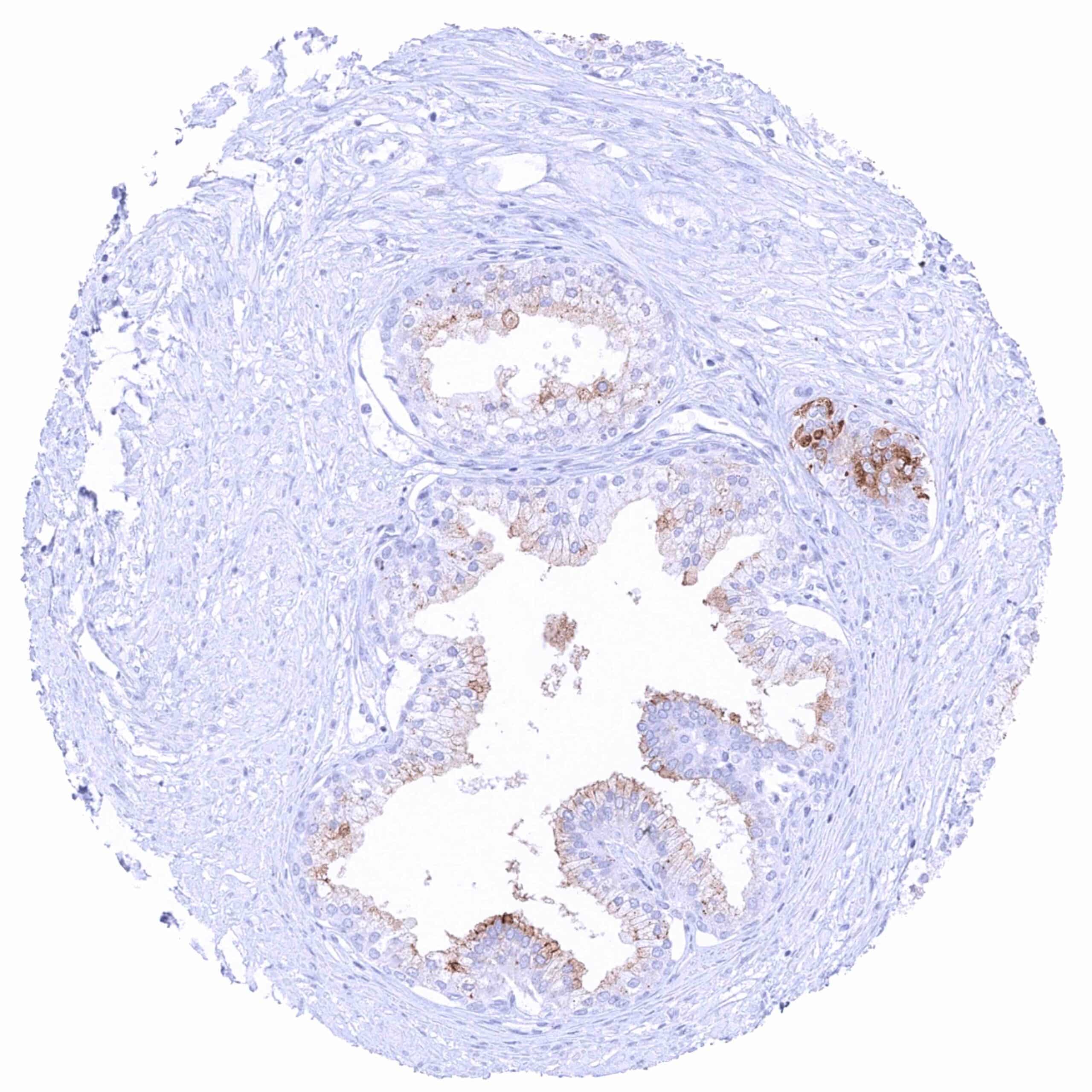
| Male genital | Prostate | Intense cytoplasmatic (and also membranous; apical) PSMA staining of most luminal cells in most samples. There are also samples with low staining intensity in only few cells. |
| Seminal vesicles | Negative. | |
| Testis | Negative. | |
| Epididymis | A weak to moderate apical membranous PSMA staining can focally occur in the cauda epididymis. | |
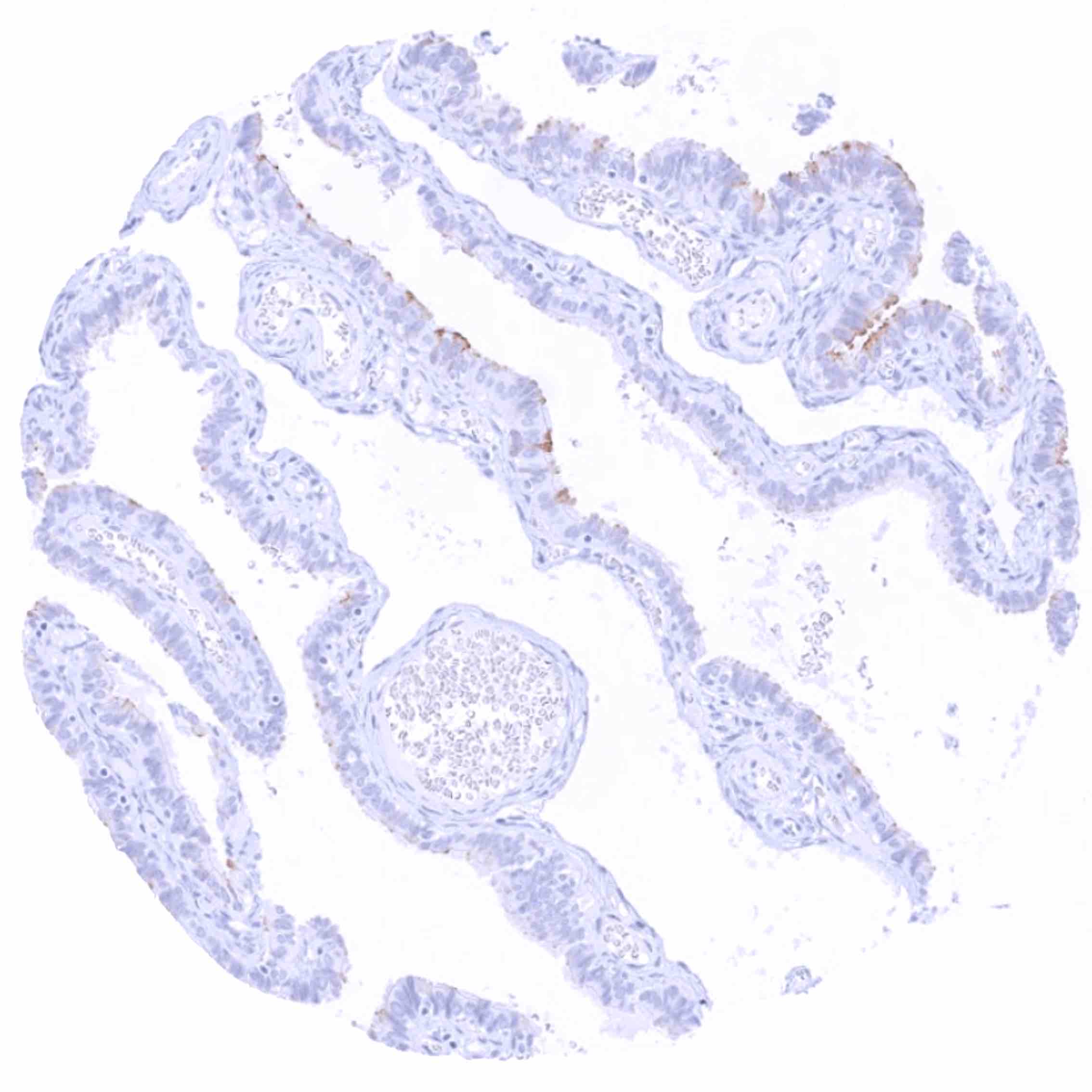
| Female genital | Breast | Weak to moderate apical membranous and faint cytoplasmic PSMA staining of luminal glandular cells. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Negative. | |
| Uterus endocervix | Negative. | |
| Uterus, endometrium | A weak apical membranous (and faint cytoplasmic) PSMA staining of epithelial cells can occur. | |
| Fallopian Tube | Weak to moderate apical membranous and weak cytoplasmic PSMA staining of a subset of epithelial cells. | |
| Ovary | Negative. | |
| Placenta early | Negative. | |
| Placenta mature | Negative. | |
| Amnion | ||
| Chorion | Negative. | |
| Skin | Epidermis | Negative. |
| Sebaceous glands | Negative. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
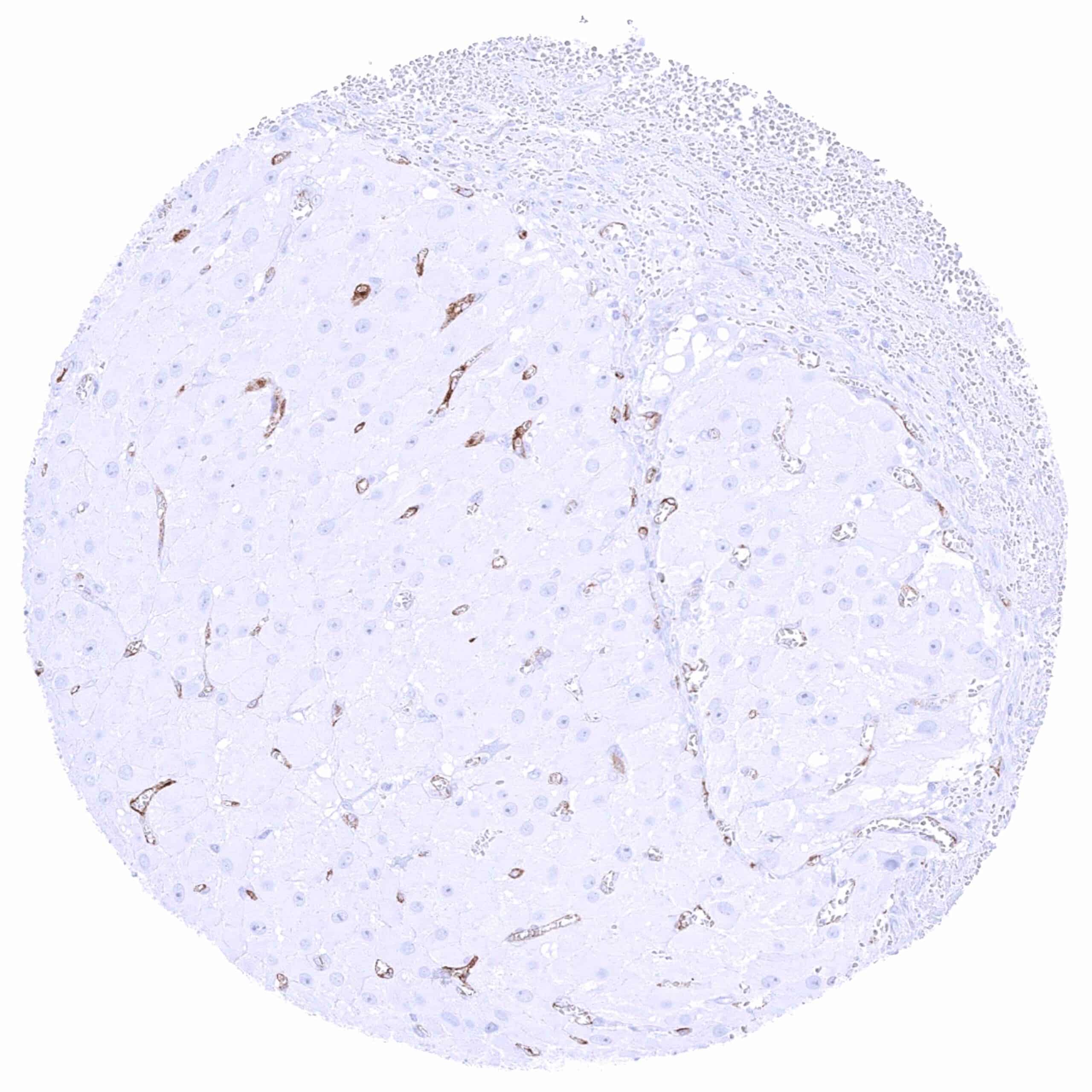
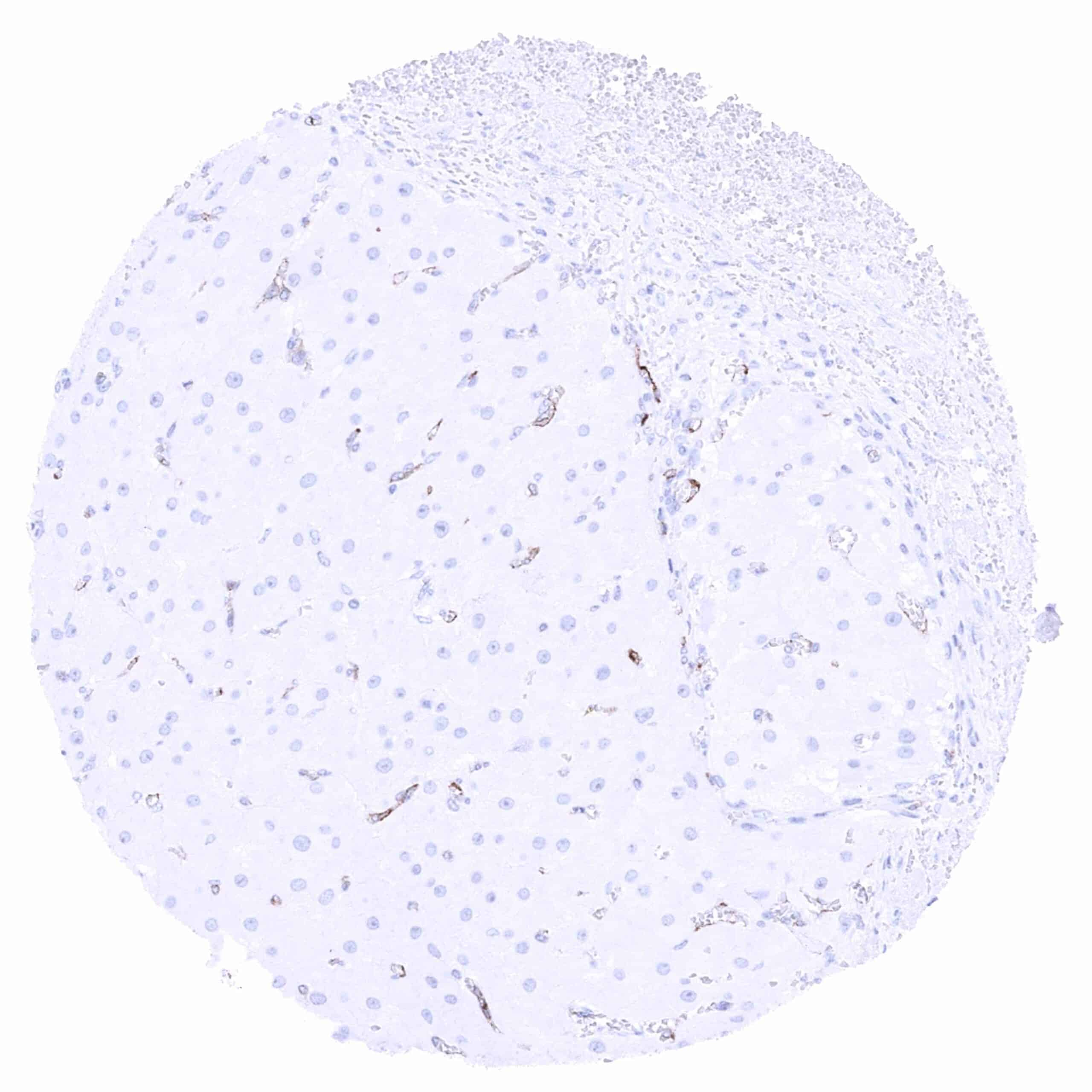
| Endothelium | PSMA positivity of variable intensity occurs in endothelial cells of many different tissues. | |
| Bone marrow/ lymphoid tissue | Bone marrow | Negative. |
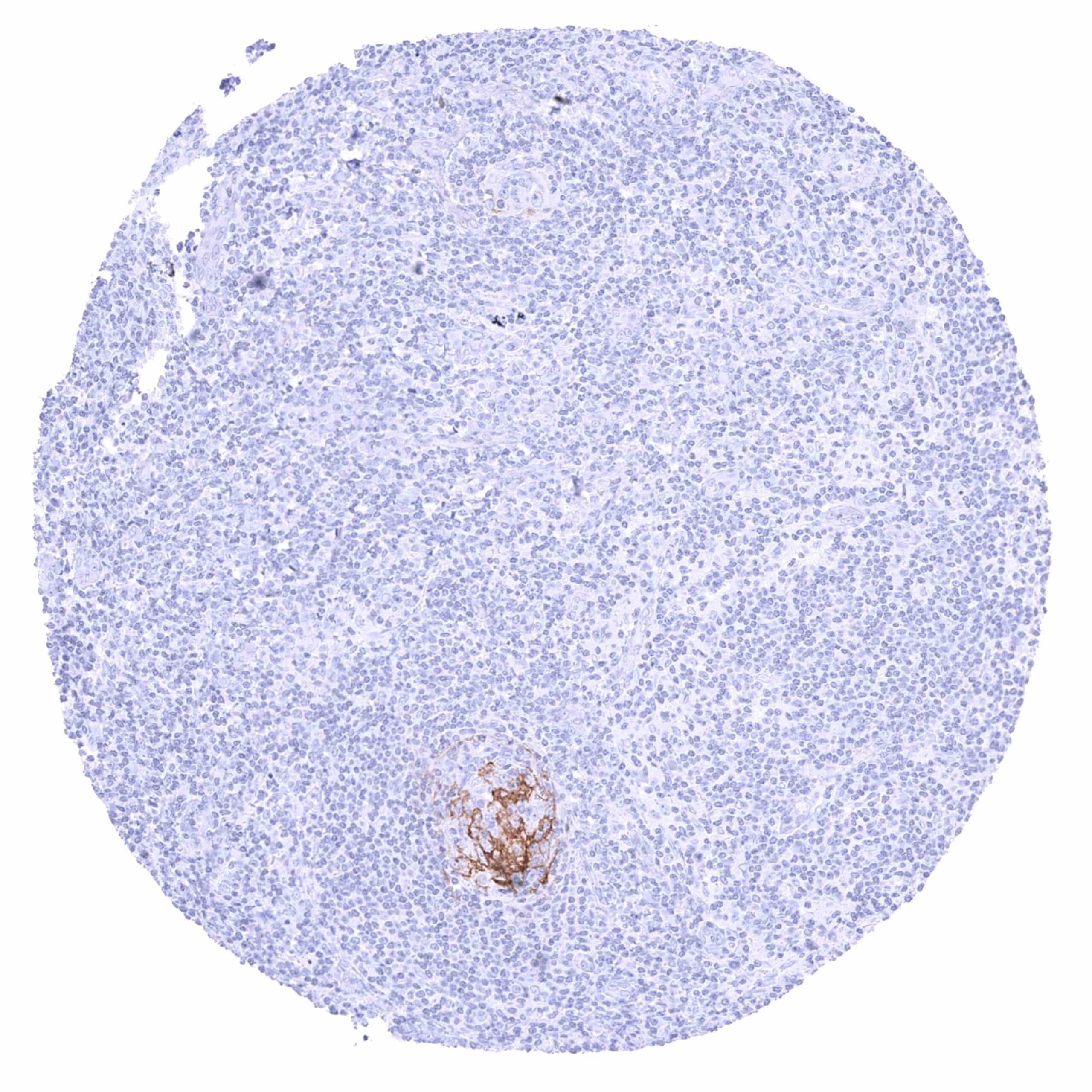
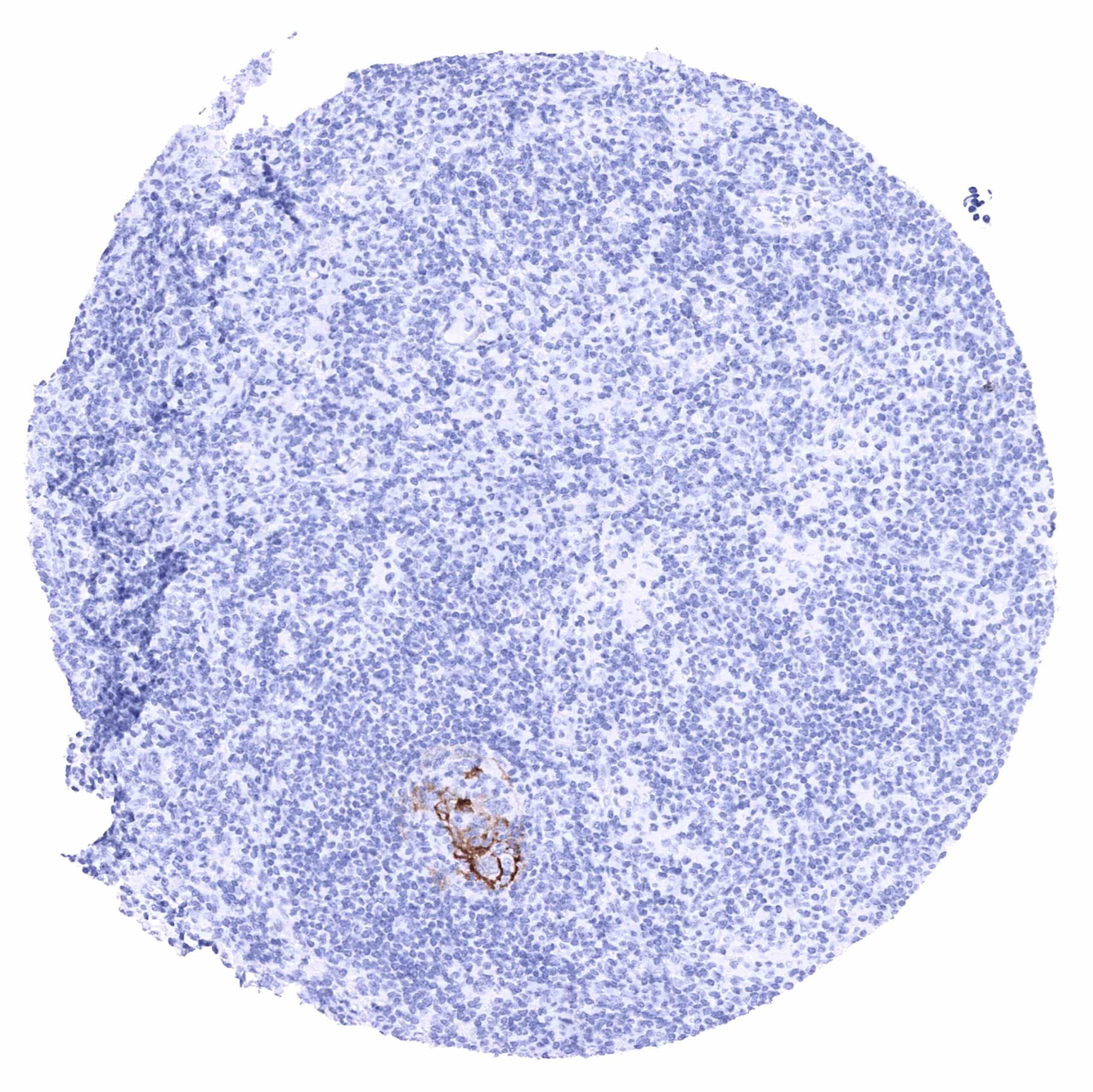
| Lymph node | A distinct membranous PSMA staining can occur in groups of germinal centre cells. Lymphocytes are PSMA negative. | |
| Spleen | Distinct PSMA staining of venous sinuses (littoral cells). | |
| Thymus | Negative. | |
| Tonsil | A distinct membranous PSMA staining can occur in groups of germinal centre cells. Lymphocytes are PSMA negative. | |
| Remarks |
These findings are largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression PSMA) where a rather ubiquitous expression is described (endothelial cells occur in all tissues).
Positive control = Prostate: A moderate to strong PSMA staining should be seen in the cytoplasm and at the apical/luminal membrane of acinar epithelial cells.
Negative control = Colon: PSMA staining must be completely absent in all cell types.
Staining Pattern in Relevant Tumor Types
PSMA expression predominates in prostatic cancers but it can also occur in other cancer types. PSMA staining is particularly frequent in blood vessels of the cancer stroma.
The TCGA findings on PSMA RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply ARX-752 at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The prevalence and clinical significance of PSMA expression in tumor cells and the neo-vasculature in different cancer types is insufficiently explored.
- The best use of PSMA as a therapeutic target has not been finally determined in prostate cancer and other tumor types.
- The role and utility as a drug target of PSMA is unclear in neurological disease.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody ARX-752 specificity is supported by the near complete concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the human protein atlas (https://www.proteinatlas.org/ENSG00000086205-FOLH1/tissue). In line with these RNA data, IHC staining by ARX-752 revealed positivity in all organs with documented RNA expression. Moreover, IHC by ARX-752 resulted in the highest levels of IHC staining in organs with highest RNA levels (prostate, duodenum, small intestine, salivary glands), detected positive cell types in all organs with low level RNA expression (brain, gallbladder) and even in organs where only traces of PSMA RNA had been detected (breast, spleen, fallopian tube). IHC staining of some endometrium glands, few cells in the cauda epididymis, and of few grouped cells in germinal centres of lymph nodes were the only IHC findings that were not corroborated by RNA data. It is assumed that these RNAs remained undetected because the number of PSMA producing cells was too low as compared to the entirety of cells of the respective organs.
Comparison of antibodies: True expression of PSMA in cell types with documented PSMA immunostaining by ARX-752 is validated by identical staining patterns obtained by a second, independent PSMA antibody, termed “validation antibody” for all cell types found to be positive by ARX-752. The successful validation also included all positive cell types observed in endometrium, cauda epididymis, and in germinal centres of lymph nodes