


295,00 € – 1.495,00 €
Product details
Synonyms = lysine demethylase 6A , KABUK2 , UTX , bA386N14.2
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = HMV311
Positive control = Testis: A strong KDM6A staining should be seen in Sertoli cells, Leydig cells and in immature cells of the spermatogenesis (spermatogonia).
Negative control = Testis: KDM6A staining must be absent in mature cells of the spermatogenesis (spermatocytes, spermatids).
Cellular localization = Intracellular
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
KDM6A is an Important enzyme for differentiation of embryonic stem cells and development of various tissues.
Recently presented poster at the ECP Annual Meeting in Florence September 7-11th 2024 by Florian Viehweger.
“KDM6A expression loss is a common feature in low-grade non-invasive urothelial carcinomas of the urinary bladder.”
Biology Behind
The lysine-specific demethylase 6A (KDM6A), also termed “Ubiquitously transcribed tetratricopeptide repeat on chromosome X” (UTX) is a 154 kDa protein coded by the KDM6A gene on chromosome Xp11.3. The gene is 5,438 bp long and contains 29 exons. It belongs to a family of Jumonji (JmjC) domain-containing enzymes which impact the demethylation of H3K27me2/3. H3K27me2/3 indicates the 27th amino acid on histone H3 which is known to represent a repressive histone modification. KDM6A regulates the transcription and expression of downstream genes, thereby regulating cell fate and functional cell characteristics. Depending on the molecular context, KDM6A can either promote or suppress cell growth. In evolving tissues, KDM6A is implicated in myogenesis, cardiac development, pancreas development, neural stem cell differentiation and immune cell functions. KDM6A is often mutated in various cancer types including bladder cancer, plasmacytoma, renal cell carcinoma, prostate cancer, and others. Mutations of KDM6A are a cause for Kabuki syndrome, a rare congenital anomaly syndrome characterized by intellectual disability, growth retardation, and multiple congenital abnormalities.
Staining Pattern in Normal Tissues
In normal tissues, Nuclear KDM6A staining is rather ubiquitous and only varies in intensity between tissues. Staining is less intense in fat cells, amnion cells, glandular cells of the stomach, hepatocytes, and a subset of renal tubuli. In squamous epithelium, KDM6A staining intensity tends to decrease from the basal to the superficial cell layers. In colorectal epithelium, KDM6A staining intensity tends to decrease from the crypt base to the superficial epithelial cell layers. Maturing testicular cells of the spermatogenesis are the only cell types with a complete lack of KDM6A staining. Images describing the KDM6A staining pattern in normal tissues obtained by the antibody HMV311 are shown in our “Normal Tissue Gallery”.
| Brain | Cerebrum | |
| Cerebellum | ||
| Endocrine Tissues | Thyroid | Moderate to strong nuclear KDM6A staining of follicular epithelial cells. |
| Parathyroid | Moderate to strong nuclear KDM6A staining of epithelial cells. | |
| Adrenal gland | Moderate to strong nuclear KDM6A staining of adrenocortical cells. | |
| Pituitary gland | Moderate to strong nuclear KDM6A staining of epithelial cells of the adenohypophysis.Faint nuclear KDM6A staining of pituicytes in the neurohypophysis. | |
| Respiratory system | Respiratory epithelium | Moderate to strong nuclear KDM6A staining of respiratory epithelial cells. |
| Lung | Moderate to strong nuclear KDM6A staining of all cell types. | |
| Gastrointestinal Tract | Salivary glands | Moderate to strong nuclear KDM6A staining of all epithelial cells. |
| Esophagus | Strong nuclear KDM6A staining of squamous epithelial cells. Staining is more intense in the lower than in the upper cell layers. | |
| Stomach | Moderate to strong nuclear KDM6A staining of epithelial cells. The staining is weaker in glandular cells than in superficial epithelium. | |
| Duodenum | Moderate to strong nuclear KDM6A staining of epithelial and inflammatory cells as well as of Brunner gland cells. | |
| Small intestine | Moderate to strong nuclear KDM6A staining of epithelial and inflammatory cells. | |
| Appendix | Strong nuclear KDM6A staining of epithelial and inflammatory cells. | |
| Colon | Moderate to strong nuclear KDM6A staining of epithelial cells. Staining is more intense in the crypt base than in the superficial epithelial cell layers. | |
| Rectum | Moderate to strong nuclear KDM6A staining of epithelial cells. Staining is more intense in the crypt base than in the superficial epithelial cell layers. | |
| Liver | Weak to moderate nuclear KDM6A staining of hepatocytes. Stronger staining of other cell types. | |
| Gallbladder | Strong nuclear KDM6A staining of epithelial cells. | |
| Pancreas | Moderate to strong nuclear KDM6A staining of acinar cells. Stronger staining of ductal and islet cells. | |
| Genitourinary | Kidney | Weak to moderate nuclear KDM6A staining of tubular cells. Staining is more intense in collecting ducts. |
| Urothelium | Strong nuclear KDM6A staining of urothelial cells. | |
| Male genital | Prostate | Moderate nuclear KDM6A staining of all epithelial cells. |
| Seminal vesicles | Strong nuclear KDM6A staining of epithelial cells. | |
| Testis | Moderate to strong nuclear KDM6A staining of Sertoli cells. KDM6A staining is weak in spermatogonia and virtually absent in more mature cells of spermatogenesis. | |
| Epididymis | Moderate to strong nuclear KDM6A staining of epithelial cells of the caput and the cauda. Staining is less intense in basal cells. | |
| Female genital | Breast | Strong nuclear KDM6A staining of basal and luminal cells of breast glands. |
| Uterus, myometrium | Moderate to strong nuclear KDM6A staining of muscular cells. | |
| Uterus, ectocervix | Moderate to strong nuclear KDM6A staining of squamous epithelial cells. Staining is stronger in the lower than in the upper cell layers. | |
| Uterus endocervix | Strong nuclear KDM6A staining of epithelial cells. | |
| Uterus, endometrium | Strong nuclear KDM6A staining of epithelial and stromal cells although stroma cell staining is somewhat less intense. | |
| Fallopian Tube | Strong nuclear KDM6A staining of all epithelial cells. | |
| Ovary | Strong nuclear KDM6A staining of corpus luteum cells. Moderate nuclear KDM6A staining of stroma cells. | |
| Placenta early | Strong nuclear KDM6A staining of trophoblastic cells, stroma cells and endothelial cells. | |
| Placenta mature | Strong nuclear KDM6A staining of trophoblastic cells, stroma cells and endothelial cells. | |
| Amnion | Weak nuclear KDM6A staining of amnion cells. | |
| Chorion | Moderate to strong staining of chorion cells. | |
| Skin | Epidermis | Moderate to strong nuclear KDM6A staining of squamous epithelial cells. |
| Sebaceous glands | ||
| Muscle/connective tissue | Heart muscle | Weak to moderate KDM6A staining of a subset of heart muscle cells. |
| Skeletal muscle | Moderate nuclear KDM6A staining of myocytes. | |
| Smooth muscle | Weak to moderate nuclear KDM6A staining of muscular cells. | |
| Vessel walls | Weak nuclear KDM6A staining of some spindle-shaped cells. | |
| Fat | Faint nuclear KDM6A staining of some fat cells. | |
| Stroma | Weak to moderate nuclear KDM6A staining of all types of stroma cells is often seen. | |
| Endothelium | Weak to moderate nuclear KDM6A staining is often seen. | |
| Bone marrow/lymphoid tissue | Bone marrow | Intense nuclear KDM6A staining of virtually all cells. |
| Lymph node | Moderate to strong staining of lymphocytes and other cell types. | |
| Spleen | Moderate to strong staining of all cell types. | |
| Thymus | Intense nuclear KDM6A staining of all cell types. | |
| Tonsil | Strong nuclear KDM6A staining of squamous epithelial cells and of lymphocytes. | |
| Remarks | Nuclear KDM6A staining is rather ubiquitous and only varies in intensity between tissues. |
These findings are largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression KDM6A) which also suggest ubiquitous KDM6A expression.
Positive control = Testis: A strong KDM6A staining should be seen in Sertoli cells, Leydig cells and in immature cells of the spermatogenesis (spermatogonia).
Negative control = Testis: KDM6A staining must be absent in mature cells of the spermatogenesis (spermatocytes, spermatids).
Staining Pattern in Relevant Tumor Types
A KDM6A expression loss (indicating a truncating KDM6A mutation) primarily occurs in urothelial neoplasms but can also be seen in various other tumor entities. KDM6A expression at variable levels occurs in the vast majority of tumors.
The TCGA findings on KDM6A RNA expression in different tumor categories have been summarized in the Human Protein Atlas.



Compatibility of Antibodies
KDM6A (HMV311) publication summary
Relevant publication:
(1) Viehweger et al. “Prevalence of KDM6A deficiency in human cancer: A tissue microarray study on 18,570 cancers from 153 different tumor types“ Published in Virchows Archive 2026 Feb 17. Epub ahead of print. PMID: 41703255.;
A total of 14,814 tumors from 153 different tumor categories and another 2,125 urothelial cancers were successfully analyzed in the two studies by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. HMV311, at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
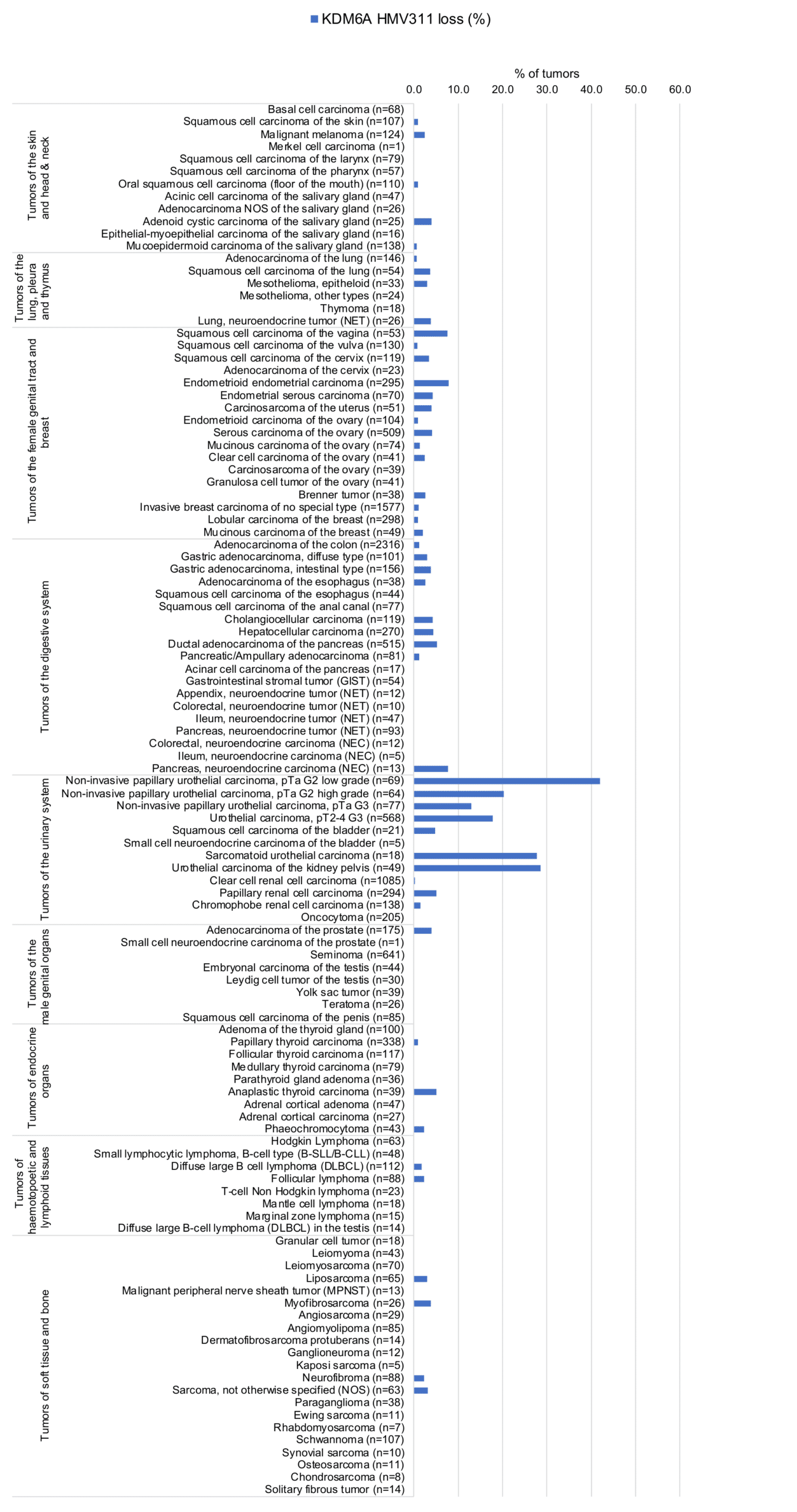
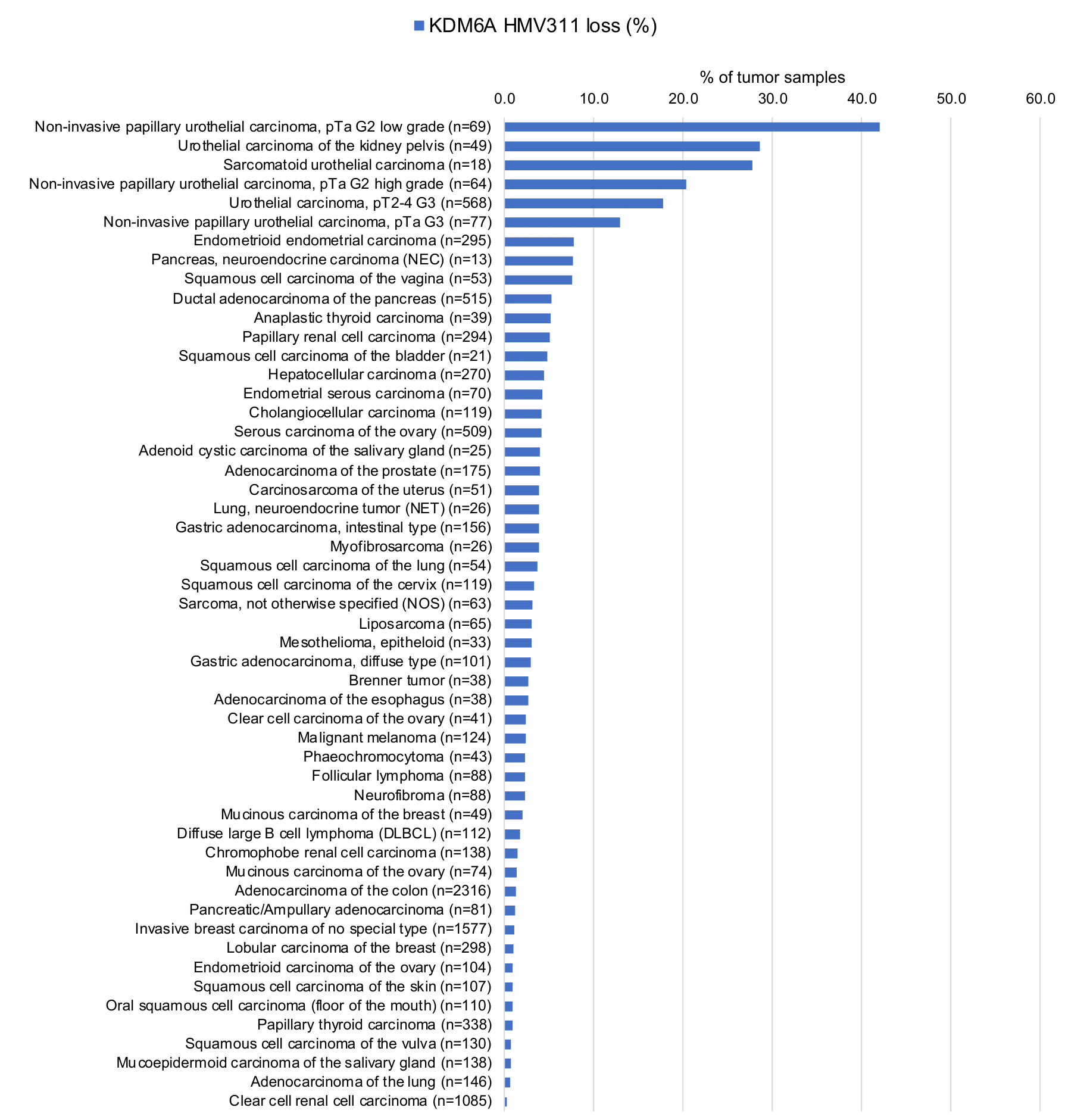
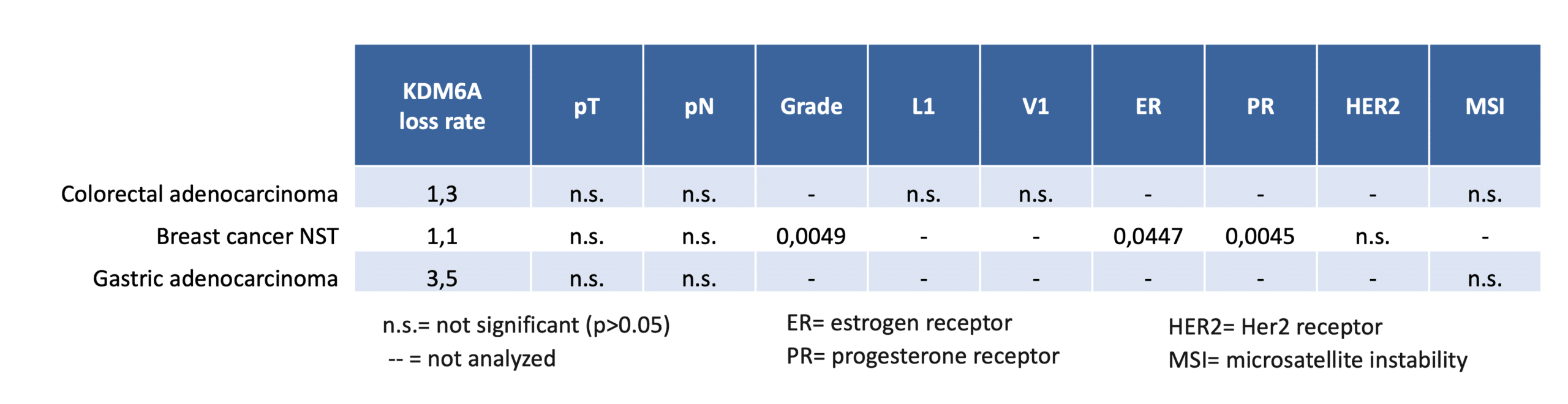
In 14,814 tumors, KDM6A deficiency was observed in 58 of 153 tumor categories, with the highest rates in urothelial carcinomas (17–24%). In other tumor types, prevalence was generally <10%, including gallbladder (9%), gastric (≤8%), pancreatic (8%), and prostatic adenocarcinomas (6%), as well as endometrial carcinomas and squamous cell carcinomas from various organs (≤8%). Frequencies were ≤5% in anaplastic thyroid carcinoma and papillary renal cell carcinoma, and ≤4% in hepatocellular carcinoma, melanoma, and high-grade serous ovarian carcinoma. KDM6A deficiency rates are shown in organ-systematic (Figure 1) and ranked (Figure 2) formats, with clinicopathological associations summarized in Figure 3 (based on Viehweger et al.).
Authors conclusions on the possible clinical role of KDM6A staining (Viehweger et al.):
- KDM6A IHC may be a useful tool for the distinction of neoplastic from non-neoplastic urothelial cells especially in the following situations:
- in follow-up examinations of patients with KDM6A deficient urothelial neoplasms.
- In urine cytology
- In flat urothelium suspicious for dysplasia
- Small or crushed biopsies
Authors conclusions on diagnostic utility of KDM6A IHC with respect to the distinction of different tumor entities (Viehweger et al.):
- Given that KDM6A deficiency strongly predominates in urothelial neoplasms but occurs at lower frequencies also in several other cancer entities, KDM6A IHC may have only limited utility for the discrimination of different tumor entities.
Authors conclusions on the prognostic role of KDM6A immunostaining results (Viehweger et al.):
- KDM6A deficiency was significantly associated with low grade and non-invasive tumor growth in urothelial carcinoma in our previous study on >2000 urothelial carcinomas of the urinary bladder (Viehweger et al.).
- A complete KDM6A loss (KDM6A deficiency) was associated with high grade (p=0.0049) as well as with ER and PR loss (p<0.05 each) in breast cancer of no special type in the present study (Viehweger et al.).
Data from the publication: “Prevalence of KDM6A deficiency in human cancer: A tissue microarray study on 18,570 cancers from 153 different tumor types“. Published by Viehweger et al. in Virchows Archive 2026 Feb 17. Epub ahead of print. PMID: 41703255. Summarized in own graphics:
1. KDM6A staining in tumors “organ-specific” with antibody HMV311
2. KDM6A staining in tumors “ranking order” by positivity with antibody HMV311
3. Table Clinico-pathological associations described by Viehweger et al. (p-value)
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply HMV311 at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- Loss of KDM6A staining is indicative for a truncating KDM6A mutation.
- The diagnostic and prognostic relevance of KDM6A expression in tumors and in preneoplastic disease needs to be investigated.
- Tumors with a KDM6A loss may be susceptible to treatment by EZH2 inhibitors.
- The function of KDM6A in cancer needs to be further studied.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody HMV311 specificity is supported by the good concordance of the immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression KDM6A). In agreement with HMV311 immunostaining data, KDM6A RNA expression occurs ubiquitously but is highest in the bone marrow and lymphoid tissues. However, orthogonal validation is not optimal for assessing ubiquitously expressed proteins.
Comparison of antibodies: True expression of KDM6A in all cell types with KDM6A positivity by HMV311 is corroborated by an identical staining obtained by a commercially available independent second antibody (termed “validation antibody”). Most of all, both antibodies showed an identical lack of KDM6A staining in maturing germ cells of the testis, and a continuous decrease of KDM6A staining intensity from basal to superficial cell layers in squamous epithelium, and from the crypt base to the superficial epithelial cell layers in the colorectal mucosa.




























