295,00 € – 995,00 €
Product details
Synonyms = Glutathione S-transferase P, GST class-pi, GSTP1-1, FAEES3, GST3, Glutathione S-transferase P, GST class-pi, EC:2.5.1.18,
Antibody type = Recombinant Rabbit monoclonal
Clone = MSVA-685R
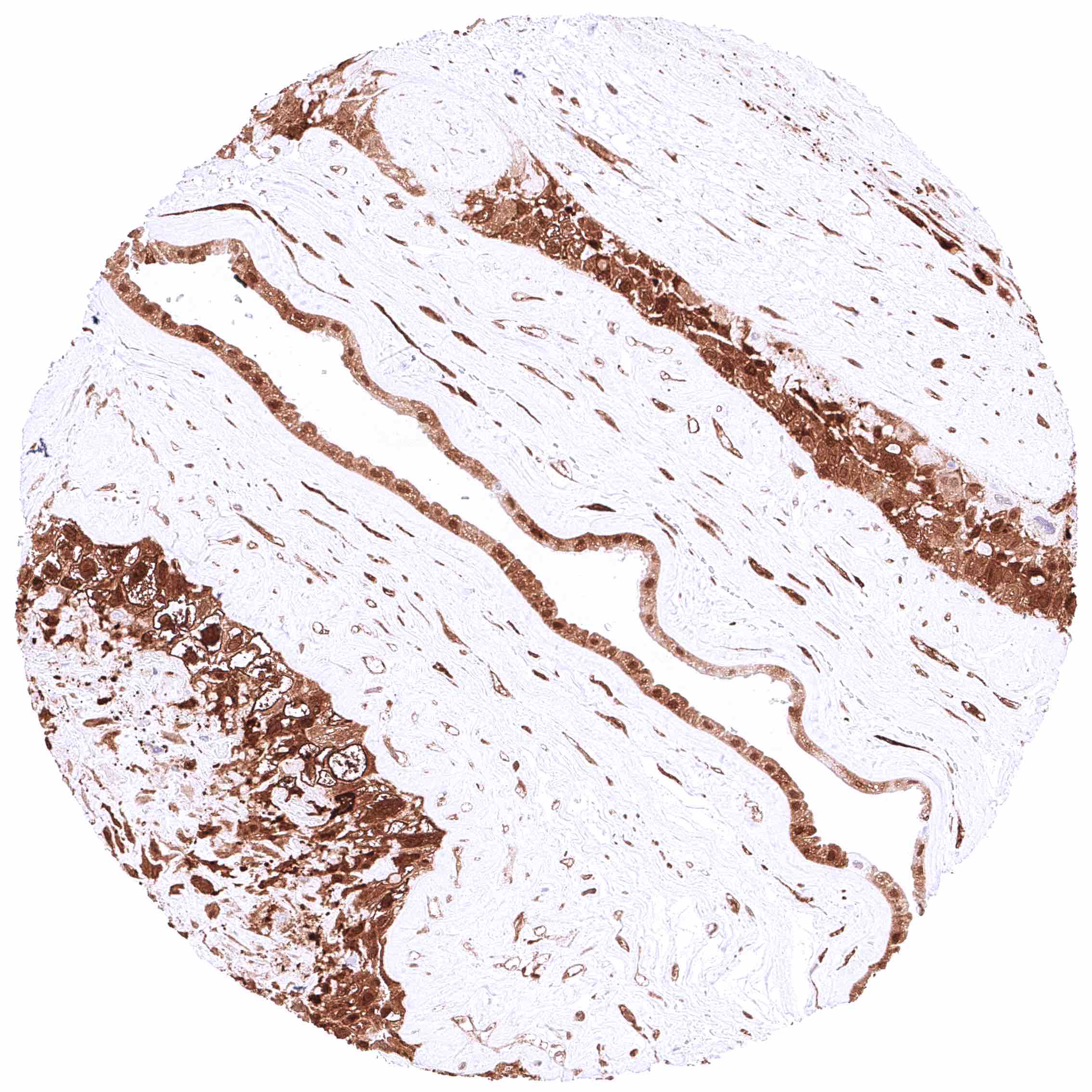
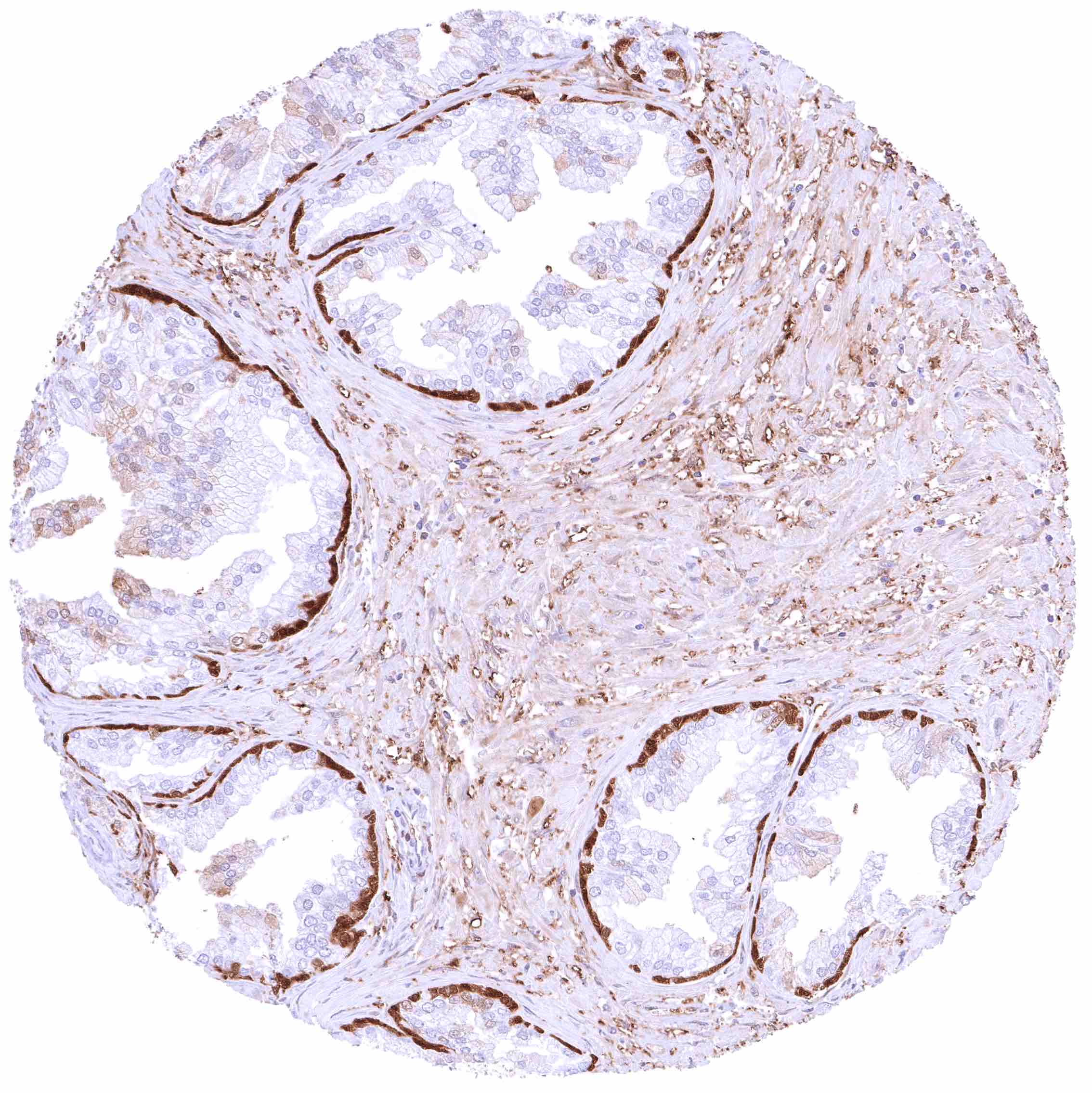
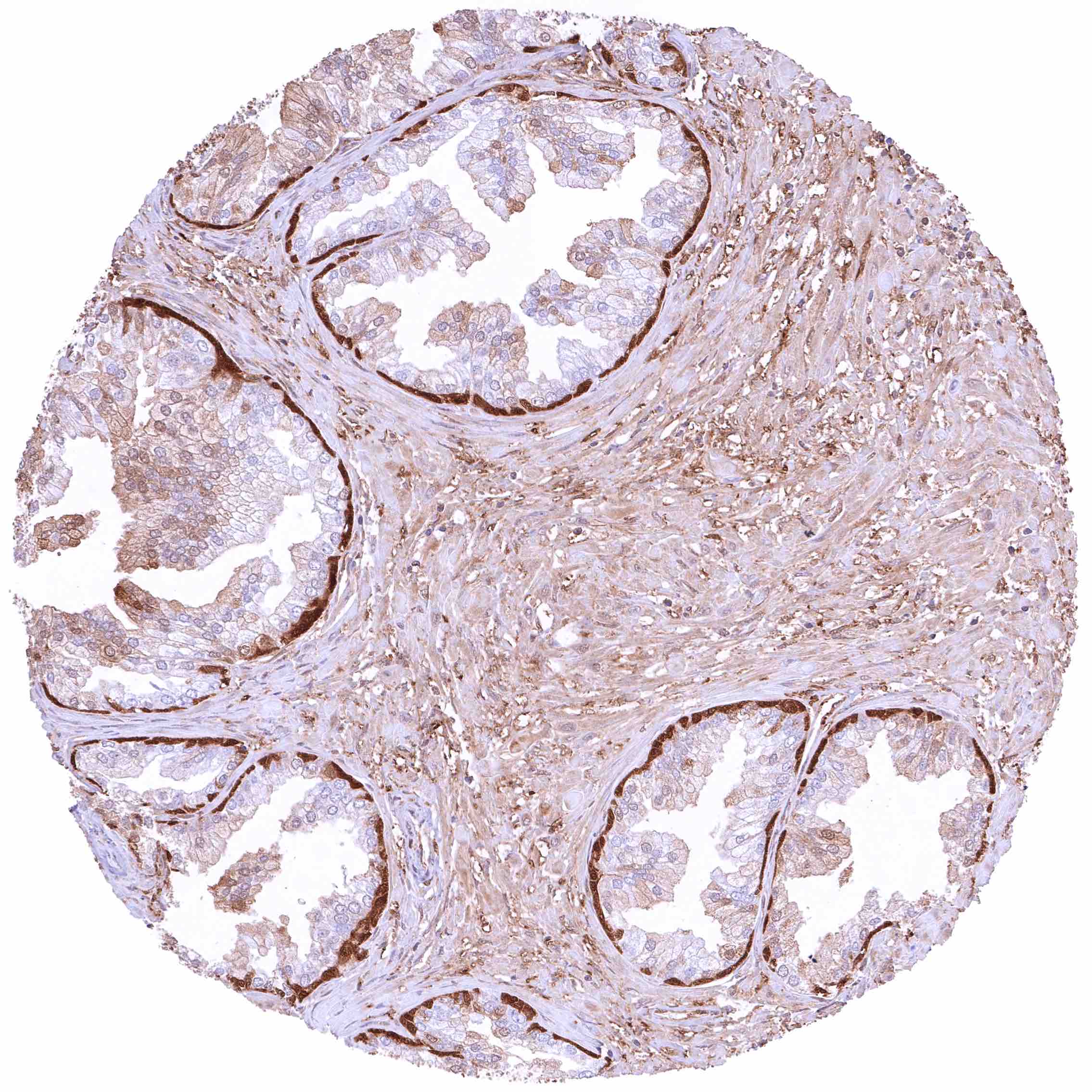
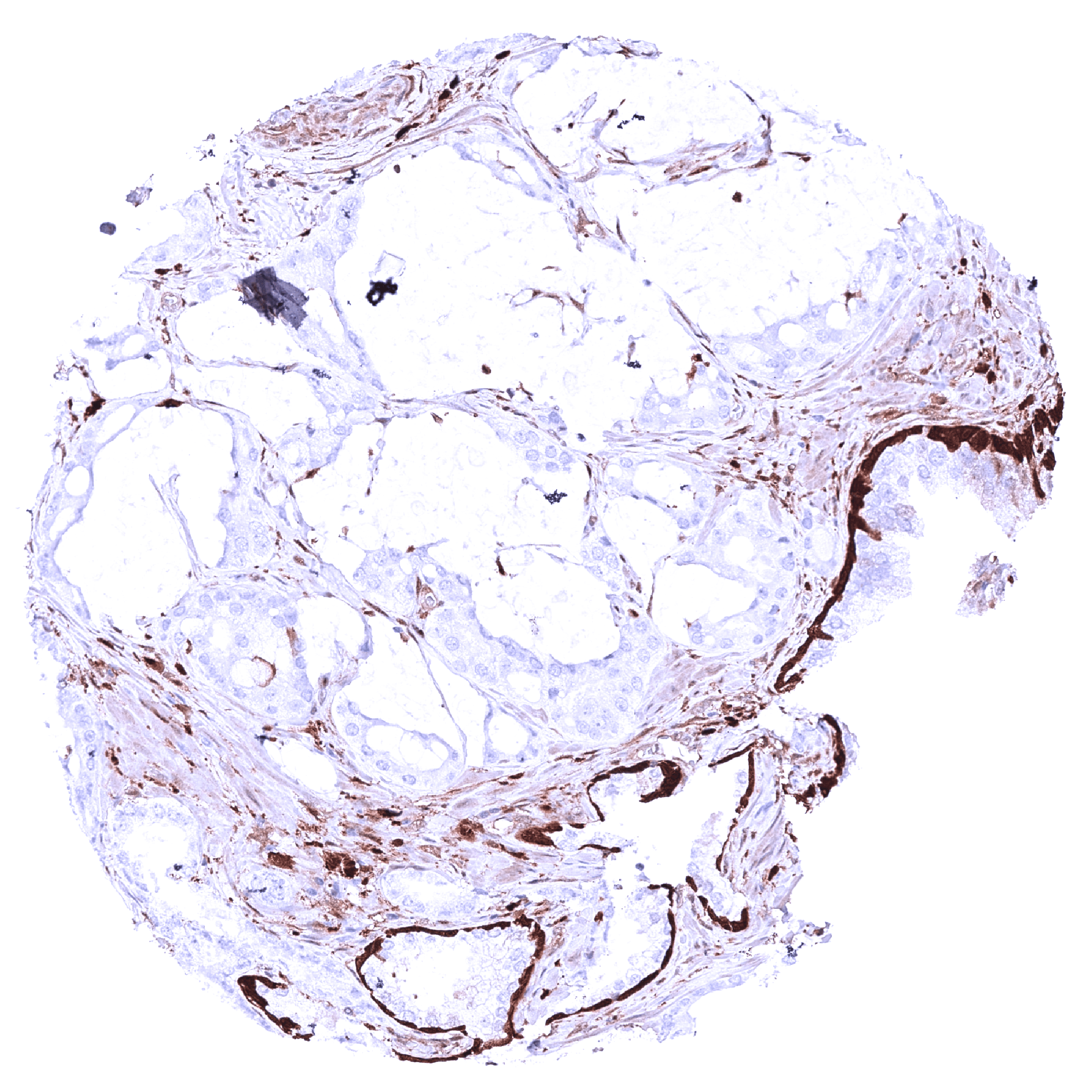
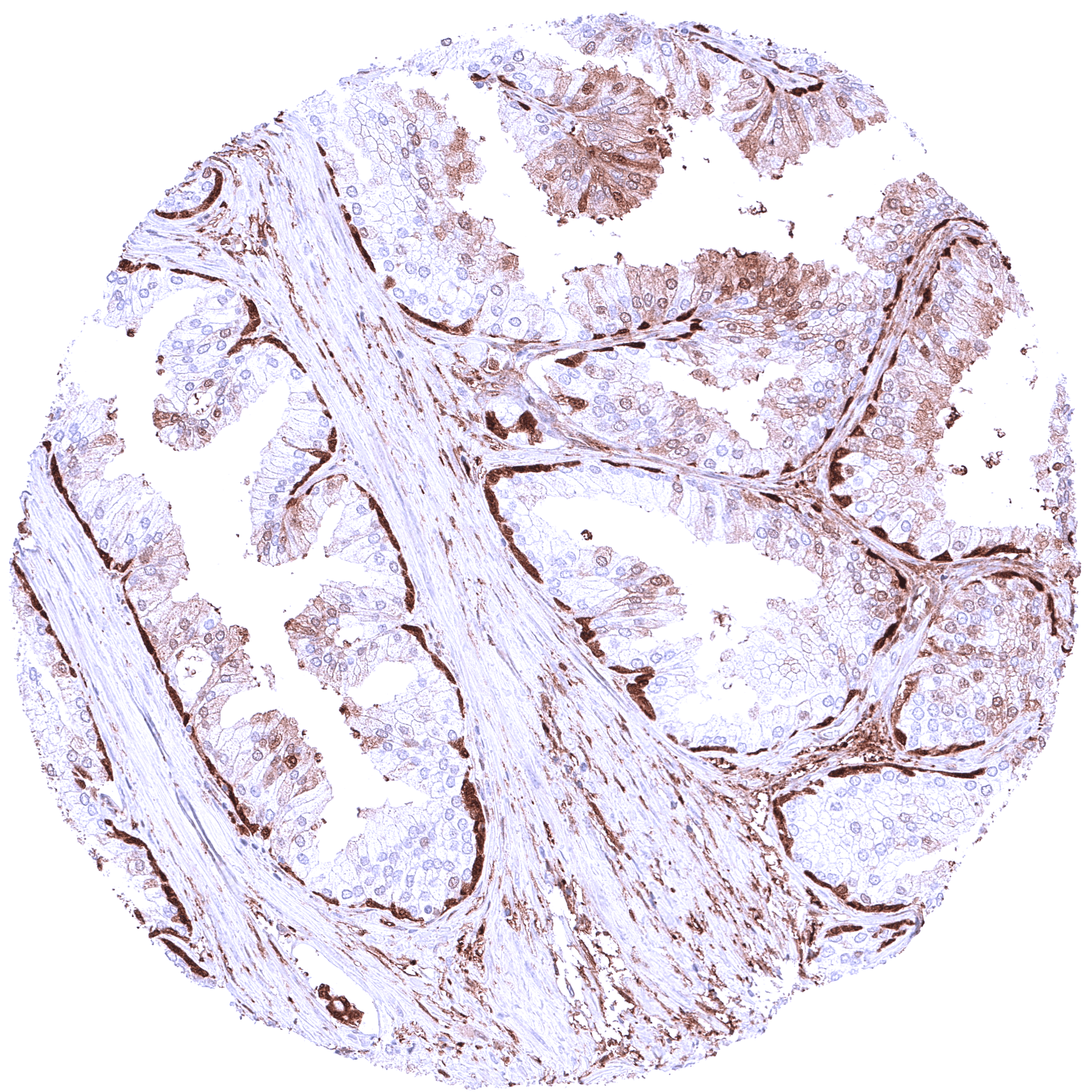
Positive control = Prostate: A strong nuclear and cytoplasmic GSTP1 staining should be seen in all basal cells of the prostate.
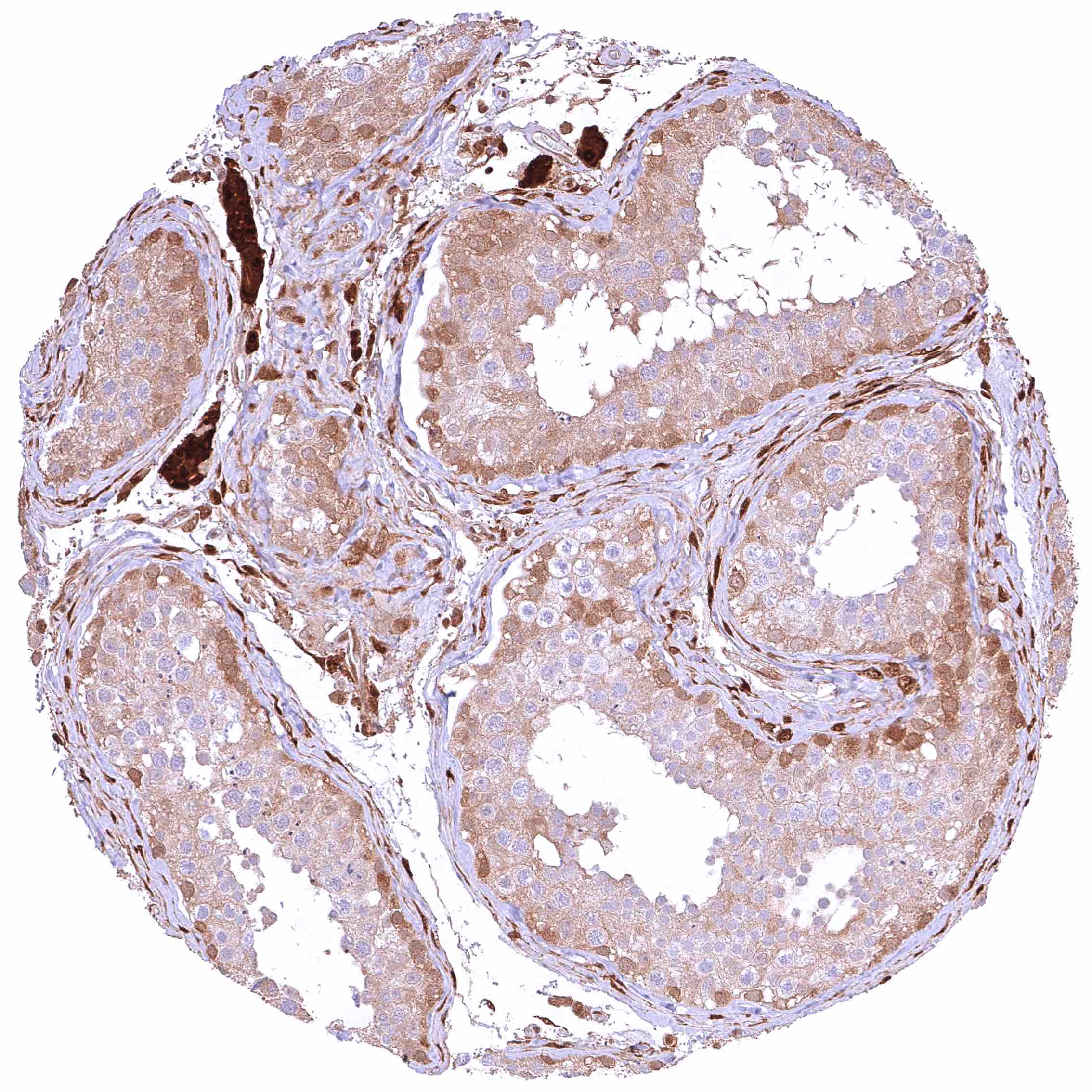
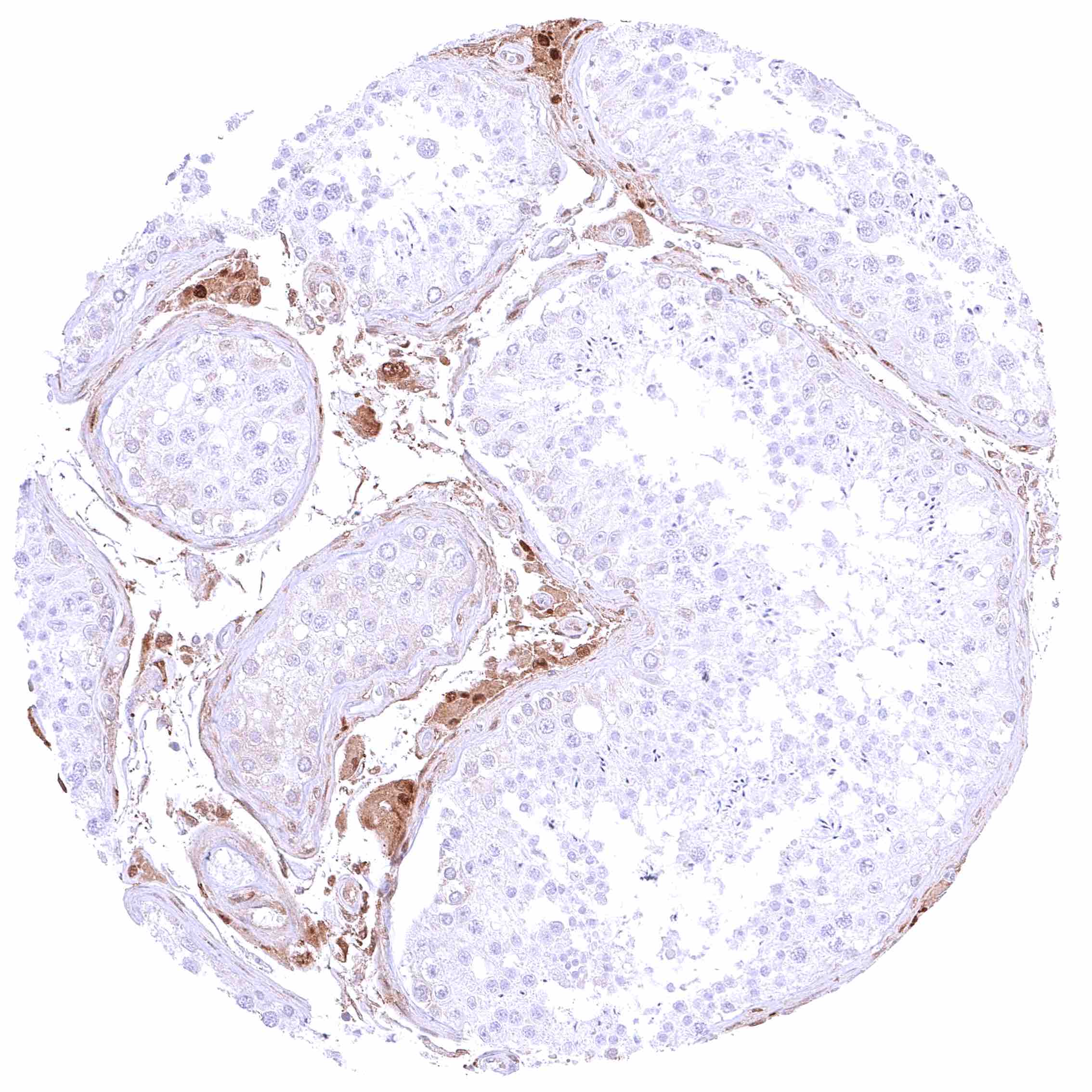
Negative control = GSTP1 staining must be absent in Sertoli cells and in maturing germ cells (weak positivity should be seen in spermatogonia).
Cellular localization = Nuclear and cytoplasmic
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
GSTP1 is critical for cell detoxification and a therapeutic target.
Biology Behind
Glutathione S-Transferase Pi1 (GSTP1) is a 23 kDa enzyme protein which is coded by the GSTP1 gene at chromosome 11q13.2 and belongs to the glutathione S-transferase (GST) family of enzymes that catalyze the conjugation of glutathione to a variety of electrophilic compounds. This activity is crucial for the detoxification of endogenous and exogenous carcinogens, oxidative stress products and drugs, thereby protecting cells from oxidative damage and mutagenesis. According to its critical role, GSTP1 is ubiquitously expressed in human cells. It is particularly abundant in epithelial cells. GSTP1 polymorphisms have been associated with altered susceptibility to various cancer types, but also other diseases such as non-alcoholic fatty liver. Accordingly, GSTP1 knockout mice have shown increased sensitivity to environmental carcinogens, oxidative stress, and inflammation. GSTP1 dysregulation plays a significant role in cancer development and progression. Overexpression of GSTP1 can contribute to resistance to chemotherapy by detoxifying anticancer drugs. Decreased GSTP1 activity or expression, often due to epigenetic silencing, can heighten vulnerability to carcinogenic damage and support tumor progression through an increased rate of DNA mutations. Cancer studies by IHC have described an unfavorable prognostic impact of both reduced and increased GSTP1 expression and suggested a predictive role of high expression for chemo-resistance. GSTP1 is a potential therapeutic target for cancer and other diseases. Inhibitors of GSTP1, such as ezatiostat and others are under clinical investigation as sensitizers to chemotherapy or modulators of immune response.
Staining Pattern in Normal Tissues
A nuclear and/or cytoplasmic GSTP1 immunostaining occurs – at variable intensity – in most cell types.
Images describing the GSTP1 staining pattern in normal tissues obtained by the antibody MSVA-685R are shown in our “Normal Tissue Gallery”.
| Brain | Cerebrum | Distinct GSTP1 positivity of fibres and of all cell types except neurons. |
| Cerebellum | Moderate to strong GSTP1 staining of Purkinje cells and fibers in the molecular layer. Weak to moderate positivity of a small subset of cells of the granule cell layer and of endothelial cells. | |
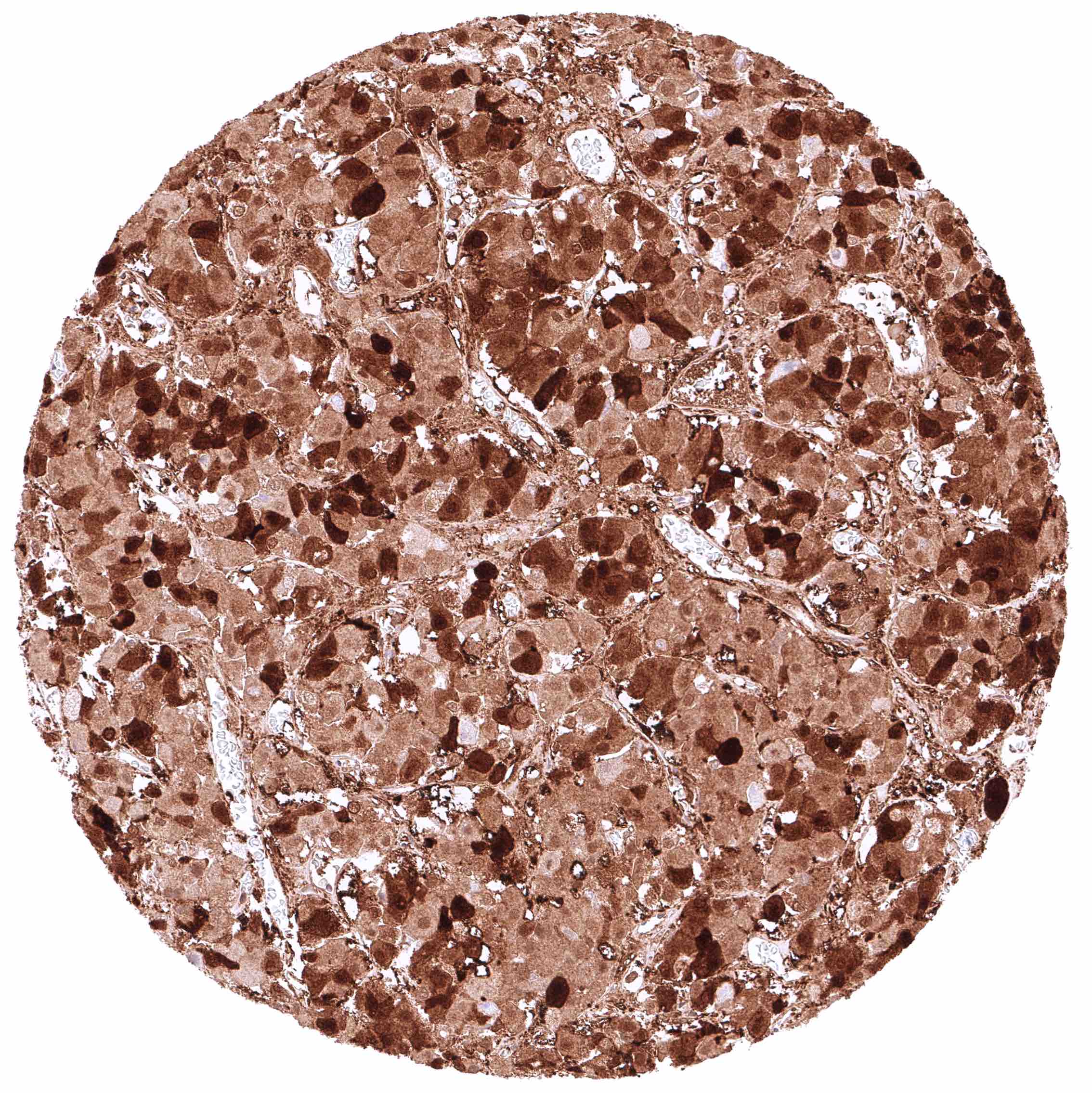
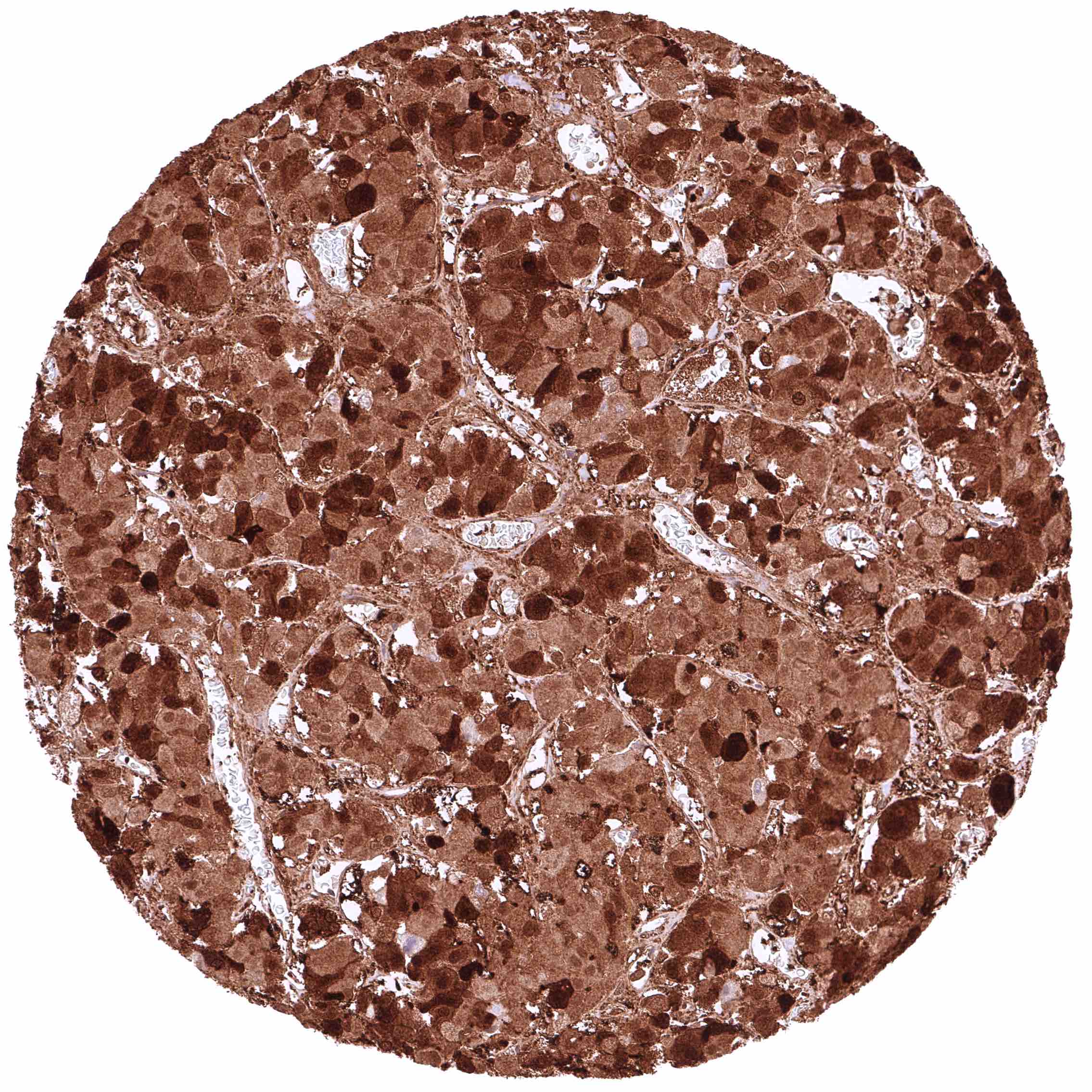
| Endocrine Tissues | Thyroid | Strong nuclear and cytoplasmic GSTP1 positivity of epithelial cells. |
| Parathyroid | Strong nuclear and cytoplasmic GSTP1 positivity of epithelial cells. | |
| Adrenal gland | Moderate to strong nuclear and cytoplasmic GSTP1 positivity of epithelial cells. | |
| Pituitary gland | All cells are GSTP1 positive in the adenohypophysis, but the intensity varies sharply from weak/moderate to intense. Distinct GSTP1 positivity of fibres and probably also of pituicytes in the neurohypophysis. | |
| Respiratory system | Respiratory epithelium | Variable, moderate to strong nuclear and cytoplasmic GSTP1 positivity of respiratory epithelial cells. |
| Lung | Weak to moderate, predominantly cytoplasmic positivity of alveolar endothelial cells. Strong, nuclear and cytoplasmic GSTP1 positivity of at least a significant subset of alveolar cells. | |
| Gastrointestinal Tract | Salivary glands | Weak to moderate, predominantly cytoplasmic GSTP1 staining of glandular cells (often more intense in mucinous than in serous glands). Staining is markedly stronger in intercalated and excretory ducts. |
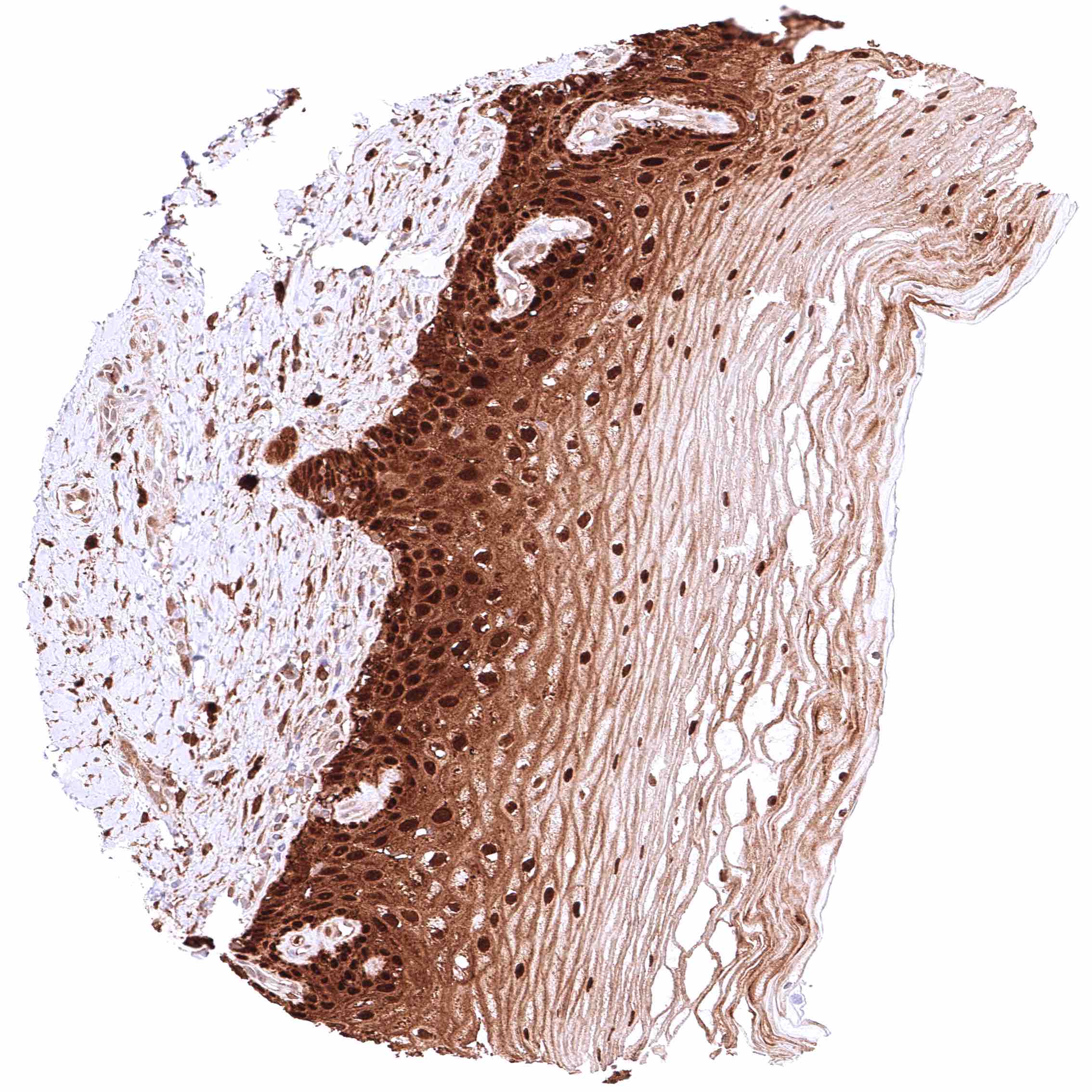
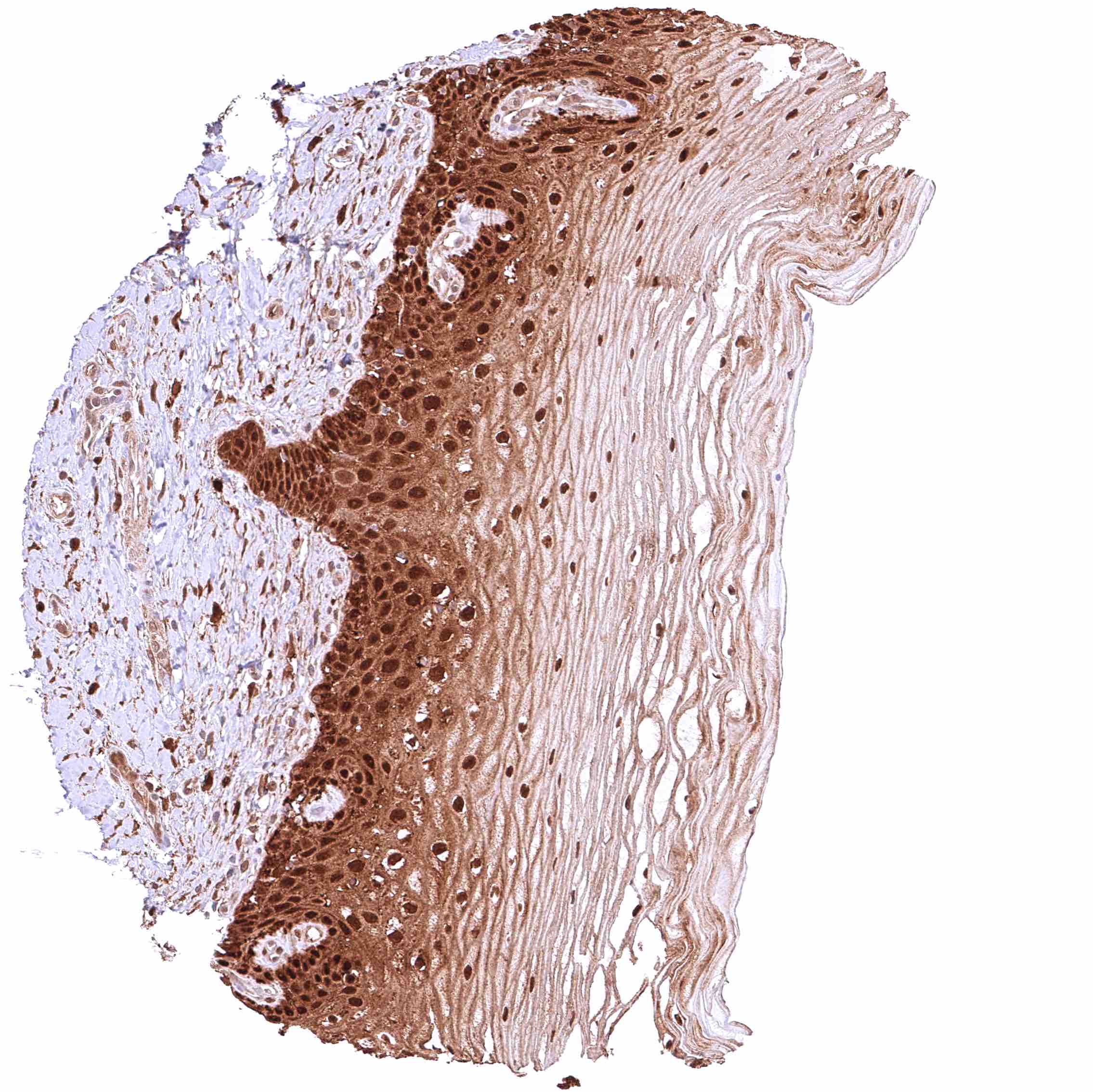
| Esophagus | Strong cytoplasmic and nuclear GSTP1 positivity of squamous epithelial cells. Staining intensity is highest in the basal and suprabasal cell layers and decreases slightly towards the surface. | |
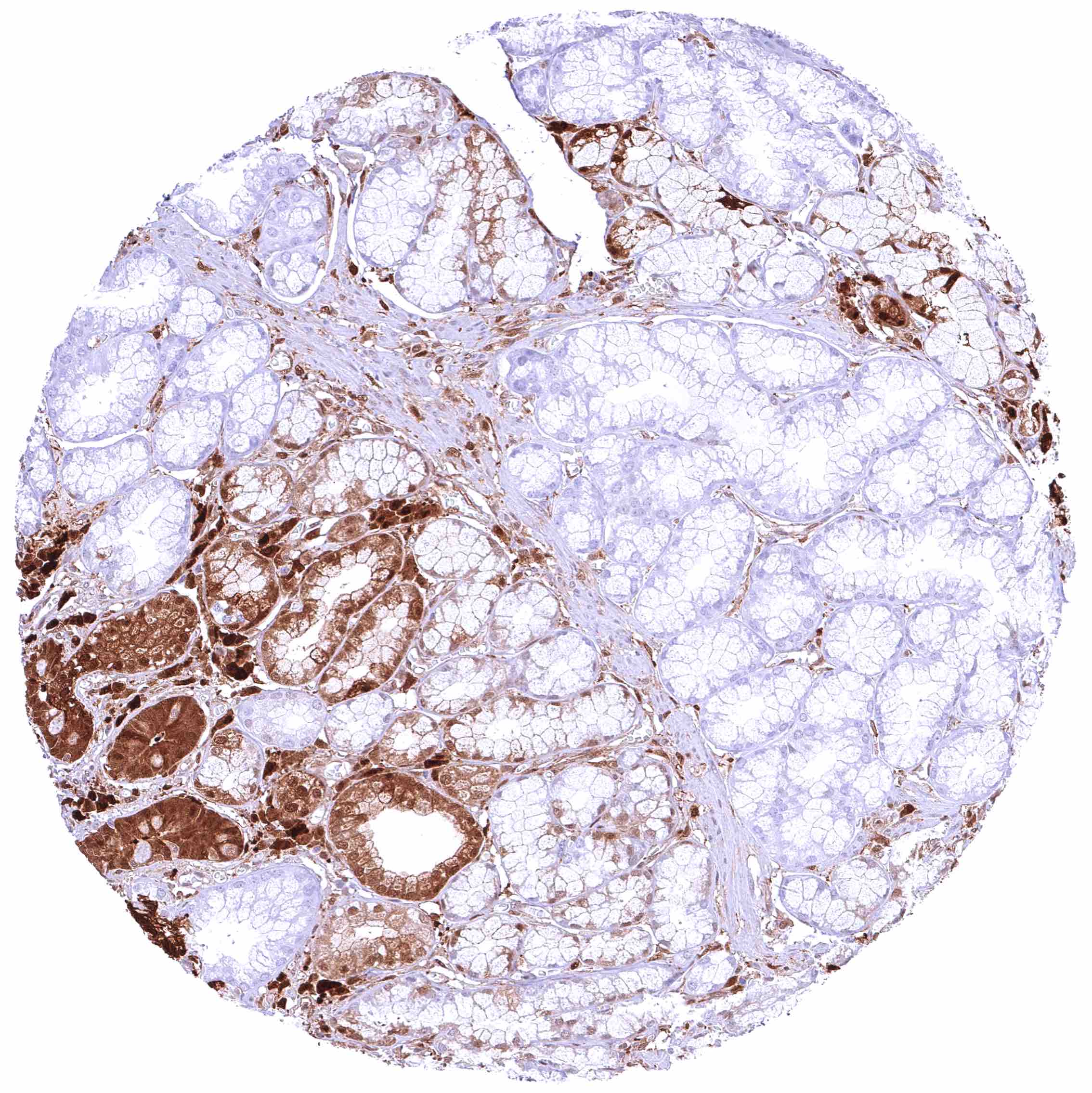
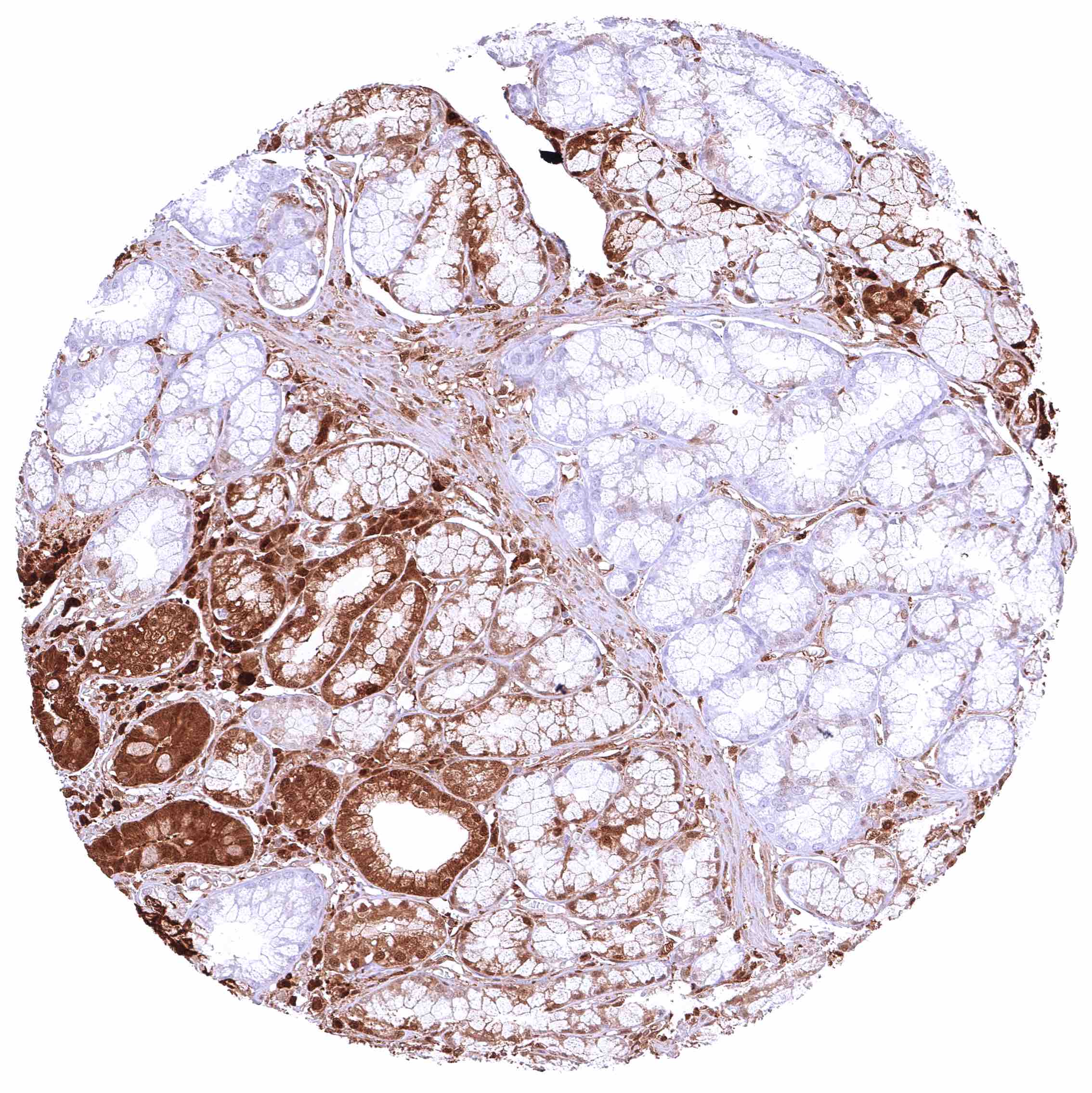
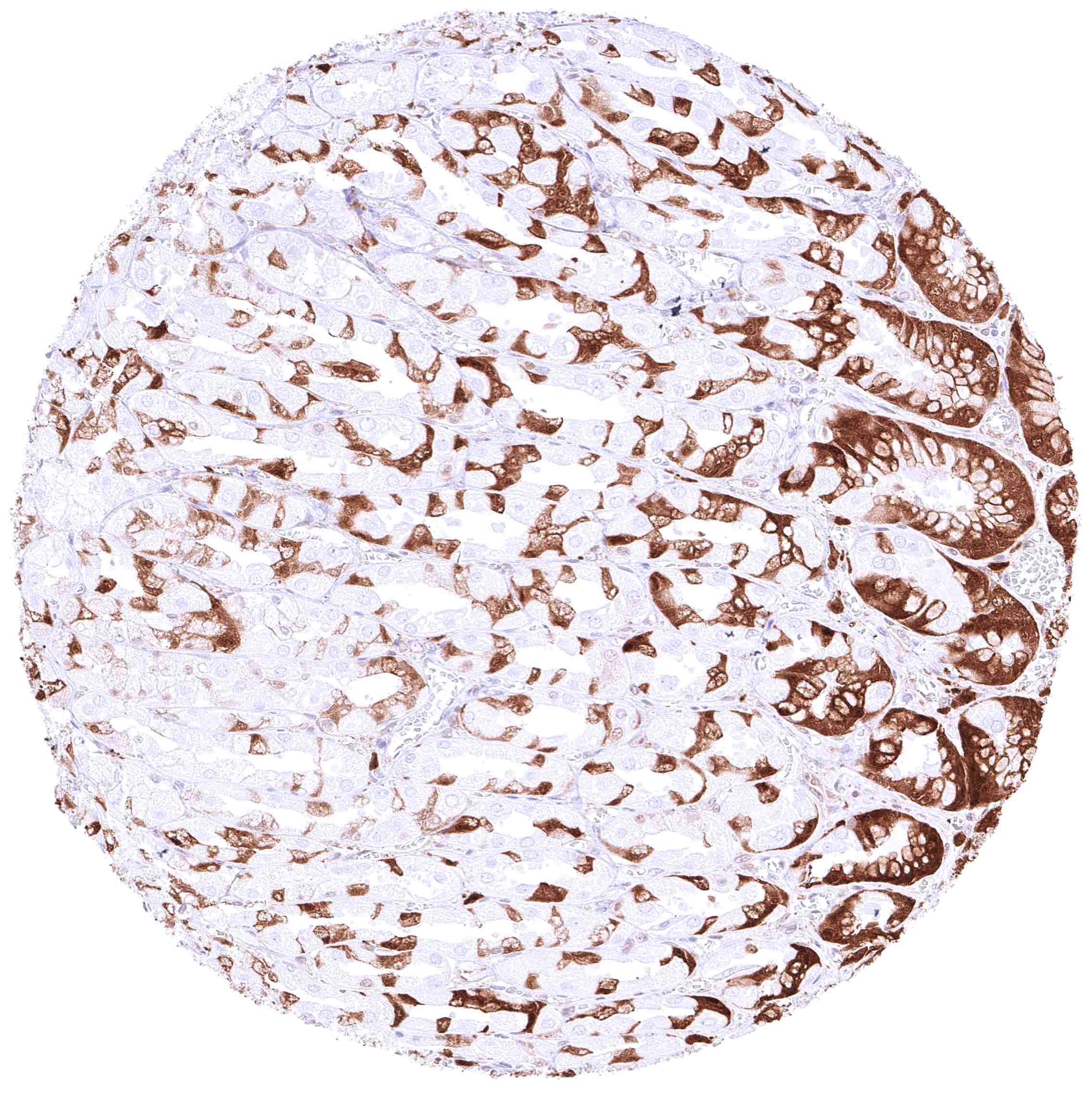
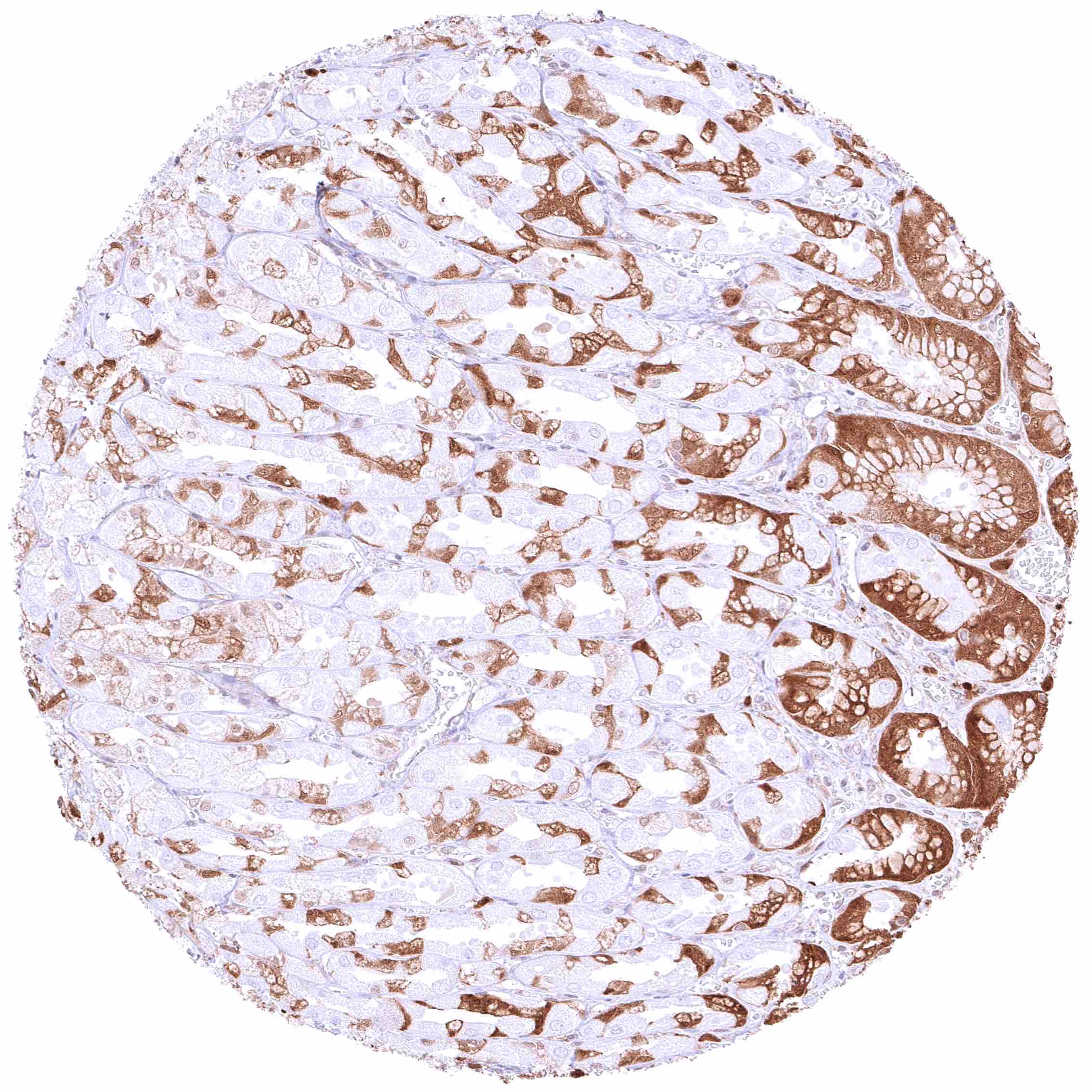
| Stomach | Strong, predominantly cytoplasmic GSTP1 positivity of gastric surface epithelium and specific glandular cells (parietal cells and endocrine cells? are GSTP1 negative). | |
| Duodenum | Strong predominantly cytoplasmic GSTP1 positivity of epithelial cells. Staining is most intense at the base of crypts and decreases slightly towards the surface epithelium.
Brunner glands are largely GSTP1 negative if cells are distant from the mucosa layer. |
|
| Small intestine | Strong predominantly cytoplasmic GSTP1 positivity of epithelial cells. Staining is most intense at the base of crypts and decreases slightly towards the surface epithelium. | |
| Appendix | Strong predominantly cytoplasmic GSTP1 positivity of epithelial cells. Staining is most intense at the base of crypts and decreases slightly towards the surface epithelium. | |
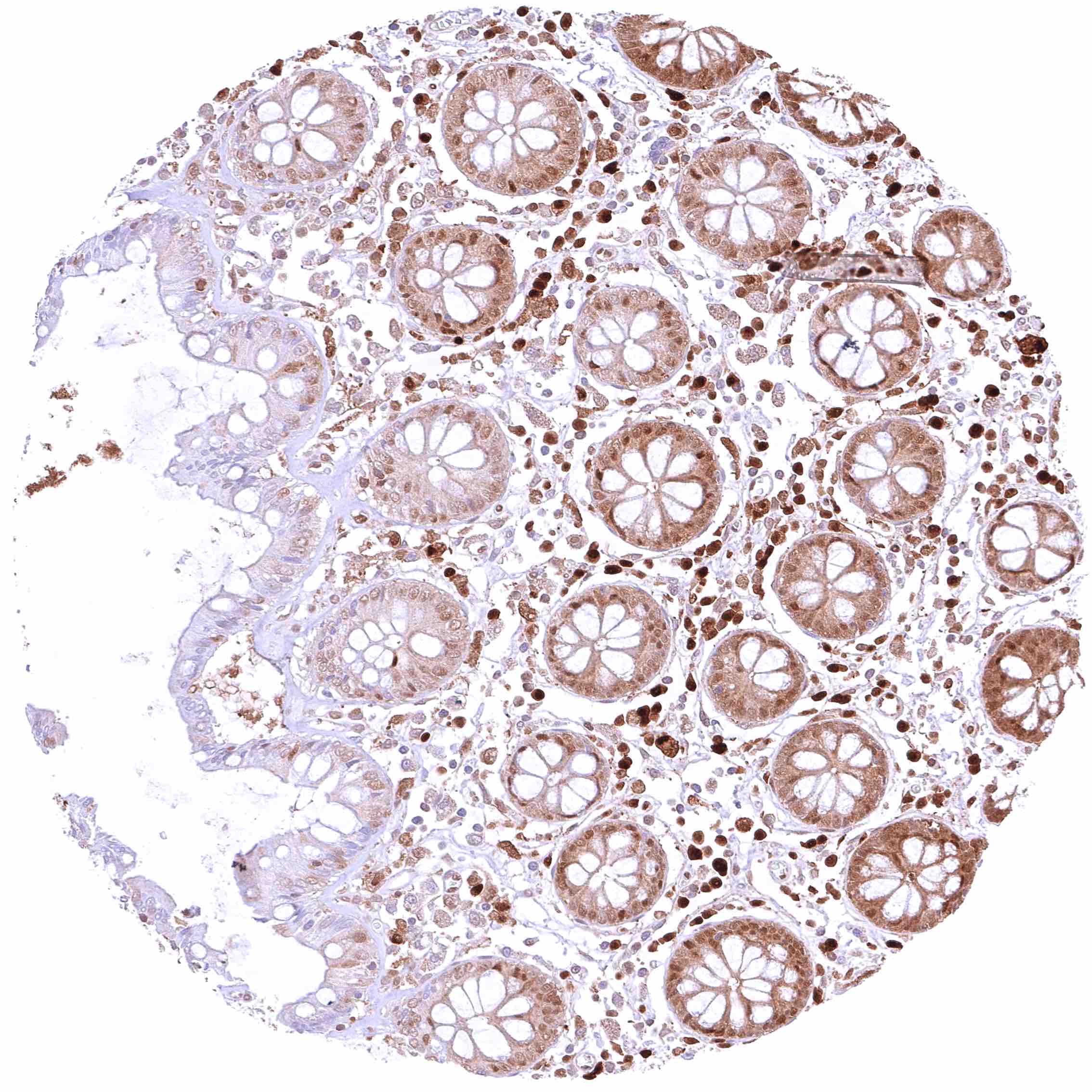
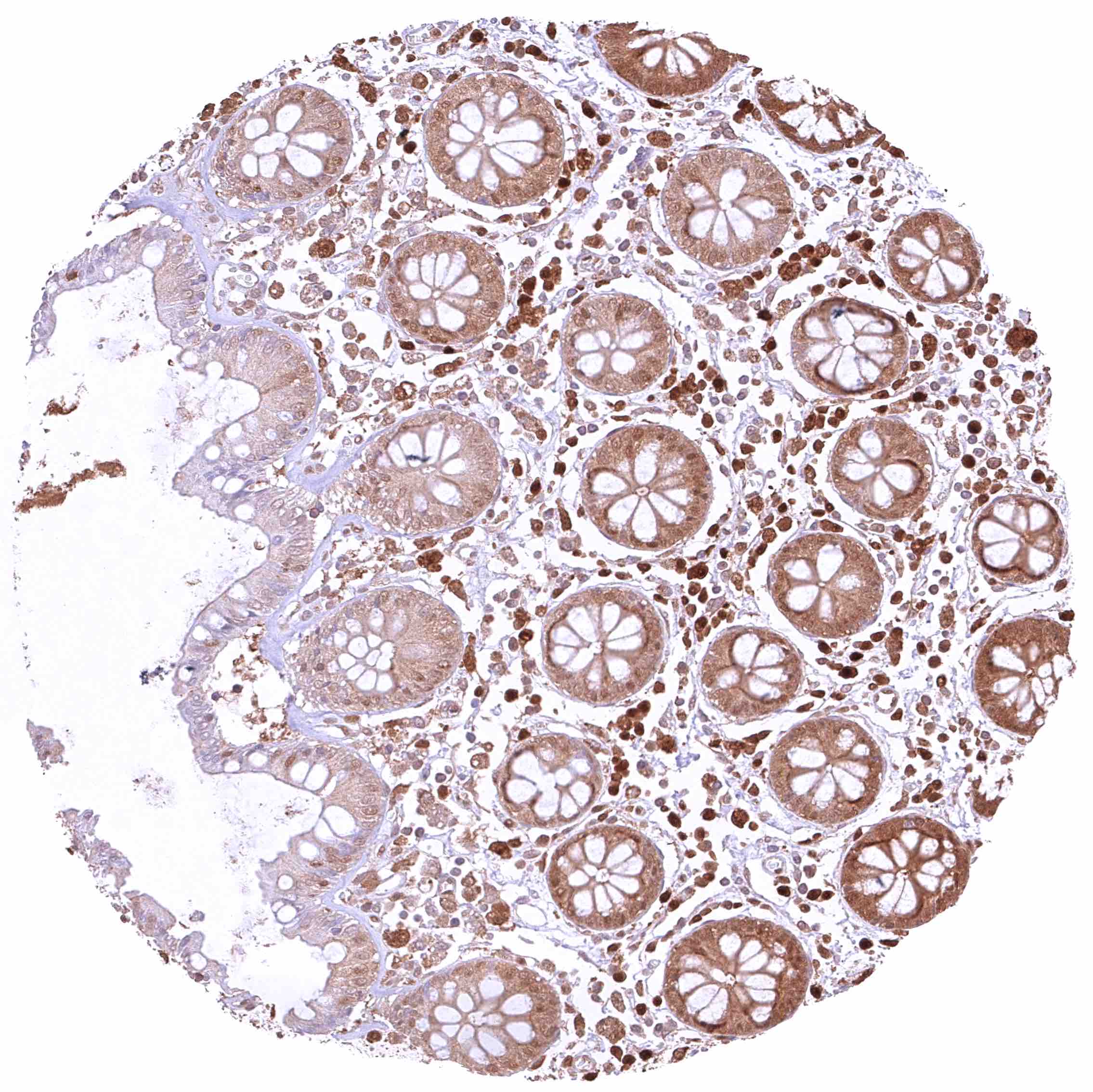
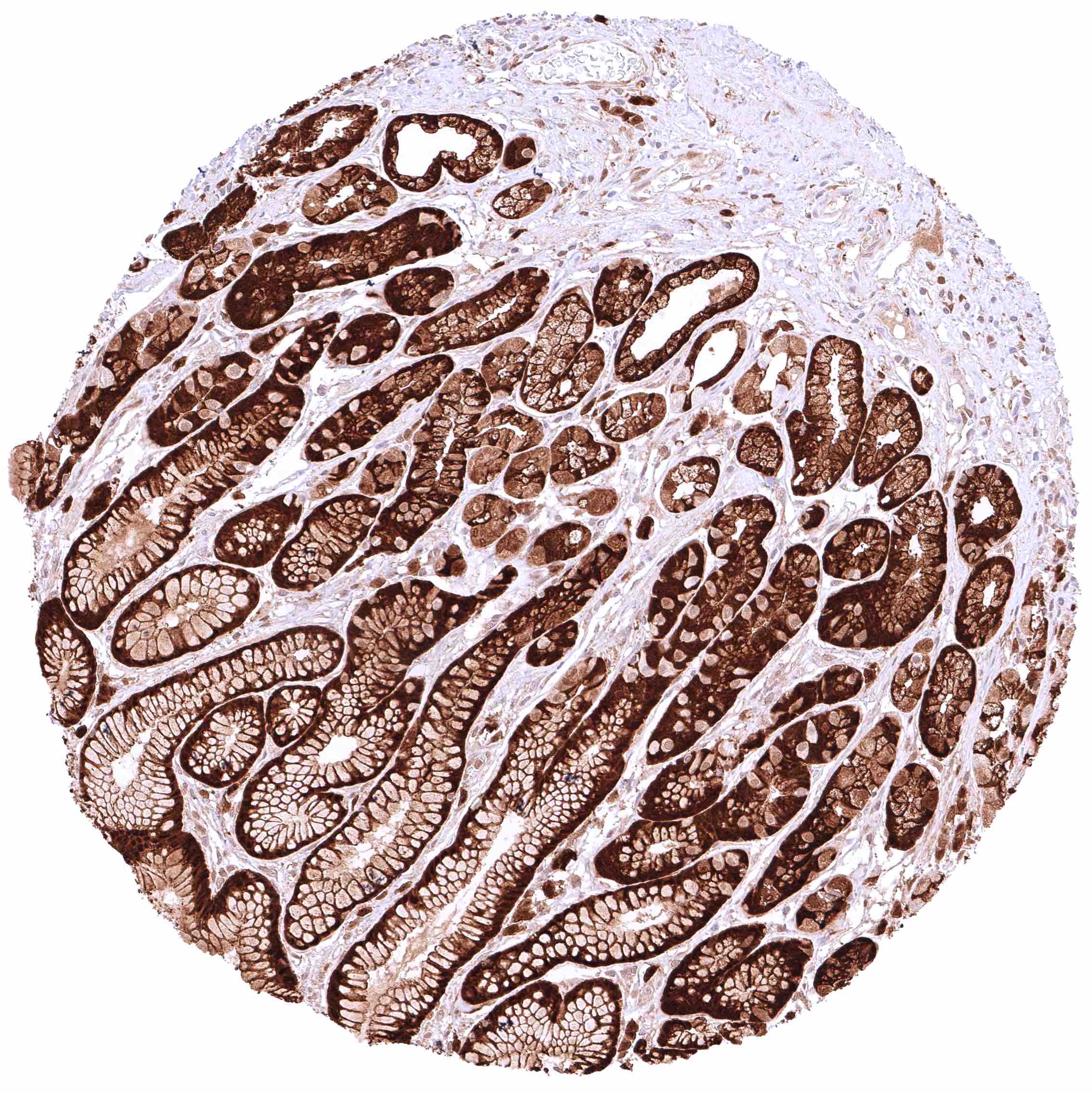
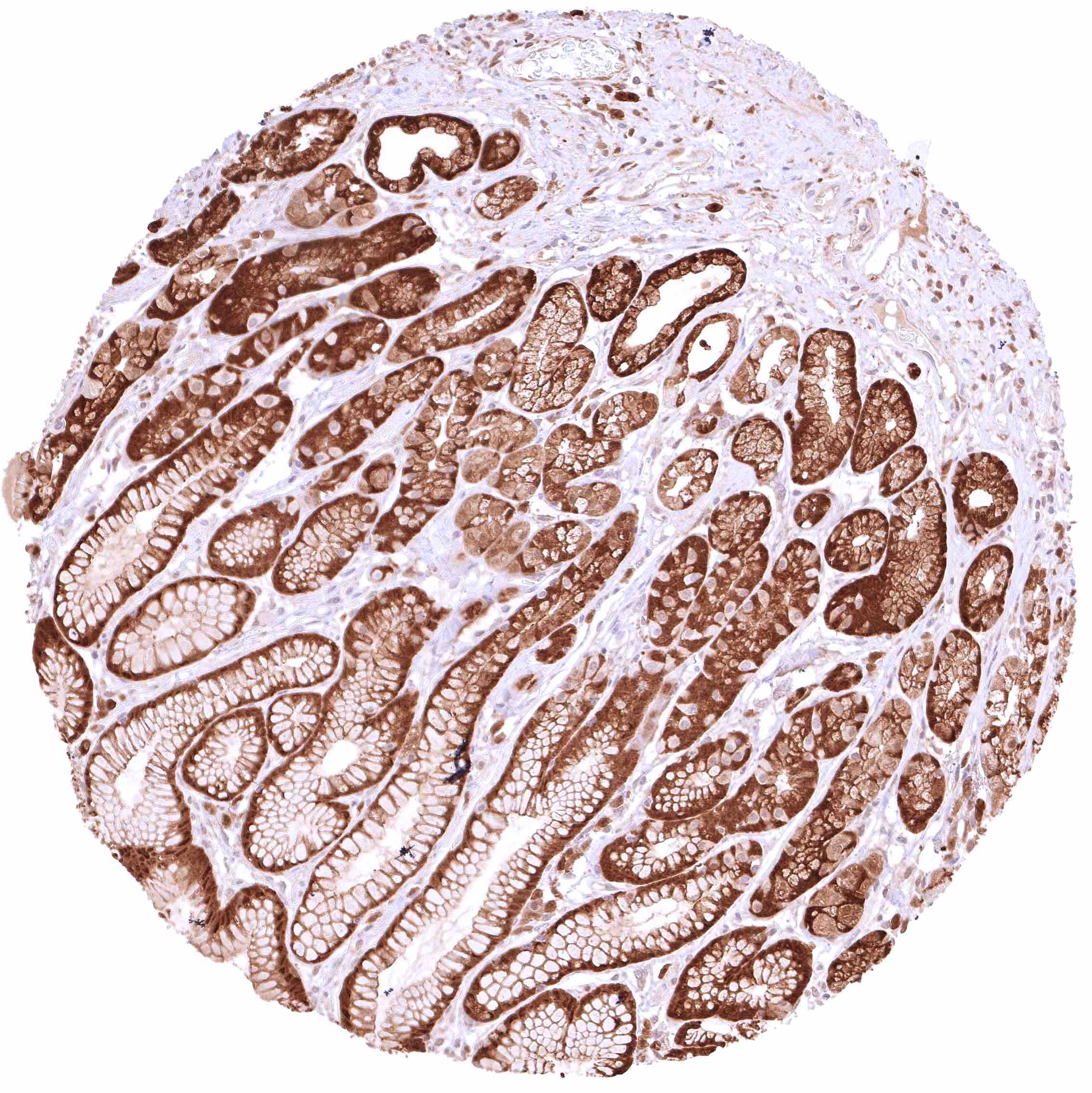
| Colon | Strong predominantly cytoplasmic GSTP1 positivity of epithelial cells. Staining is most intense at the base of crypts and decreases slightly towards the surface epithelium. | |
| Rectum | Strong predominantly cytoplasmic GSTP1 positivity of epithelial cells. Staining is most intense at the base of crypts and decreases slightly towards the surface epithelium. | |
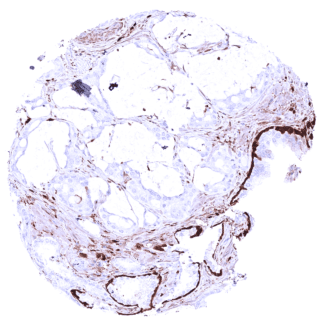
| Liver | Weak to moderate, cytoplasmic GSTP1 positivity of sinus endothelial cells while staining is stronger in Kopffer cells. Hepatocytes are GSTP1 negative. | |
| Gallbladder | Strong nuclear and cytoplasmic GSTP1 positivity of epithelial cells. | |
| Pancreas | Weak to moderate, nuclear and cytoplasmic GSTP1 positivity of acinar cells. Strong GSTP1 staining of intercalated and excretory ducts. Weak GSTP1 positivity of only a subset of islet cells. | |
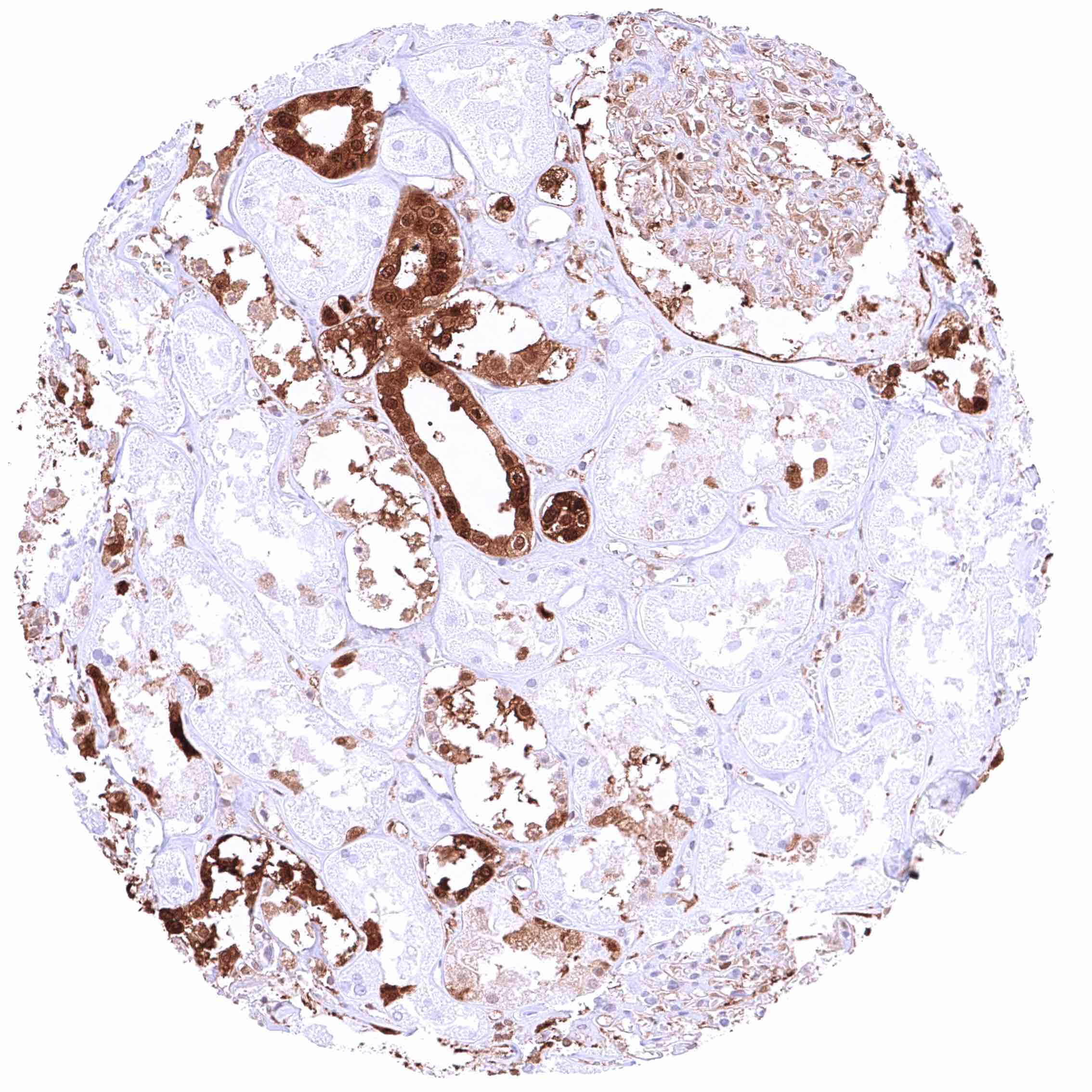
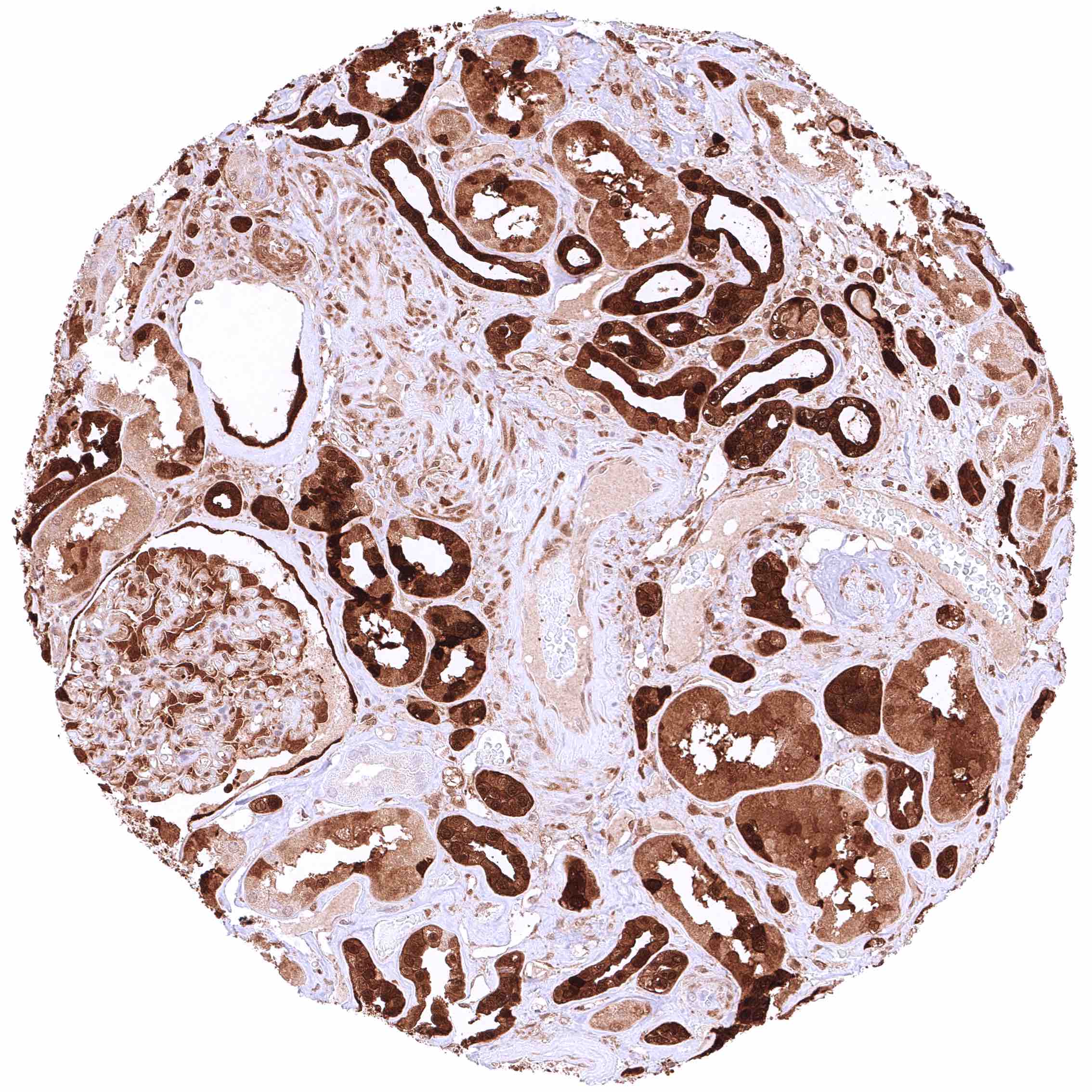
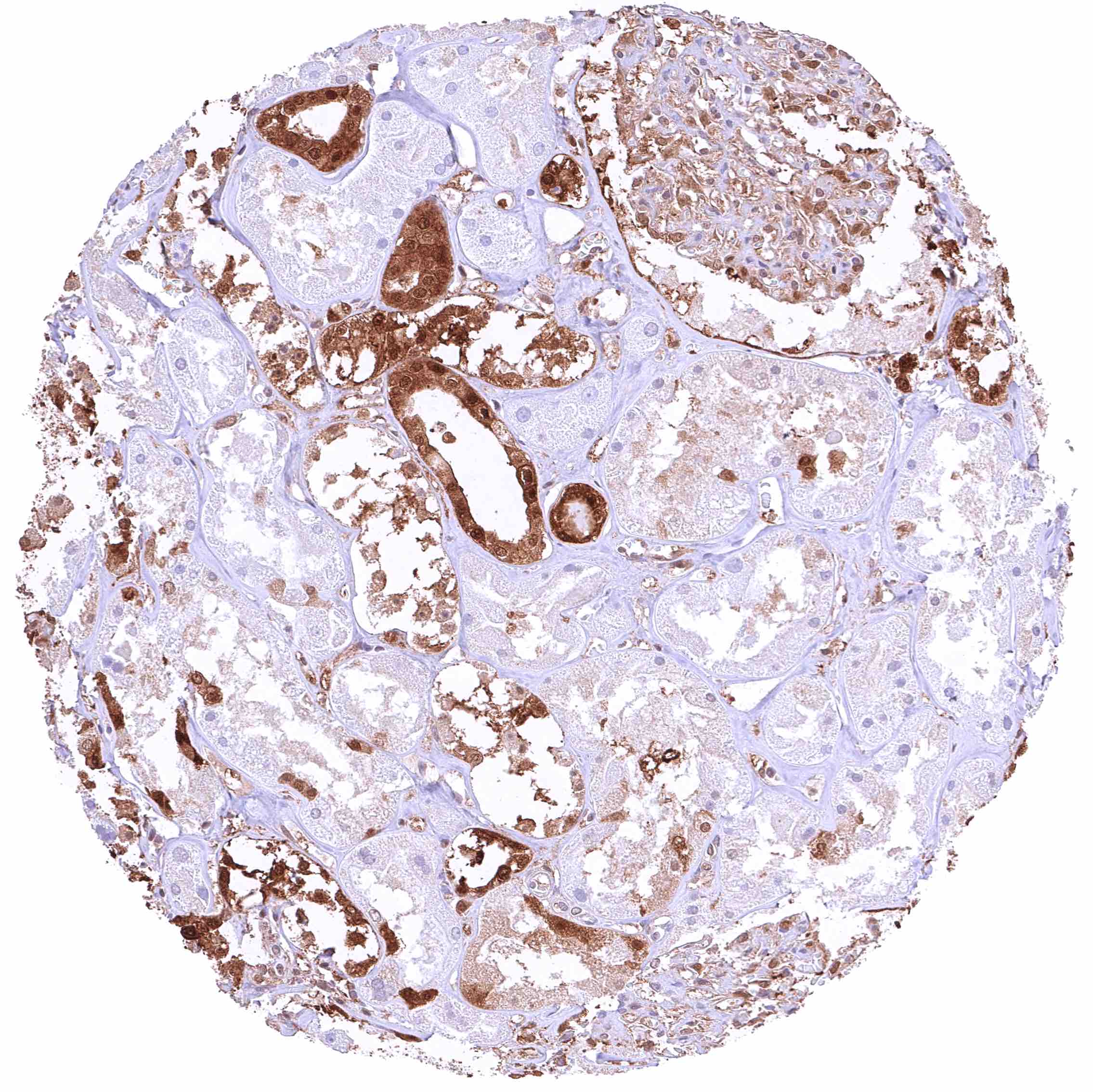
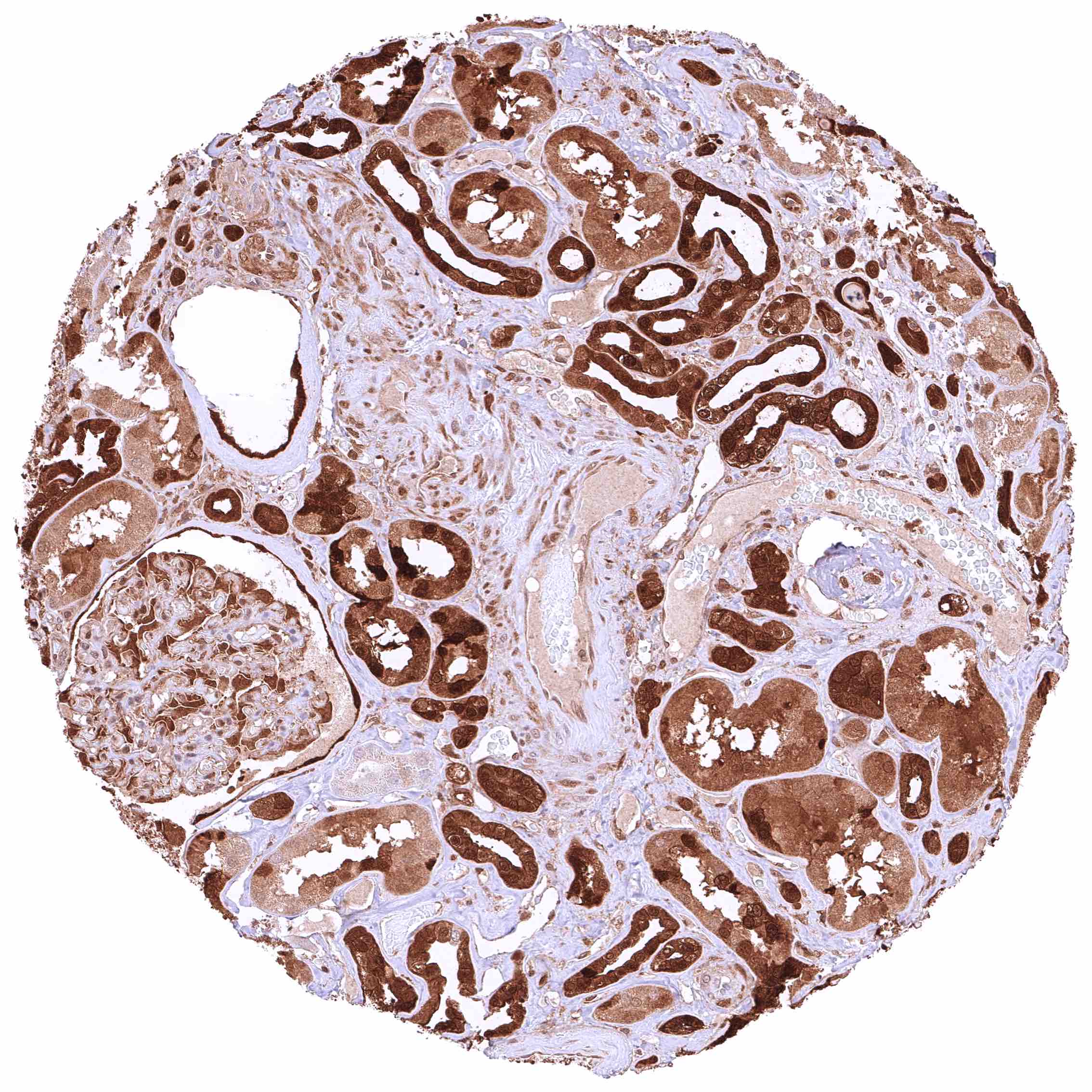
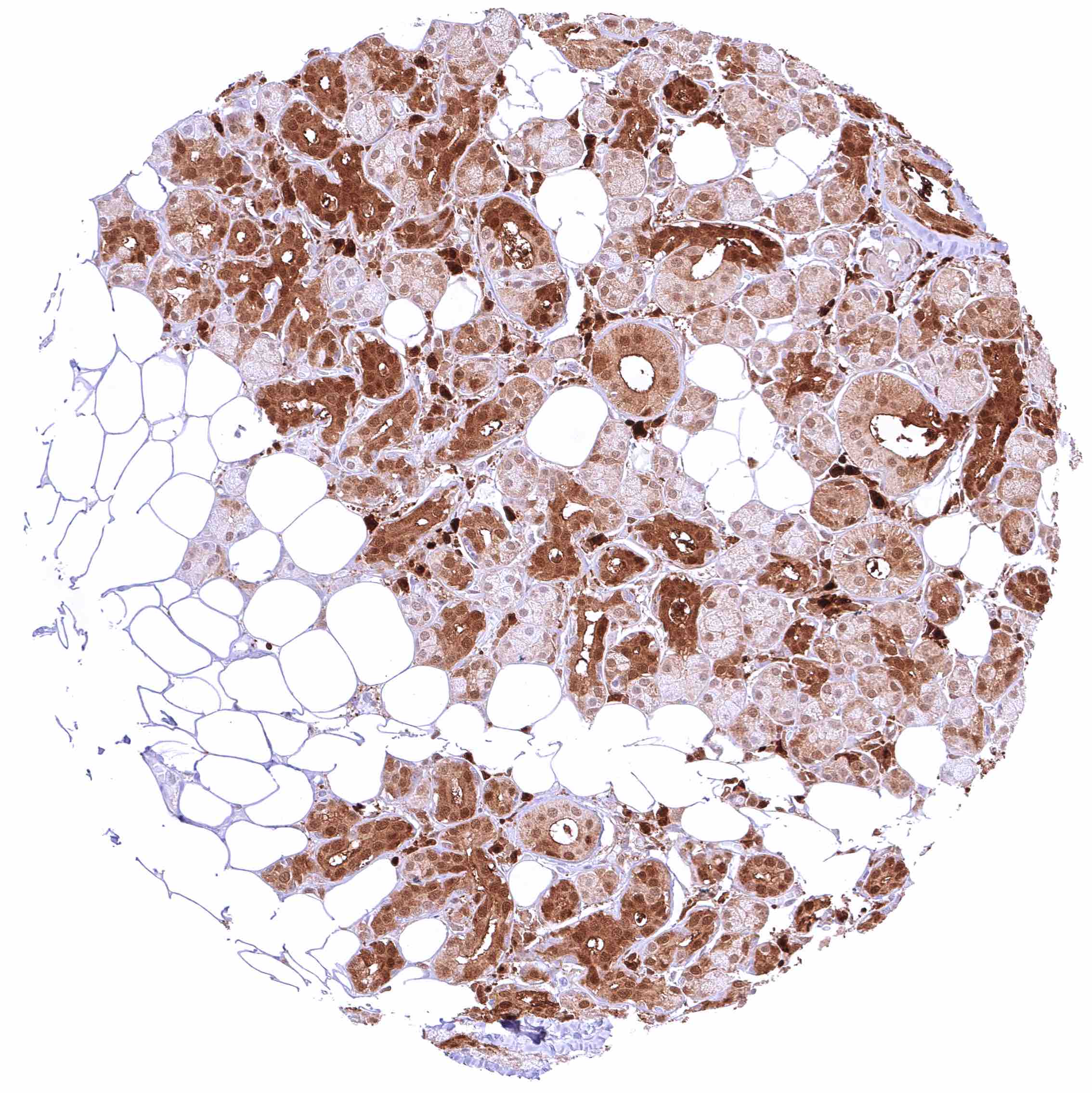
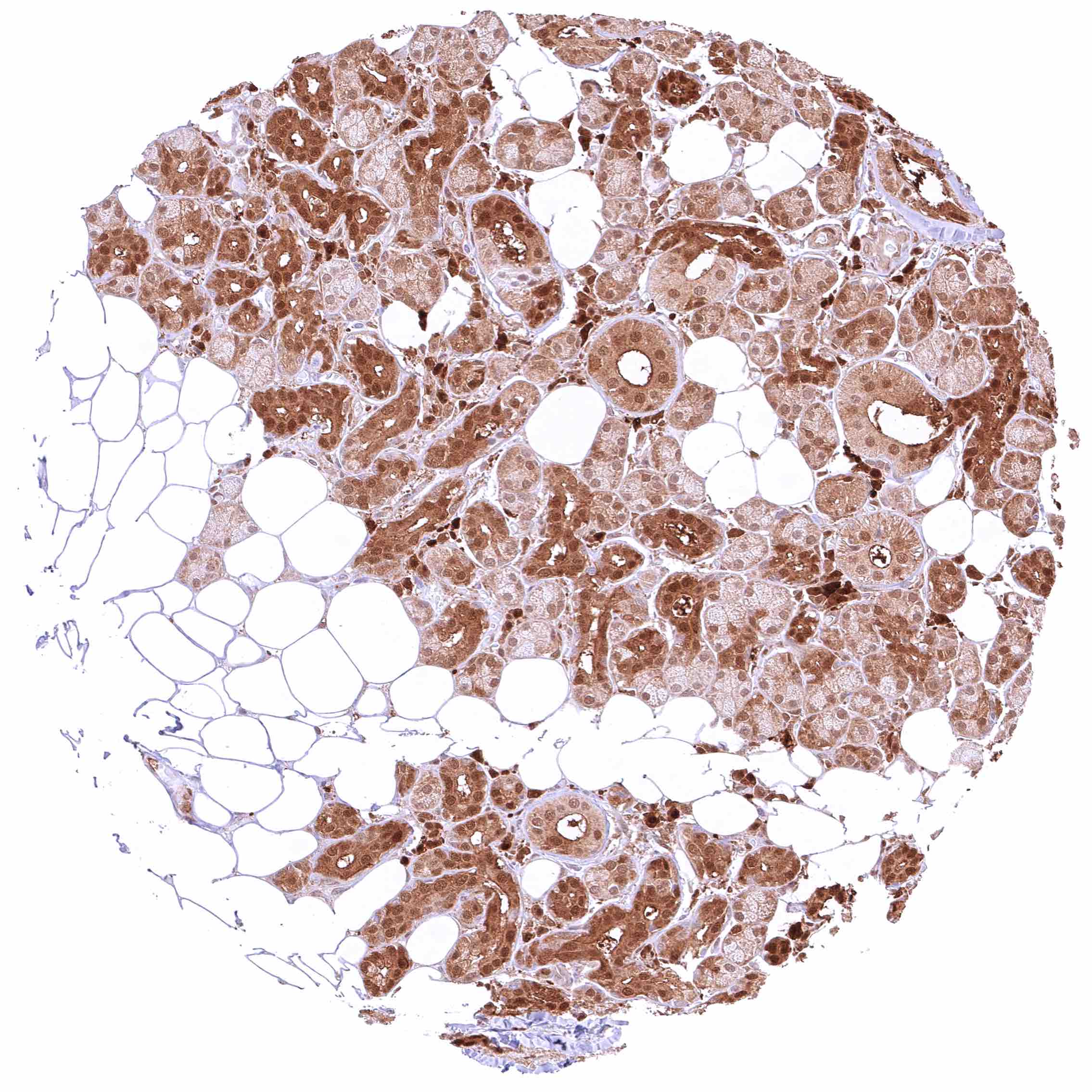
| Genitourinary | Kidney | GSTP1 staining is strong in collecting ducts and in the parietal layer of the capsule of Bowman. Among tubuli, the staining is variable but always stronger in distal than in proximal tubuli. In some samples, proximal tubules are negative while staining is strong in distal tubuli. In other samples GSTP1 staining ins moderate in proximal tubuli and intense in distal ones. |
| Urothelium | Strong, nuclear and cytoplasmic GSTP1 positivity of all urothelial cells (staining can be lower in umbrella cells). | |
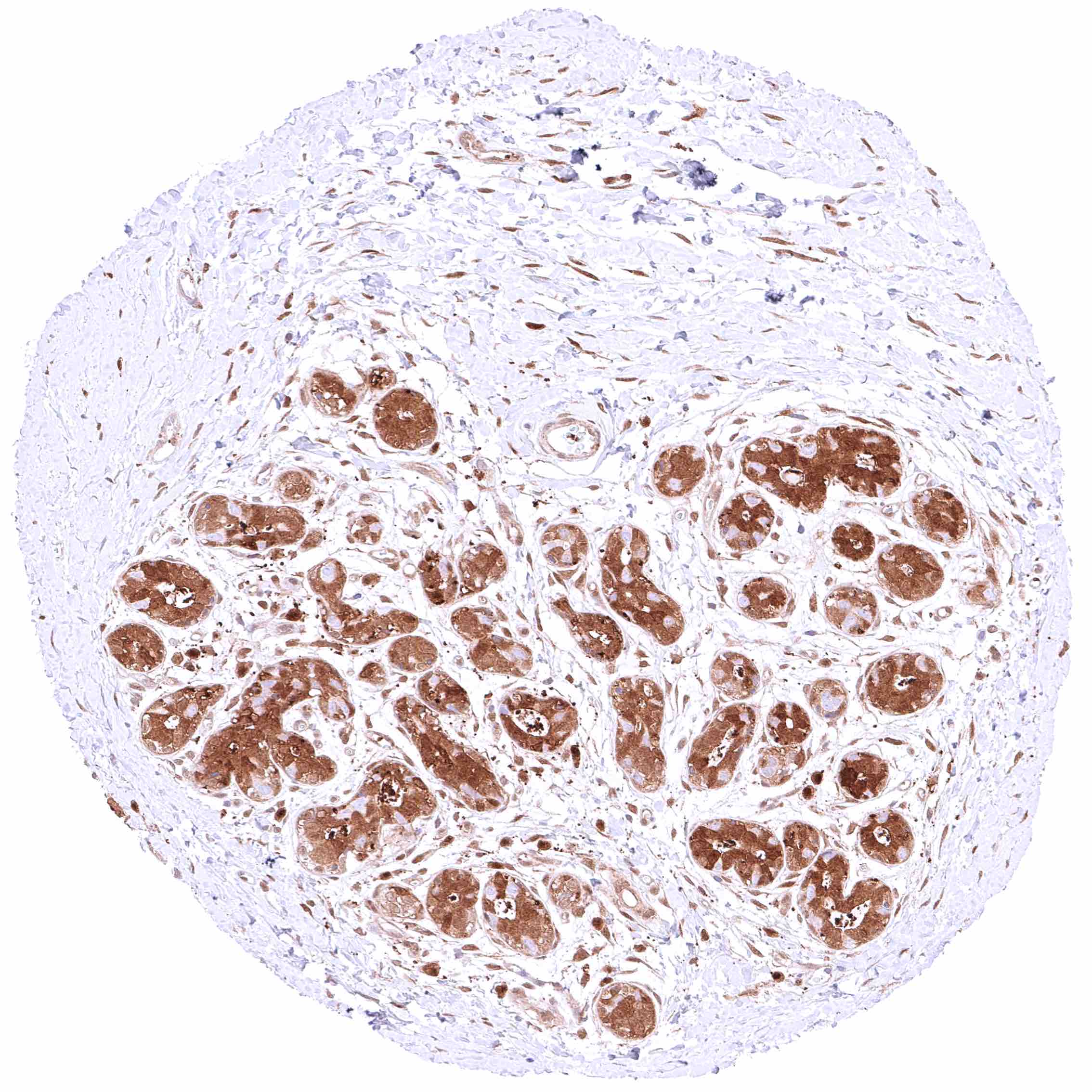
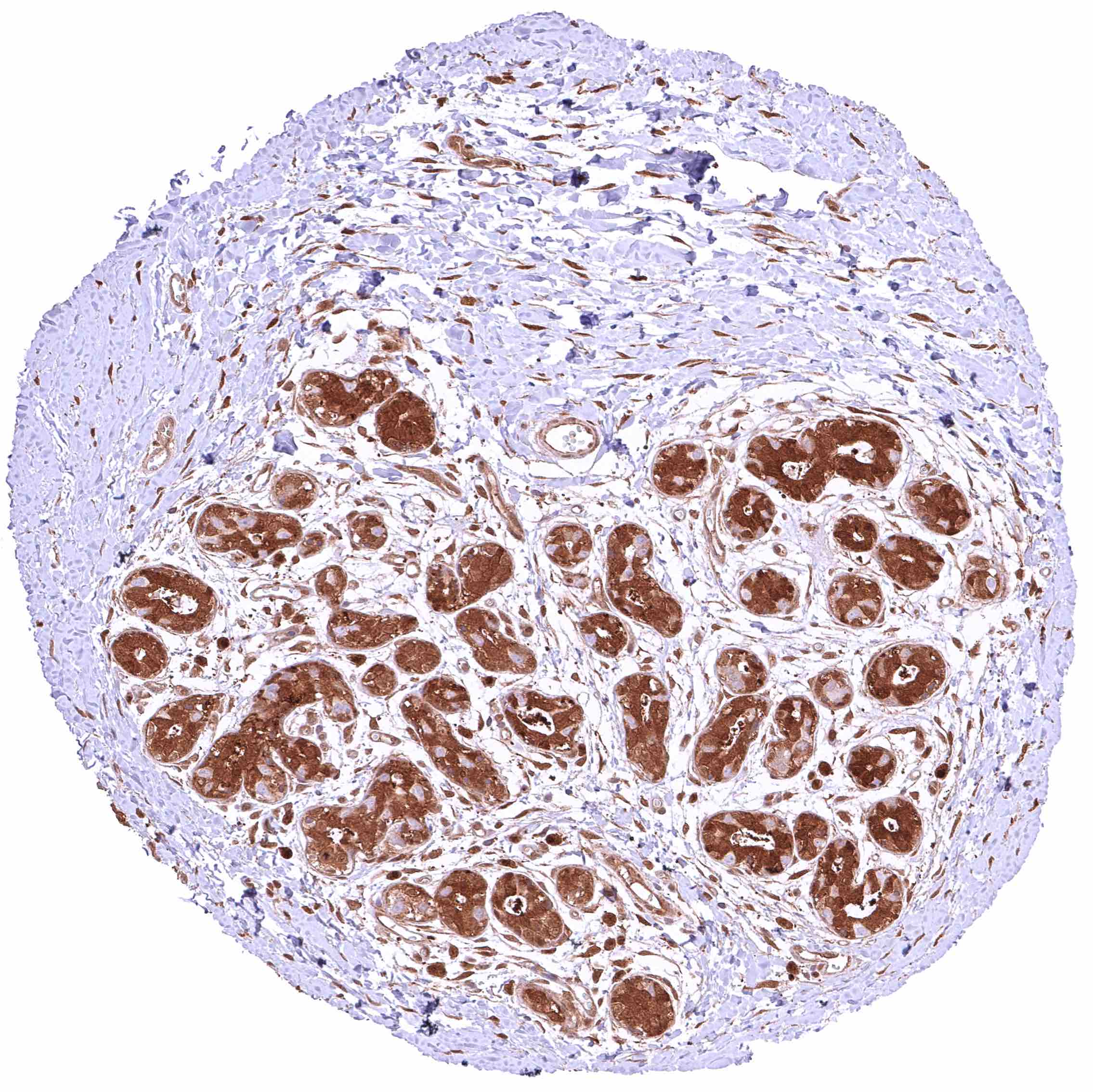
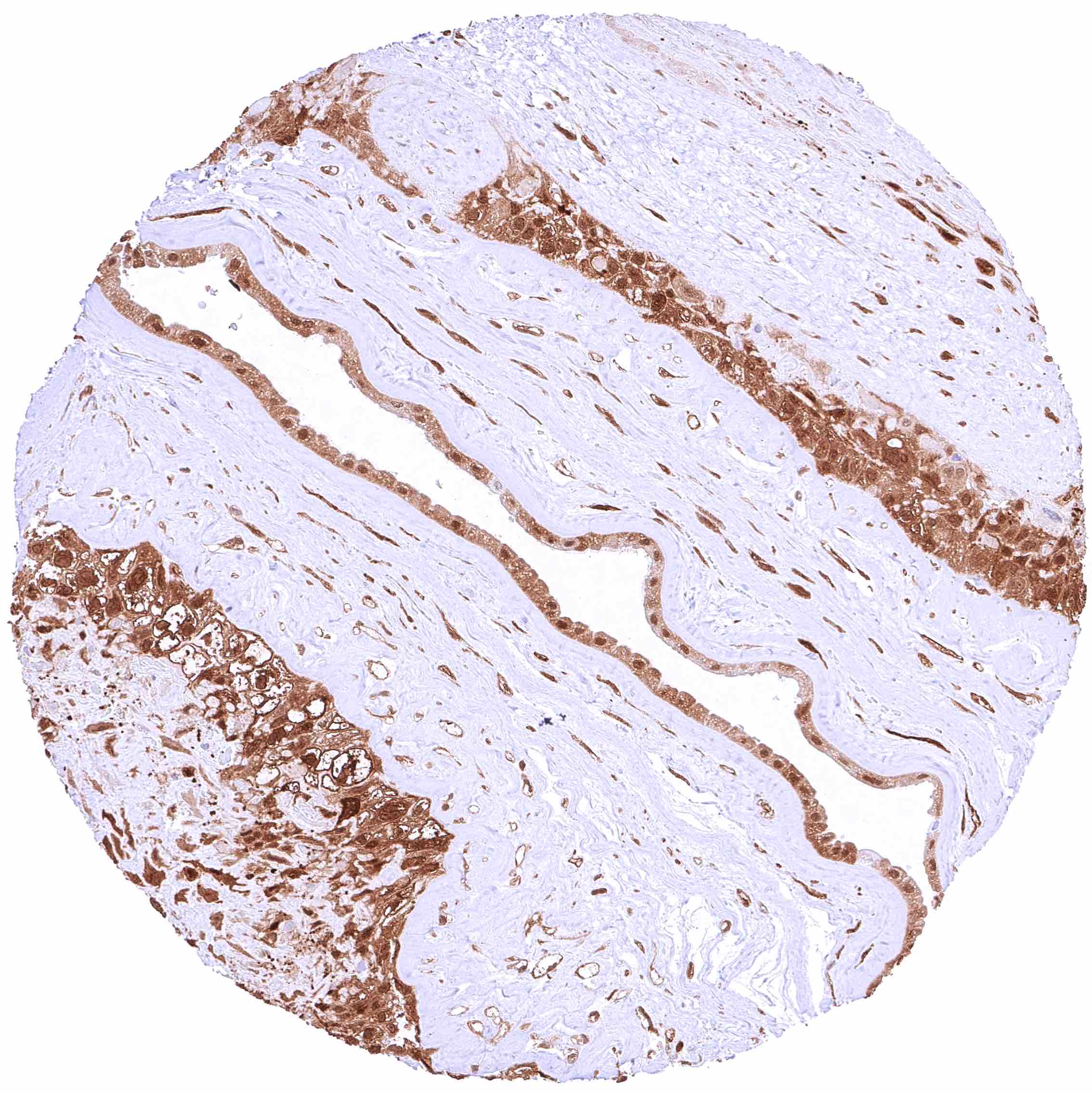
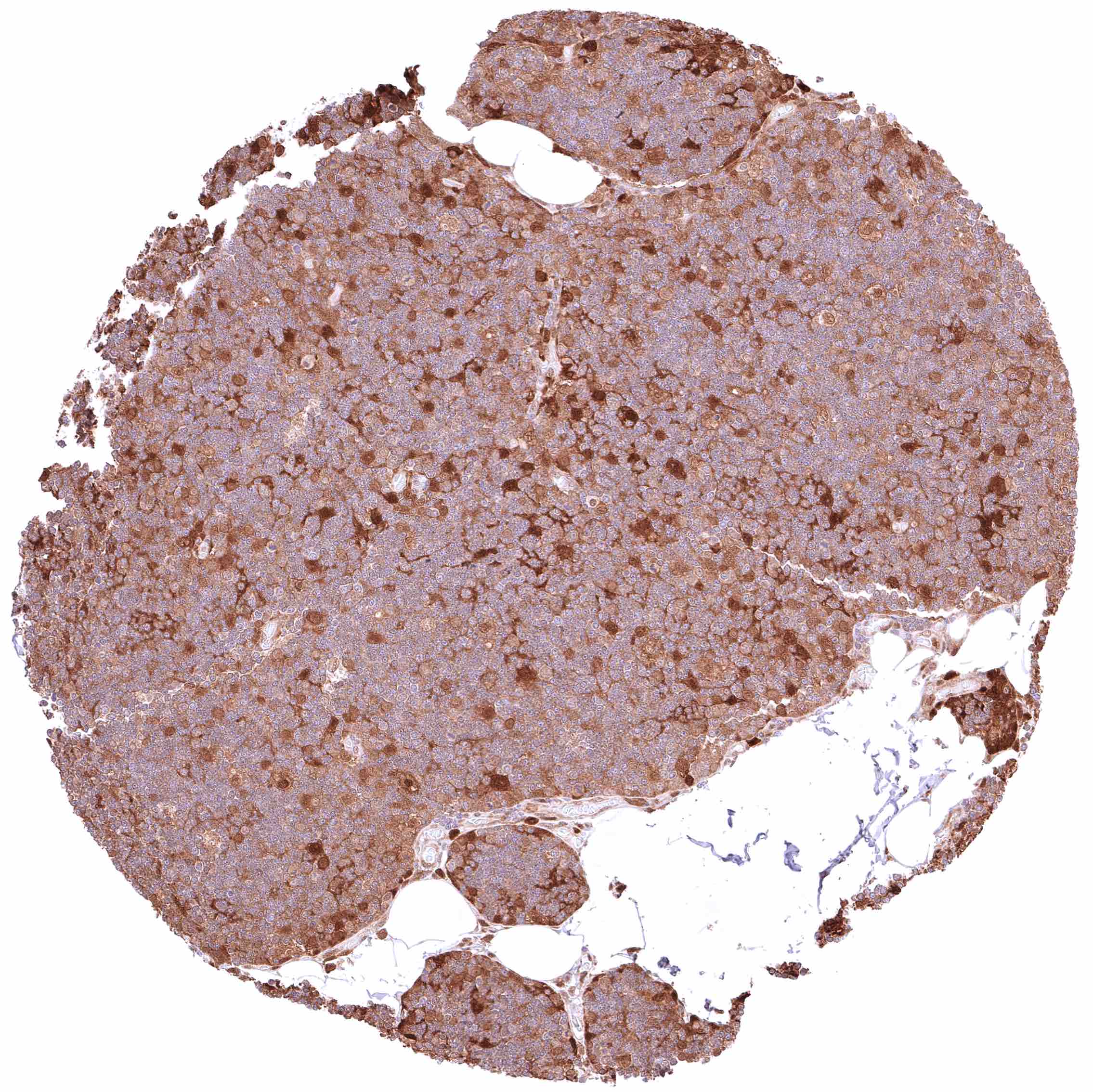
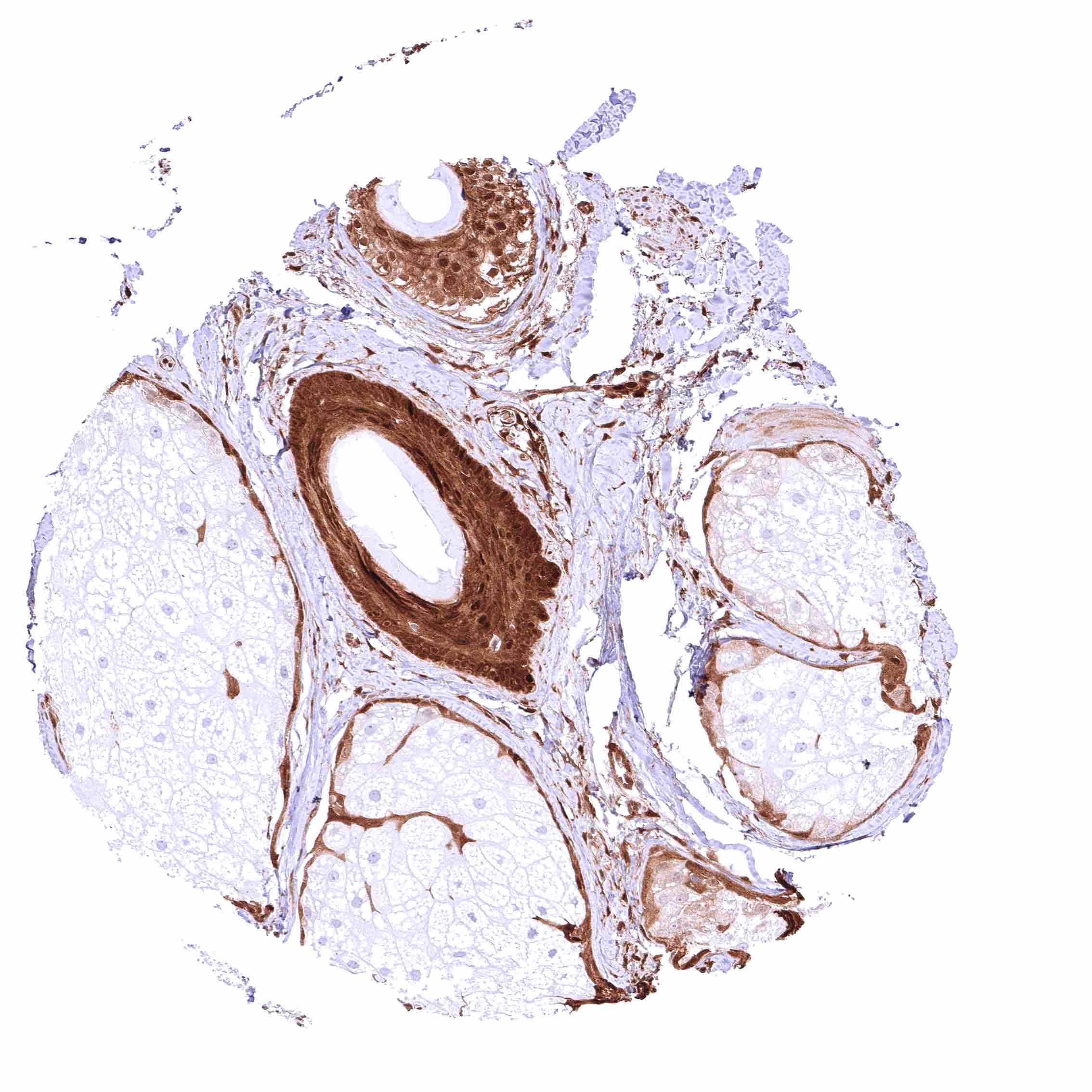
| Male genital | Prostate | Intense nuclear and cytoplasmic GSTP1 staining of basal cells while staining is faint, weak or absent in acinar cells. |
| Seminal vesicles | Intense, predominantly cytoplasmic GSTP1 staining of epithelial cells. | |
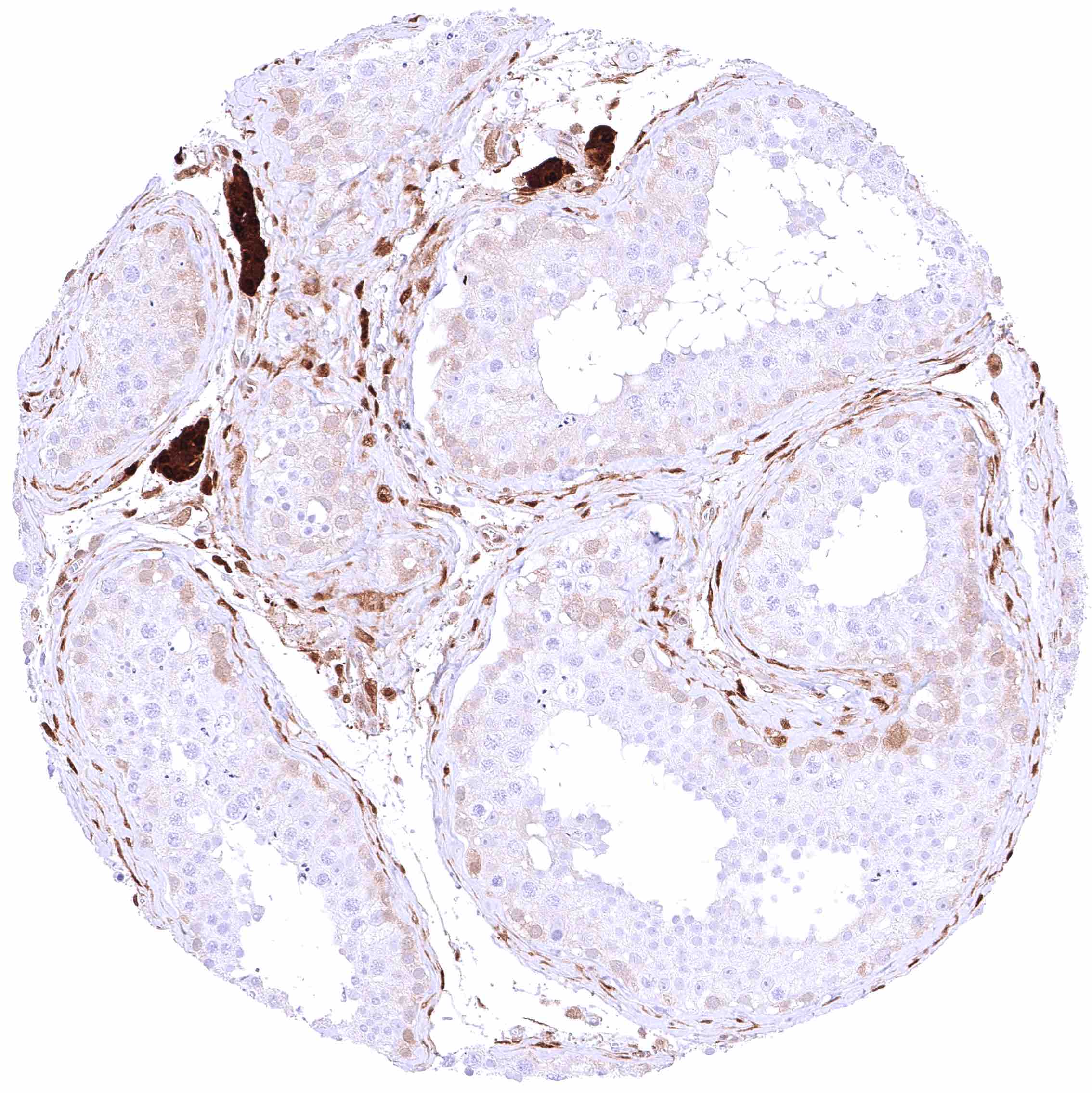
| Testis | Faint cytoplasmic GSTP1 positivity of spermatogonia while maturing germ cells and Sertoli cells are GSTP1 negative. Moderate to strong GSTP1 positivity of Leydig cells. | |
| Epididymis | Intense, predominantly cytoplasmic GSTP1 staining of epithelial cells. | |
| Female genital | Breast | Moderate to strong, nuclear and cytoplasmic GSTP1 positivity of most luminal epithelial cells, however, some of them may remain negative, at least in some samples. Staining is somewhat less intense in basal/myoepithelial cells. |
| Uterus, myometrium | Distinct, nuclear and cytoplasmic GSTP1 positivity of muscle cells. | |
| Uterus, ectocervix | Cytoplasmic and nuclear GSTP1 positivity of variable intensity of squamous epithelial cells. Staining intensity is highest in the basal and suprabasal cell layers and decreases towards the surface. | |
| Uterus endocervix | Strong, nuclear and cytoplasmic GSTP1 positivity of epithelial cells. | |
| Uterus, endometrium | Strong, predominantly cytoplasmic GSTP1 positivity of epithelial cells. However, GSTP1 staining is only faint or absent in certain distinct cell groups. Weak to moderate, predominantly cytoplasmic GSTP1 staining of decidua cells during pregnancy. | |
| Fallopian Tube | Intense, nuclear and cytoplasmic GSTP1 staining of epithelial cells. | |
| Ovary | Intense, predominantly cytoplasmic GSTP1 positivity of stromal cells. Weak to moderate, predominantly cytoplasmic GSTP1 staining of corpus luteum cells. Moderate to strong nuclear and cytoplasmic GSTP1 staining of granulosa cells. | |
| Placenta early | Variable, weak to very intense, nuclear and cytoplasmic GSTP1 positivity of cytotrophoblast and syncytiotrophoblast cells. Significant variability between samples. | |
| Placenta mature | Intense, nuclear and cytoplasmic GSTP1 positivity of cytotrophoblast and syncytiotrophoblast cells. | |
| Amnion | Moderate to strong, nuclear and cytoplasmic GSTP1 positivity of amnion cells. | |
| Chorion | Moderate to strong, nuclear and cytoplasmic GSTP1 positivity of chorion cells. | |
| Skin | Epidermis | Strong nuclear and cytoplasmic GSTP1 positivity of all squamous epithelial cells. |
| Sebaceous glands | Strong GSTP1 positivity of hair follicles, eccrine glands and peripheral germinative cells of sebaceous glands while sebaceous cells remain GSTP1 negative. | |
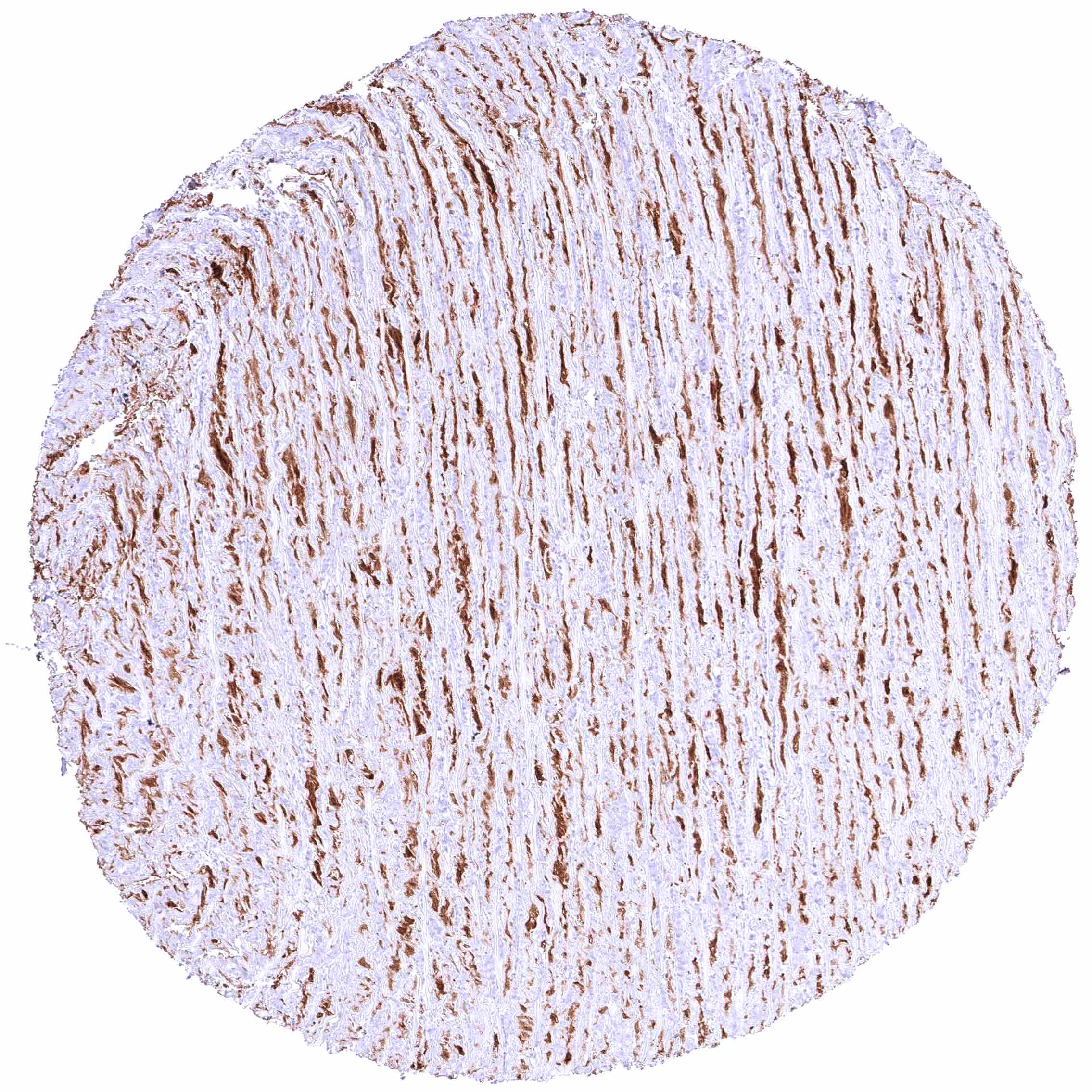
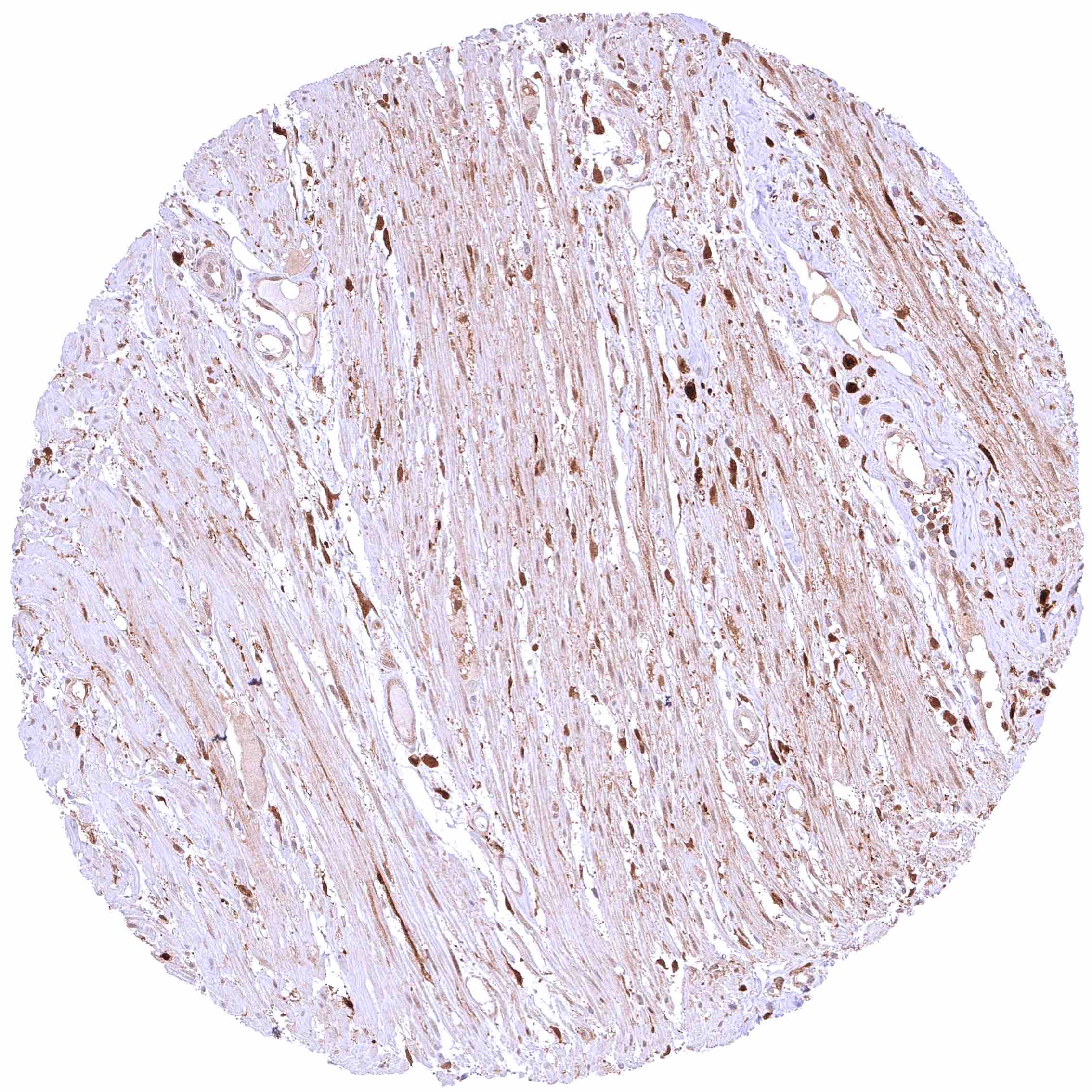
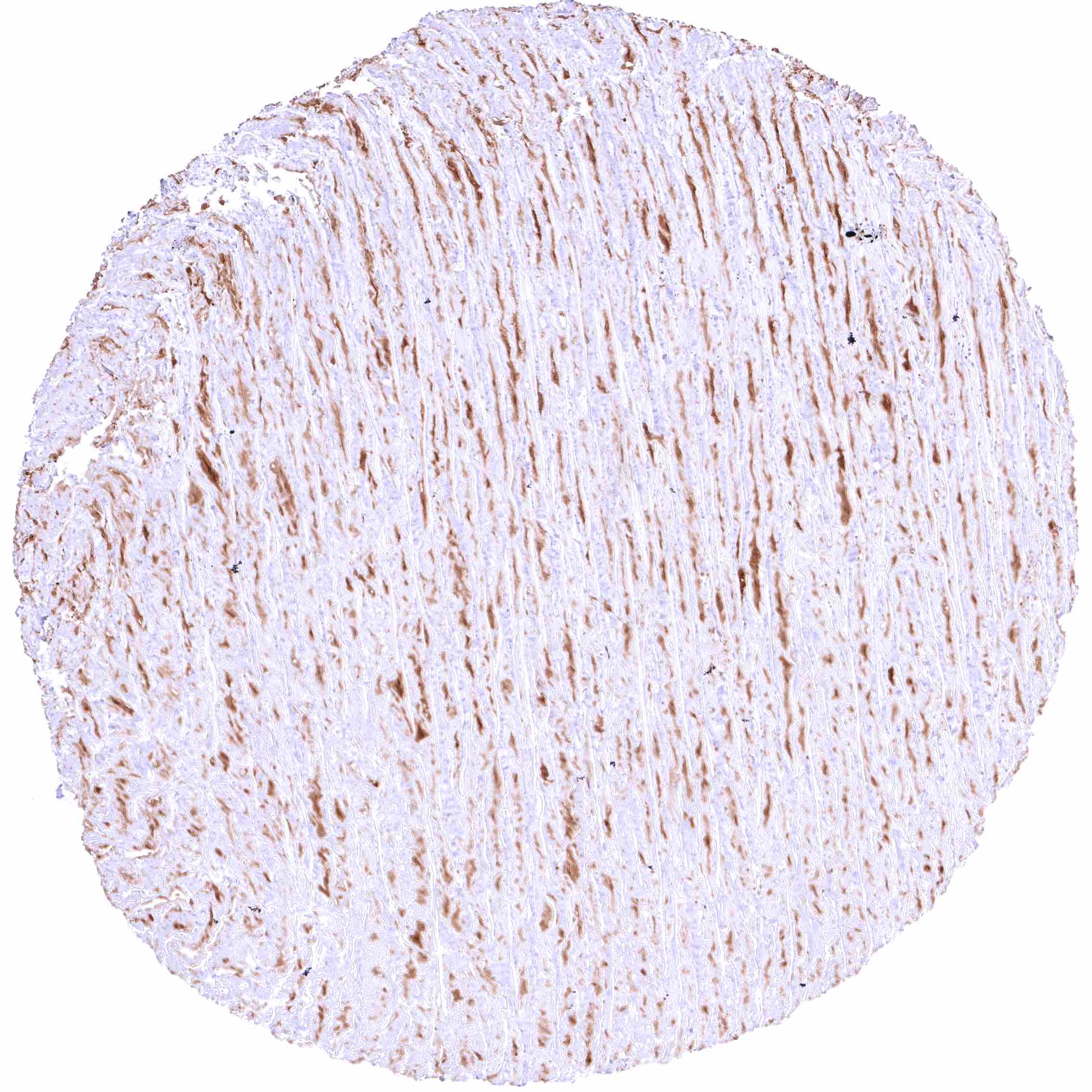
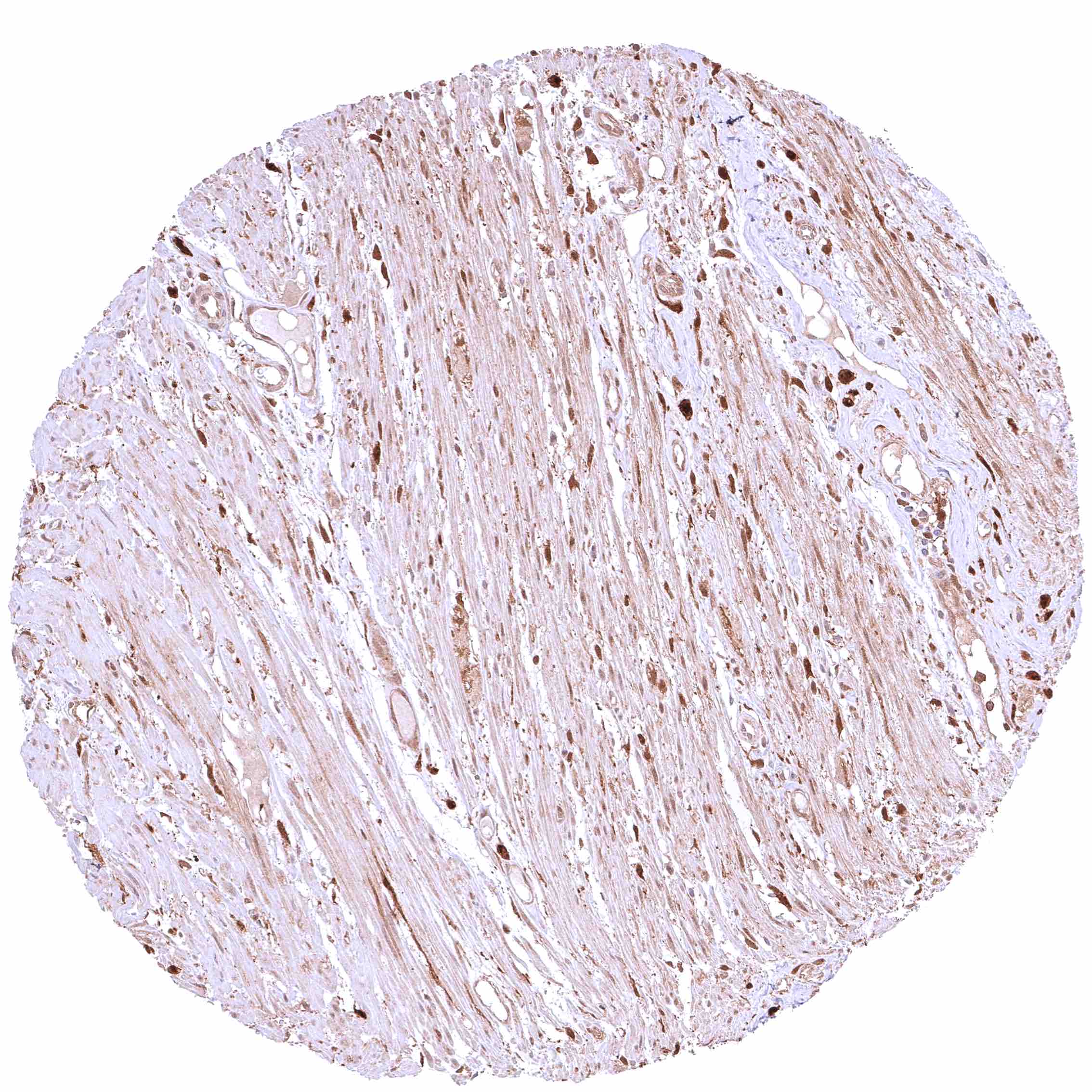
| Muscle/connective tissue | Heart muscle | Most GSTP1 staining occurs around small capillaries while heart muscle cells are GSTP1 negative. |
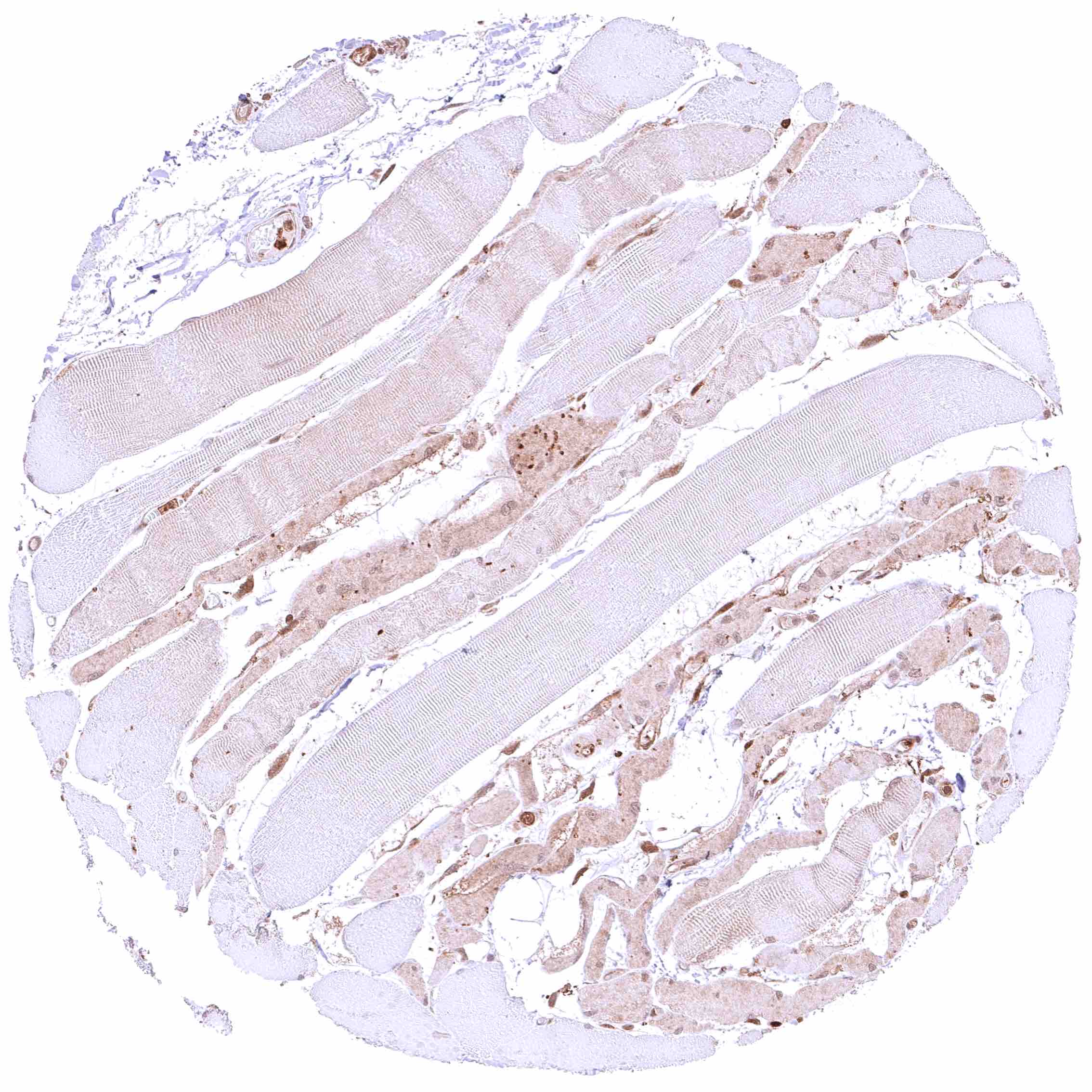
| Skeletal muscle | Most GSTP1 staining occurs around small capillaries while skeletal muscle cells are GSTP1 negative. | |
| Smooth muscle | Weak cytoplasmic GSTP1 positivity of smooth muscle cells in many different organs. | |
| Vessel walls | Distinct granular GSTP1 positivity of (intercellular?) materials in the aortic media. | |
| Fat | Faint or absent GSTP1 staining. | |
| Stroma | Weak to moderate, nuclear and cytoplasmic GSTP1 positivity of many cells. | |
| Endothelium | Weak to moderate (sometimes also strong), GSTP1 positivity. | |
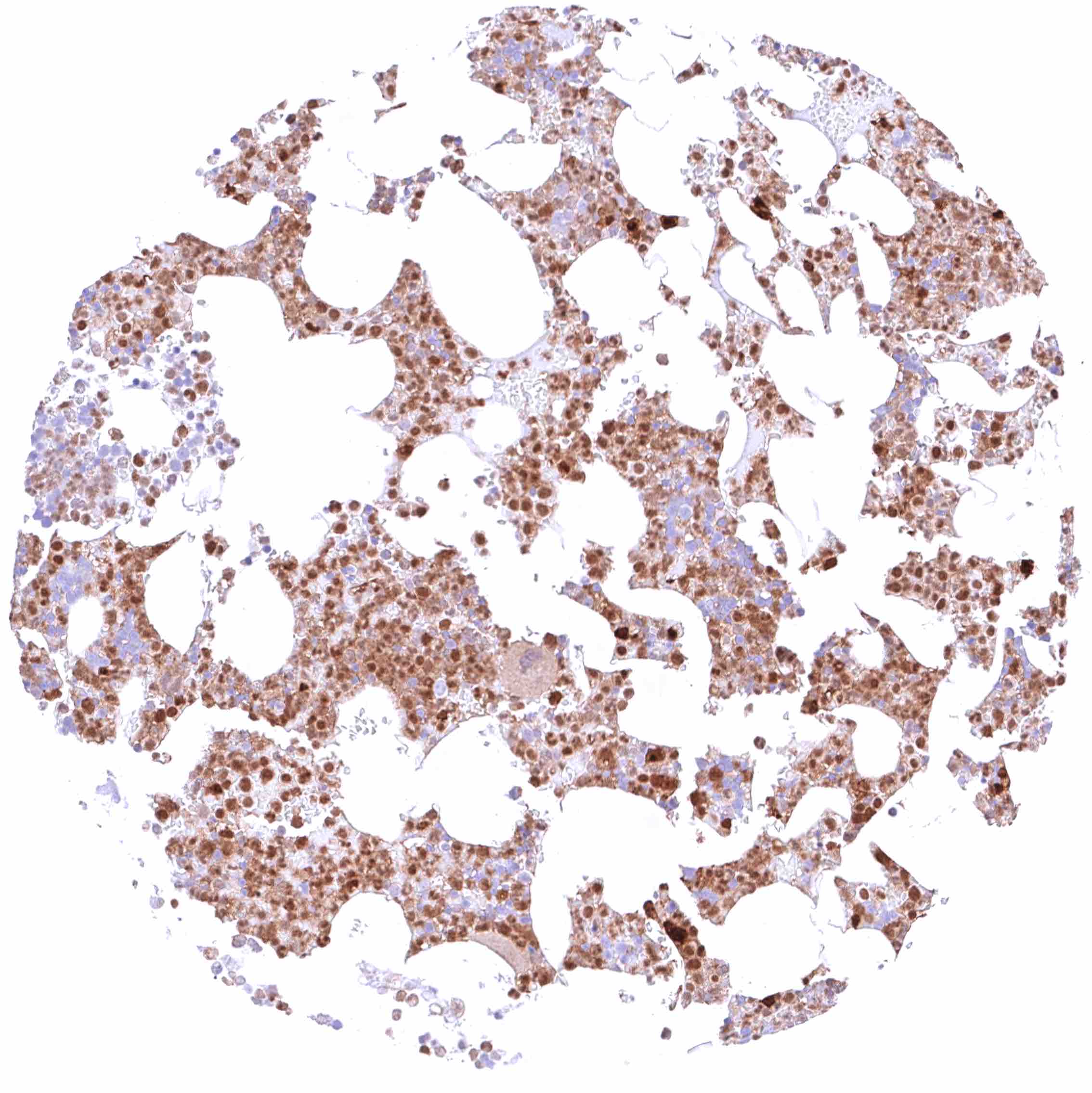
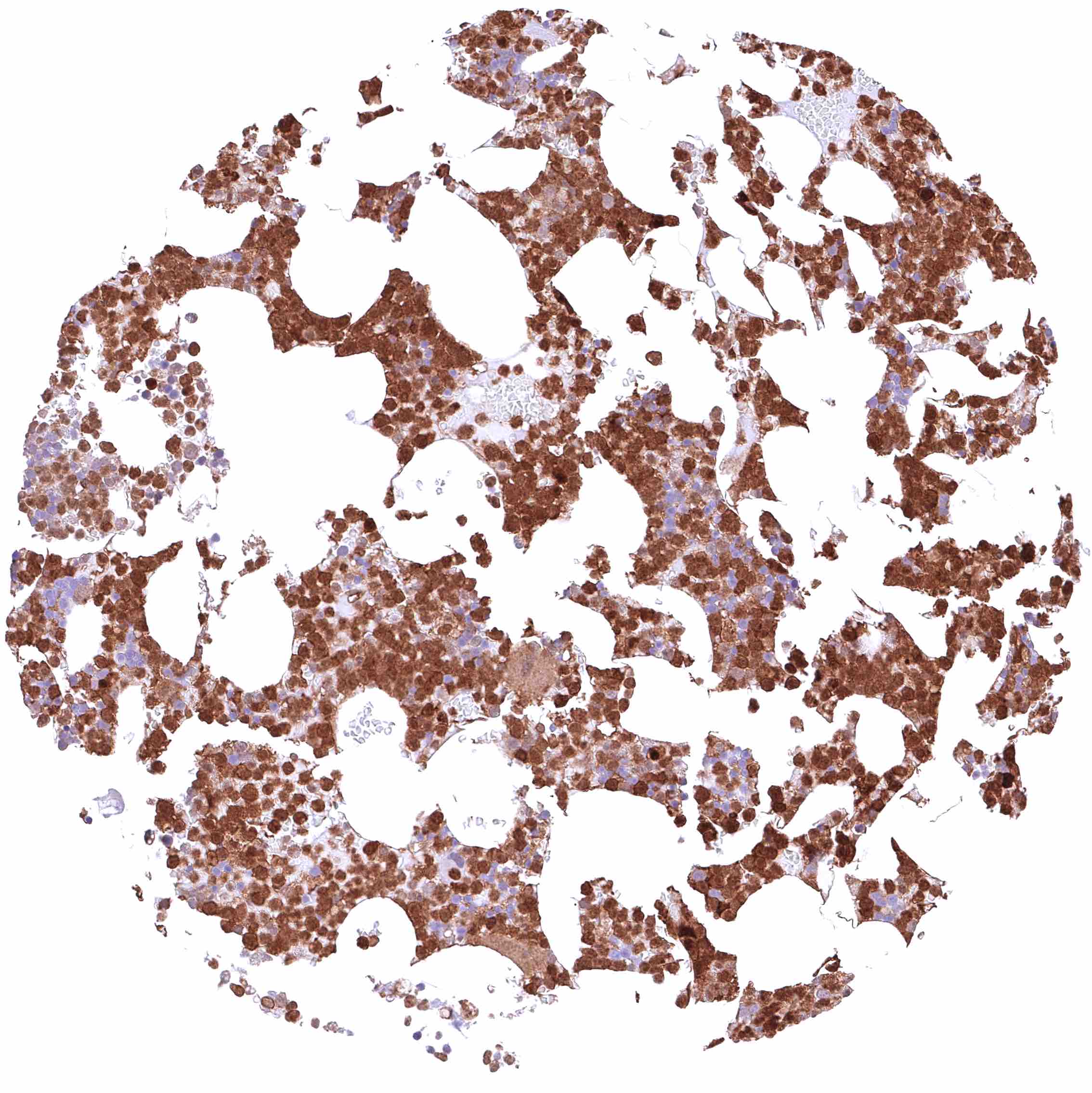
| Bone marrow/ lymphoid tissue | Bone marrow | Moderate to strong, nuclear and cytoplasmic GSTP1 staining of most cell populations although some cell types (erythropoiesis?) remain GSTP1 negative. |
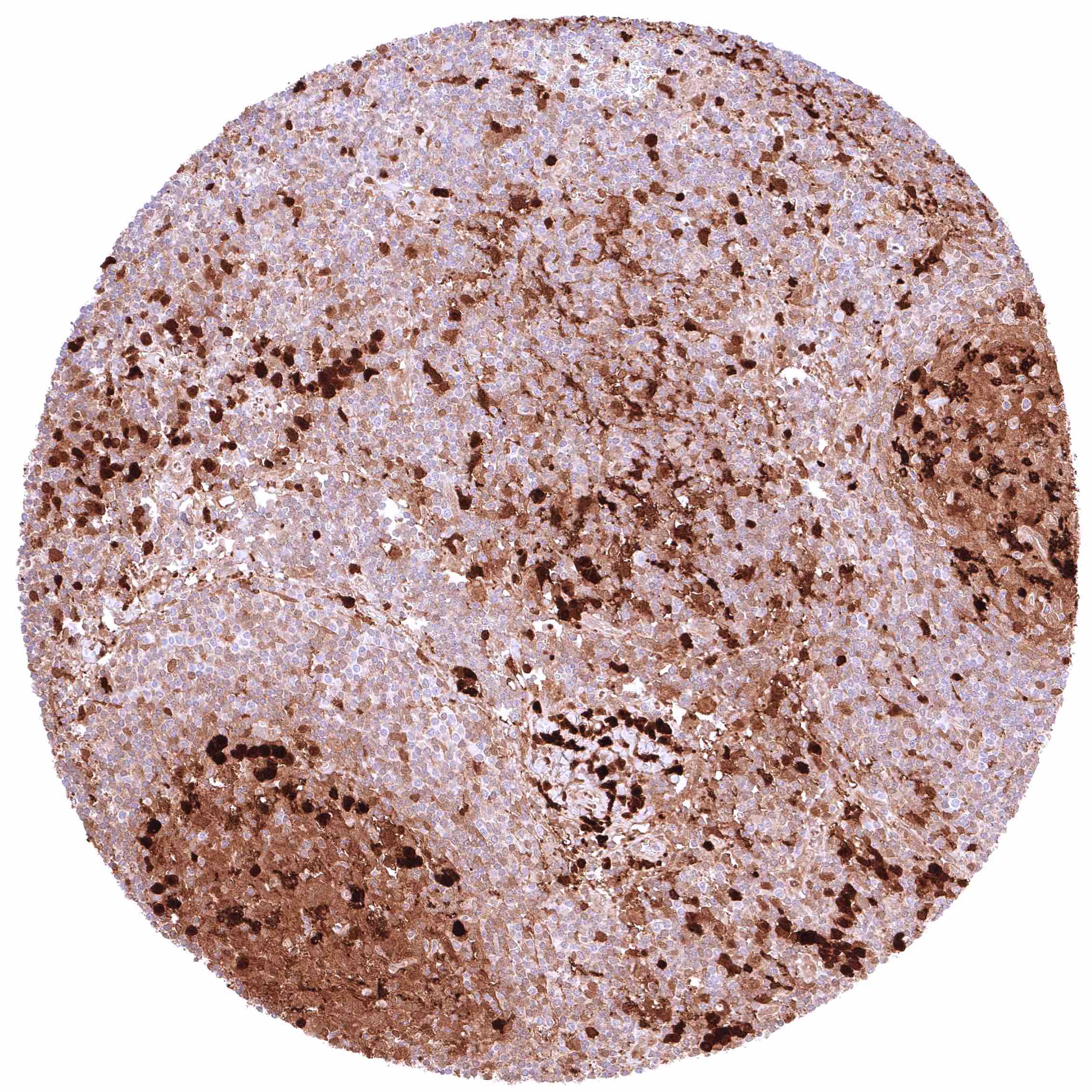
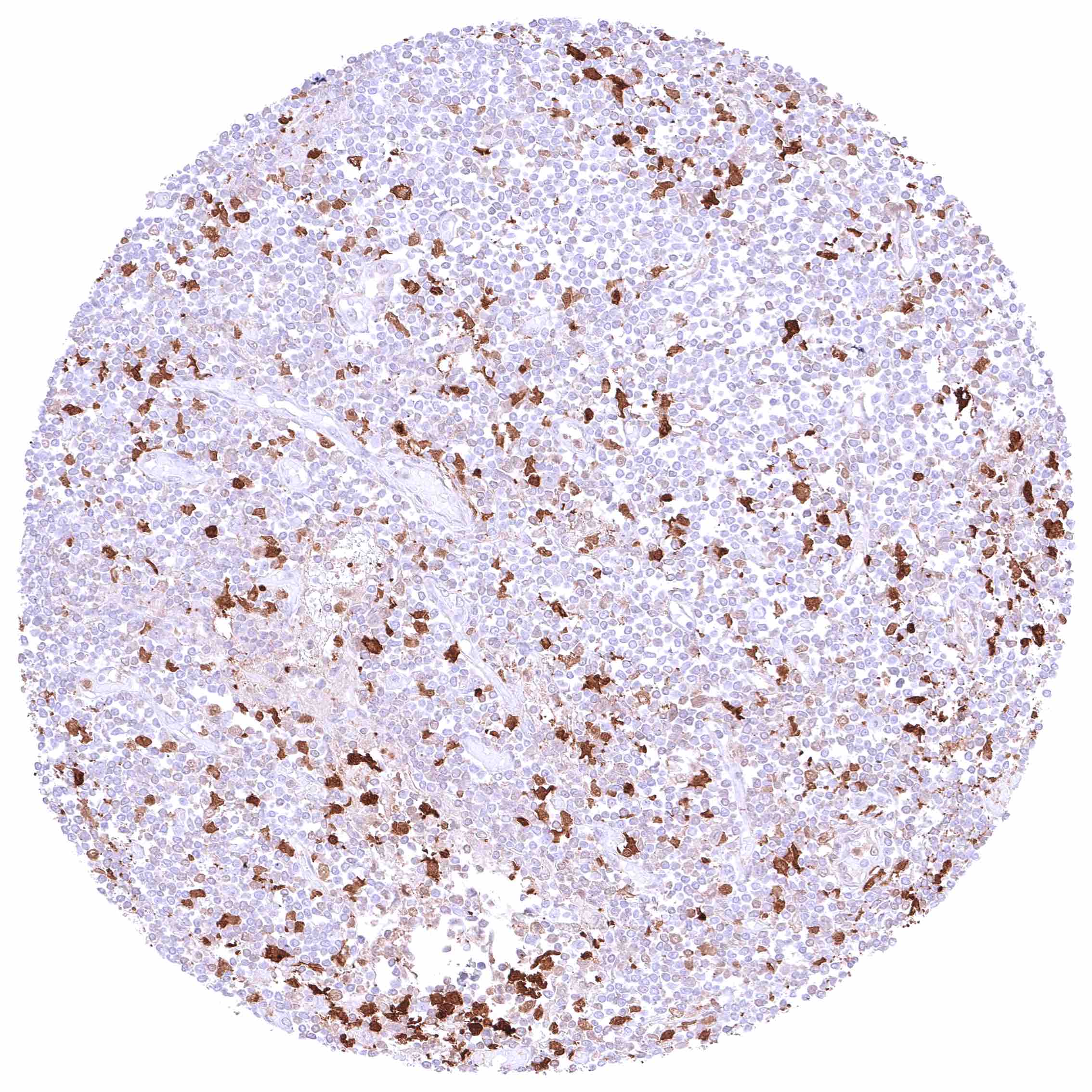
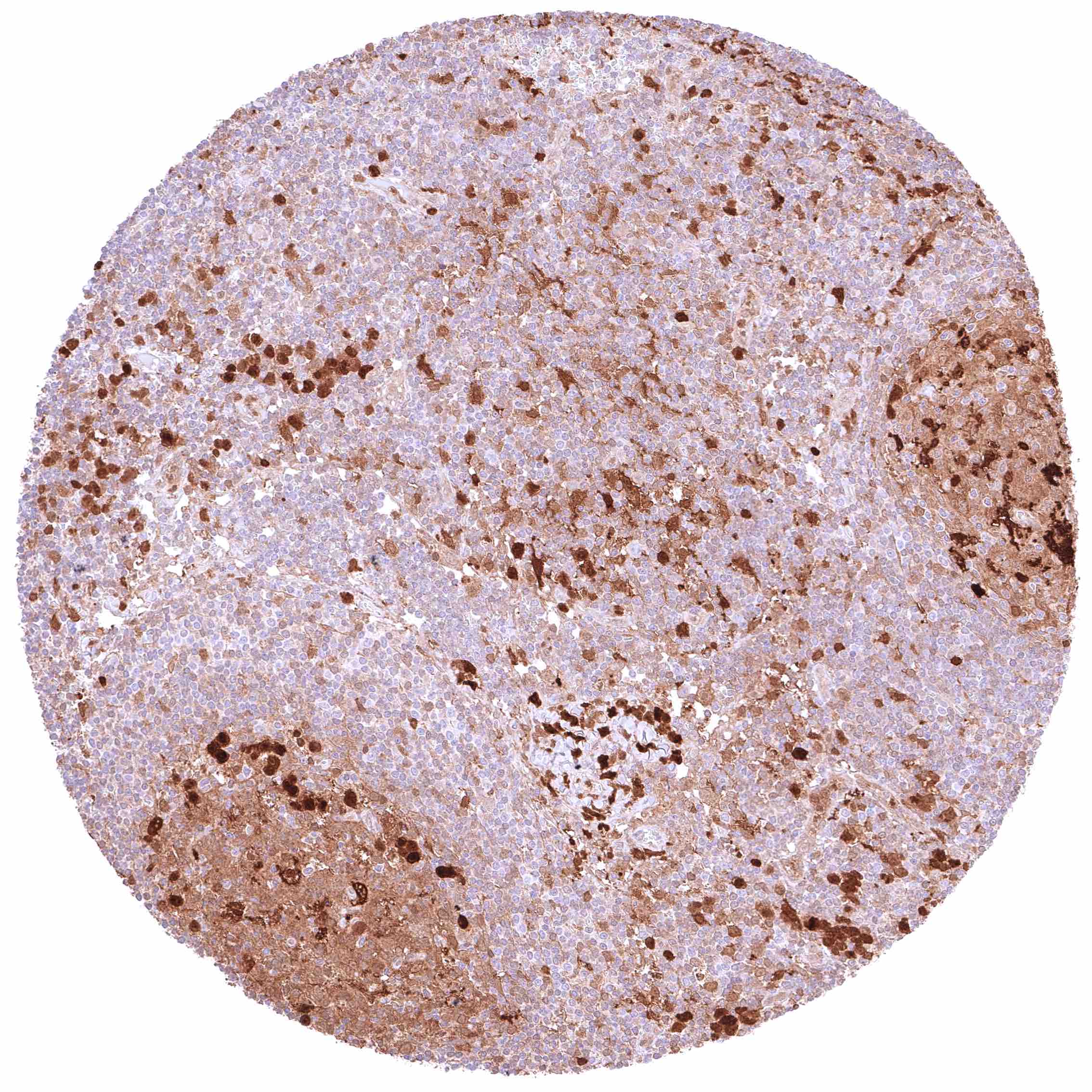
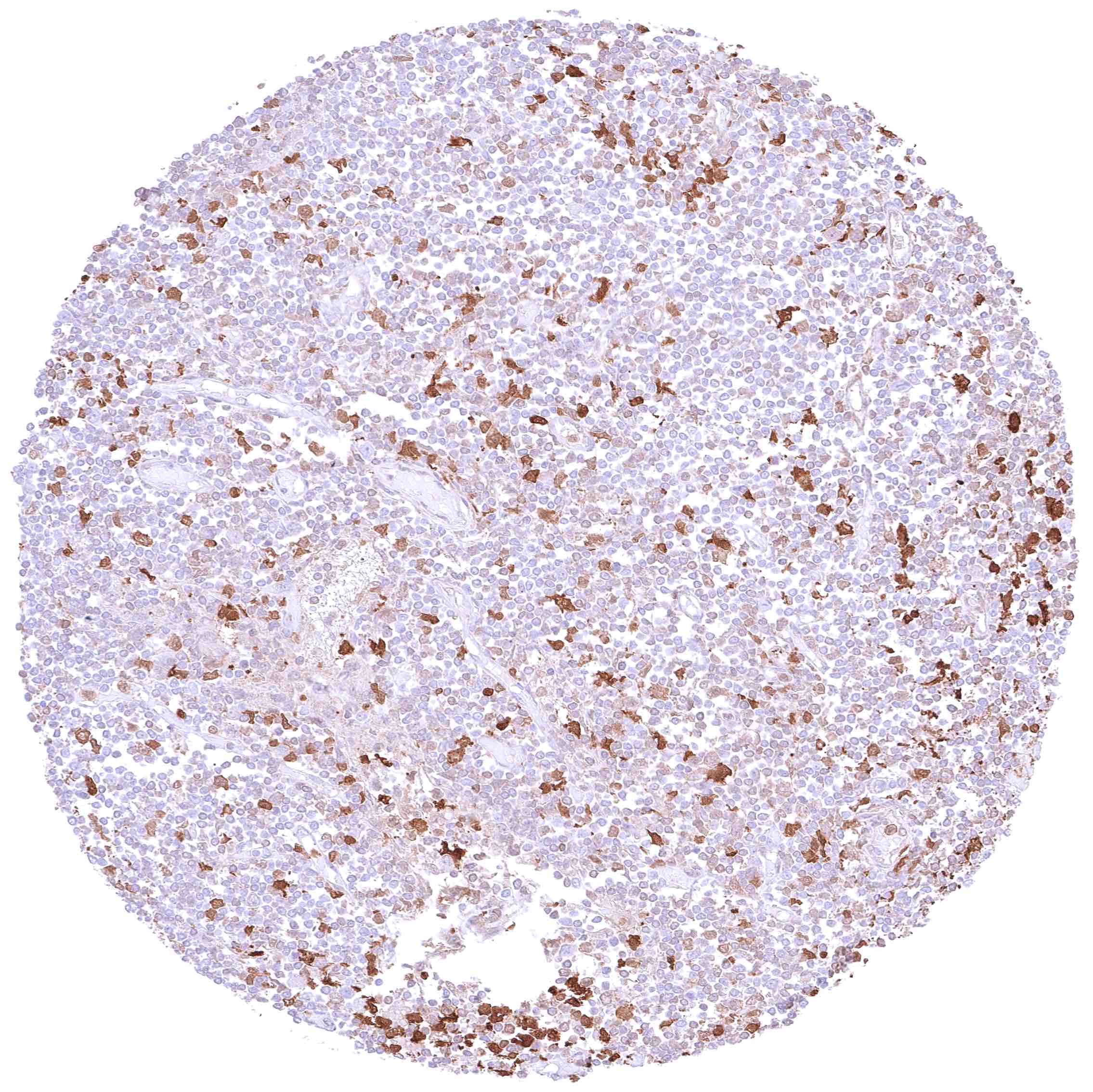
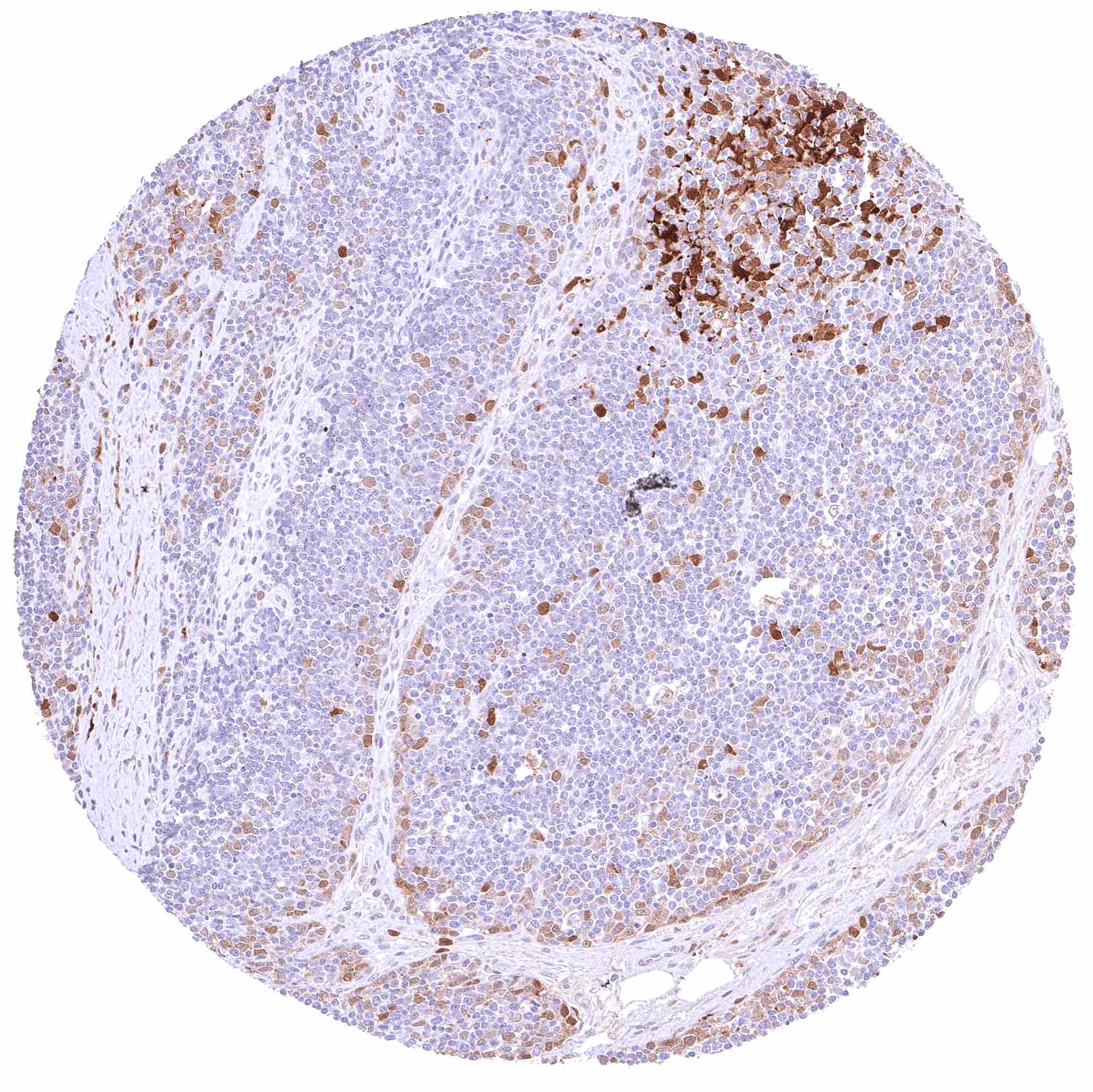
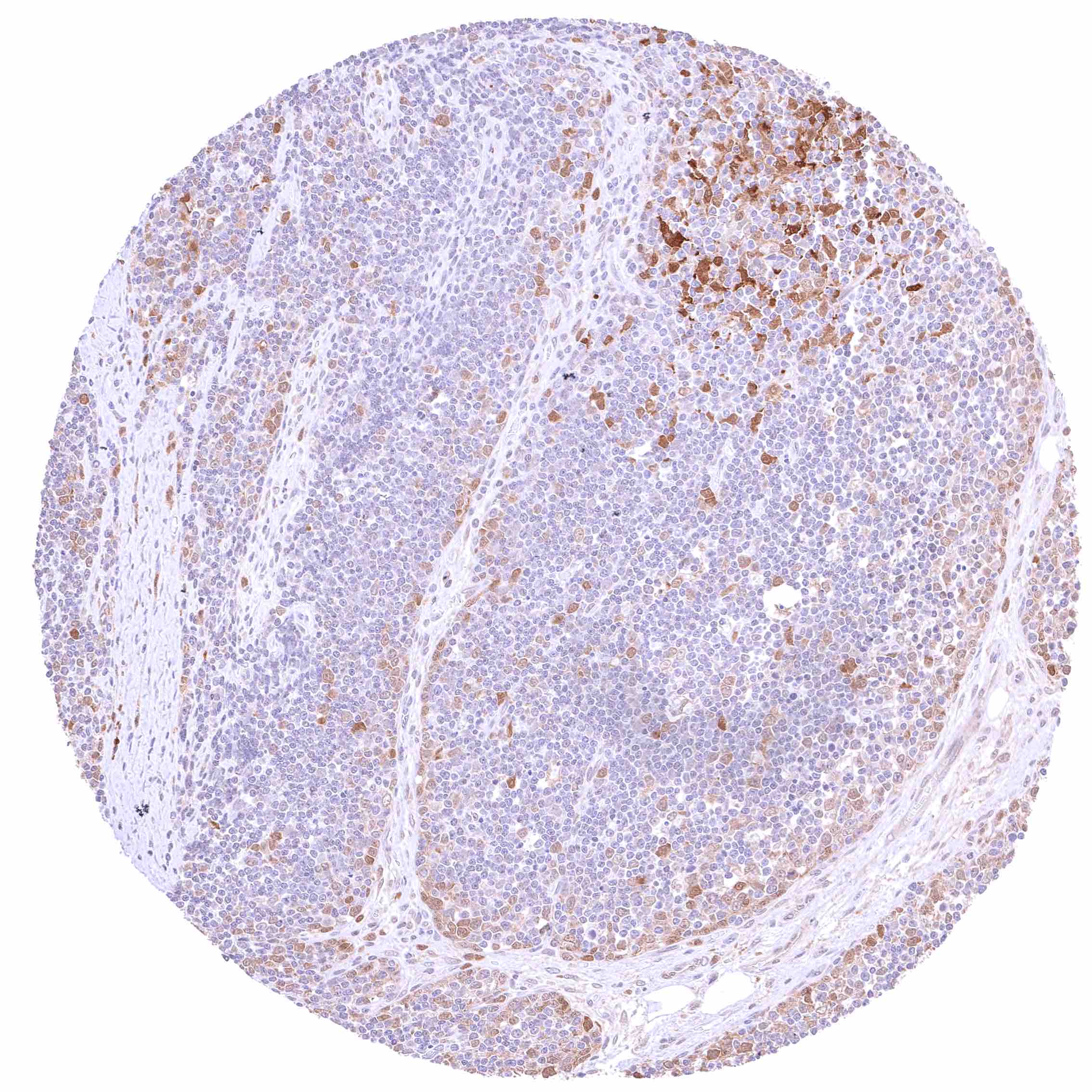
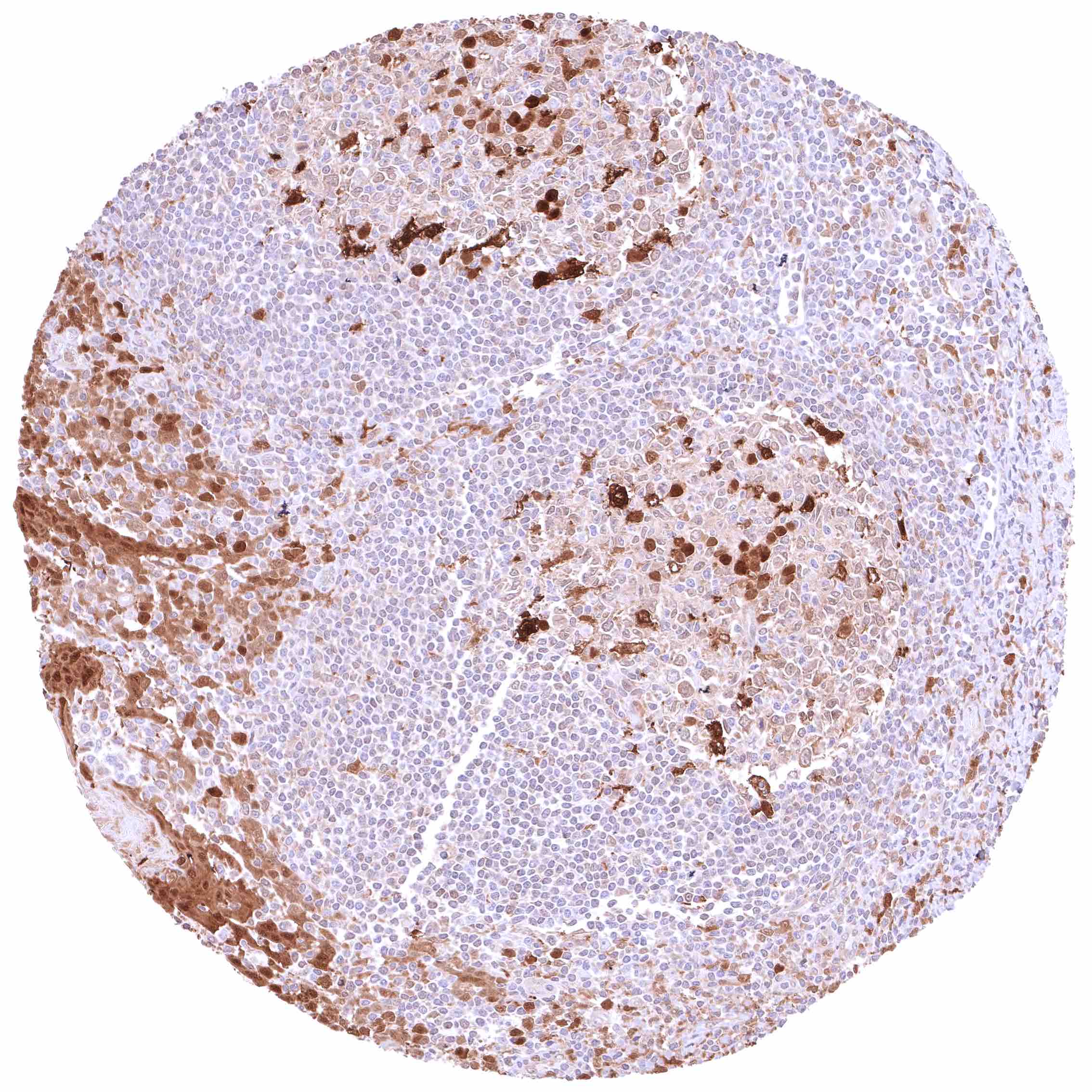
| Lymph node | GSTP1 staining intensity varies markedly between samples. Only few cells are positive in some samples, while all cells show at least some cytoplasmic staining in others. In all cases, staining intensity is highest in a subset of germinal centre cells (dendritic cells?, macrophages?). | |
| Spleen | GSTP1 staining intensity varies markedly between samples. Only few cells are positive in some samples, while all cells show at least some cytoplasmic staining in others. | |
| Thymus | GSTP1 staining intensity varies markedly between samples. Only few cells are positive in some samples, while all cells show at least some cytoplasmic staining in others. Nuclear and cytoplasmic GSTP1 positivity especially involves epithelial cells and also includes corpuscles of Hassall’s. | |
| Tonsil | Strong nuclear and cytoplasmic GSTP1 positivity of all squamous epithelial cells. With respect to lymphatic cells, GSTP1 staining intensity varies markedly between samples. Only few cells are positive in some samples, while all cells show at least some cytoplasmic staining in others. In all cases, staining intensity is highest in a subset of germinal centre cells (dendritic cells?, macrophages?). | |
| Remarks |
The ubiquitous staining of GSTP1 across all tissue types is largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression GSTP1).
Positive control = Prostate: A strong nuclear and cytoplasmic GSTP1 staining should be seen in all basal cells of the prostate.
Negative control = GSTP1 staining must be absent in Sertoli cells and in maturing germ cells (weak positivity should be seen in spermatogonia).
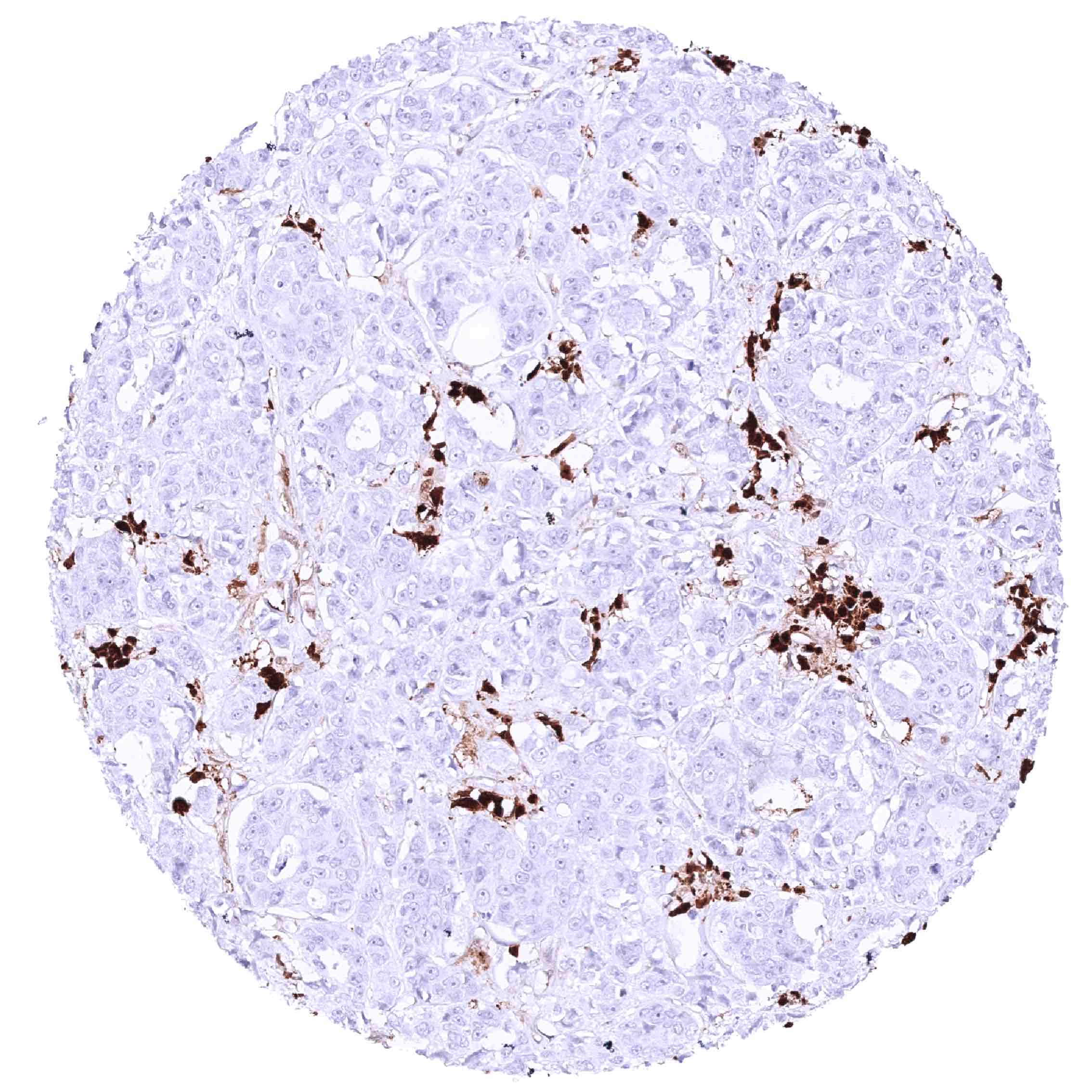
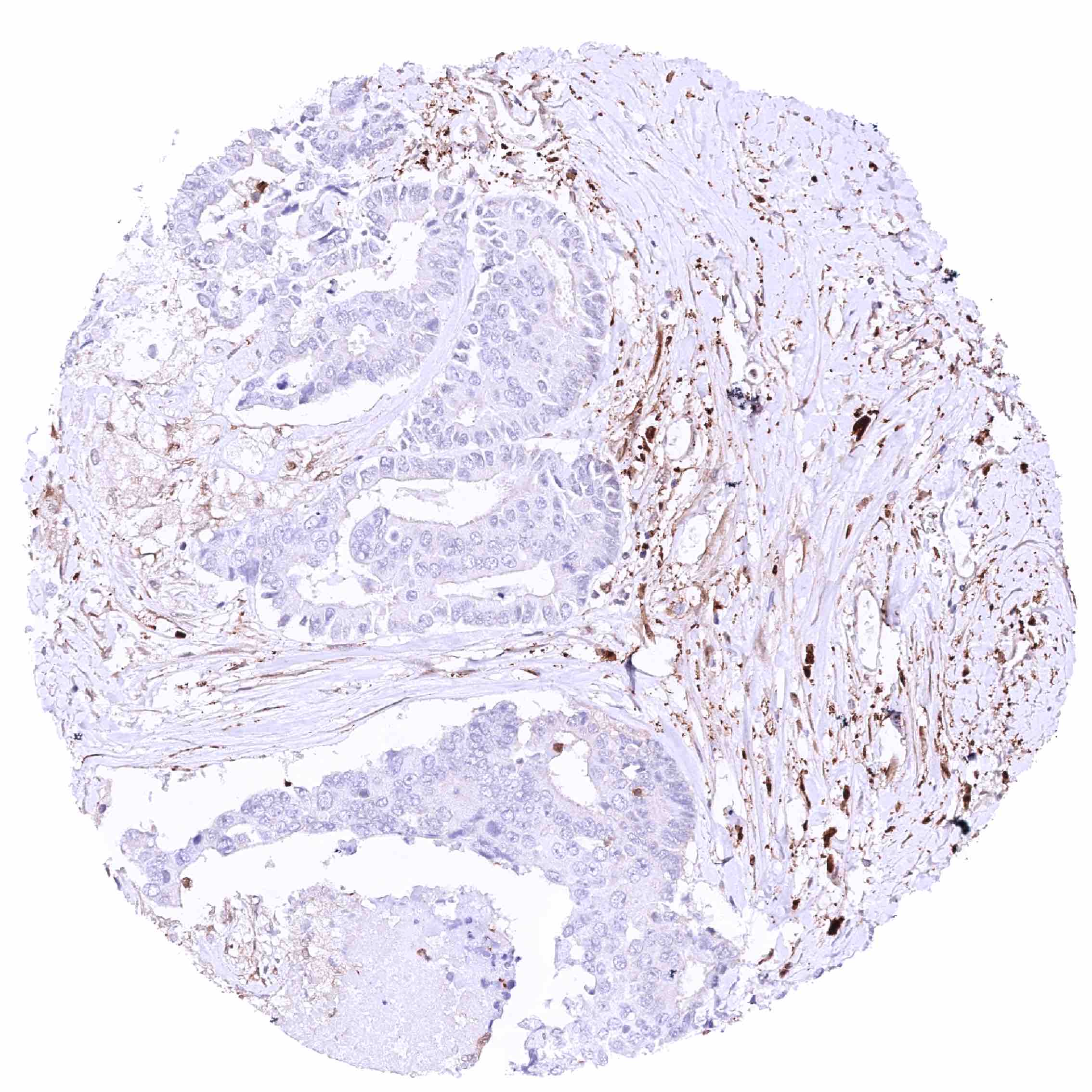
Staining Pattern in Relevant Tumor Types
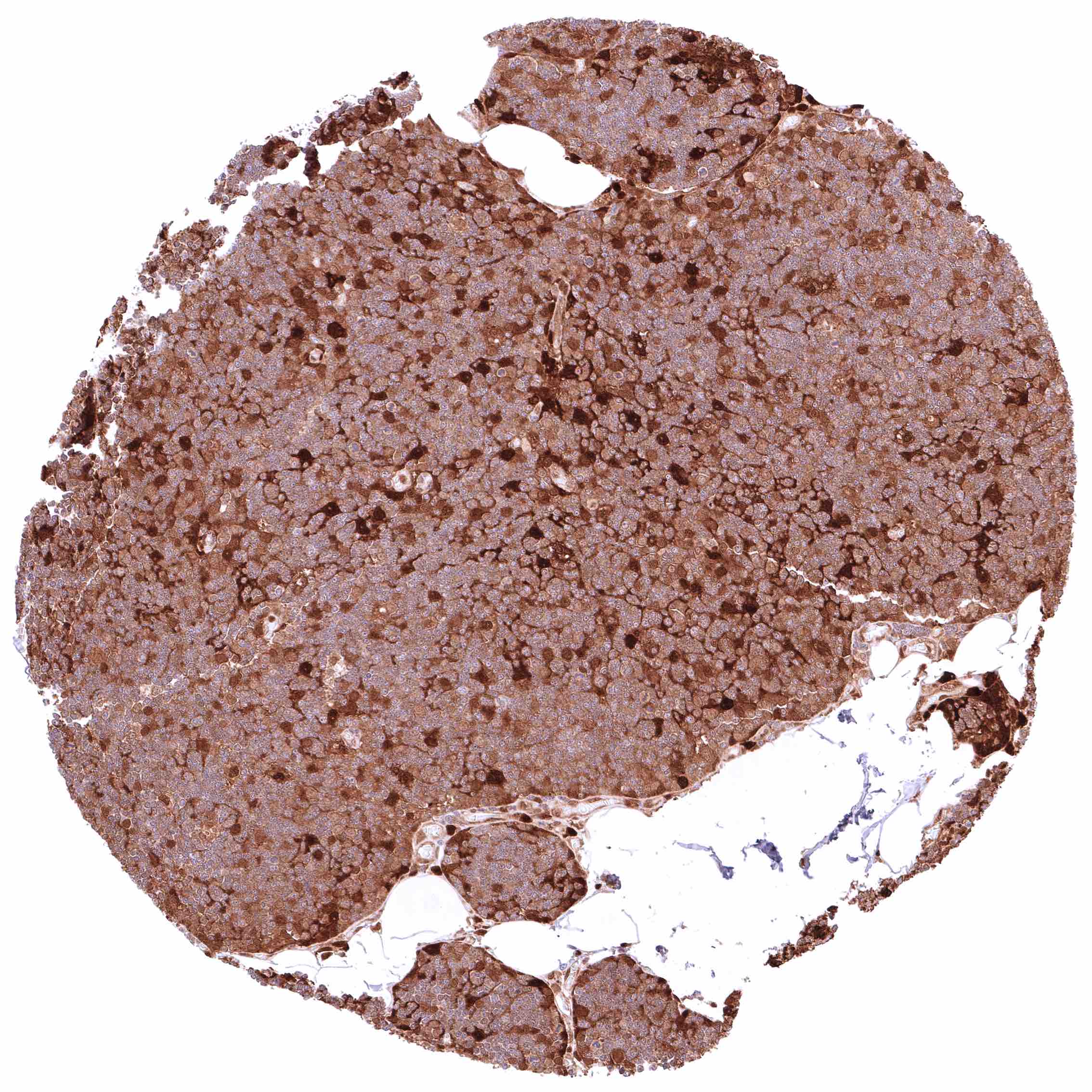
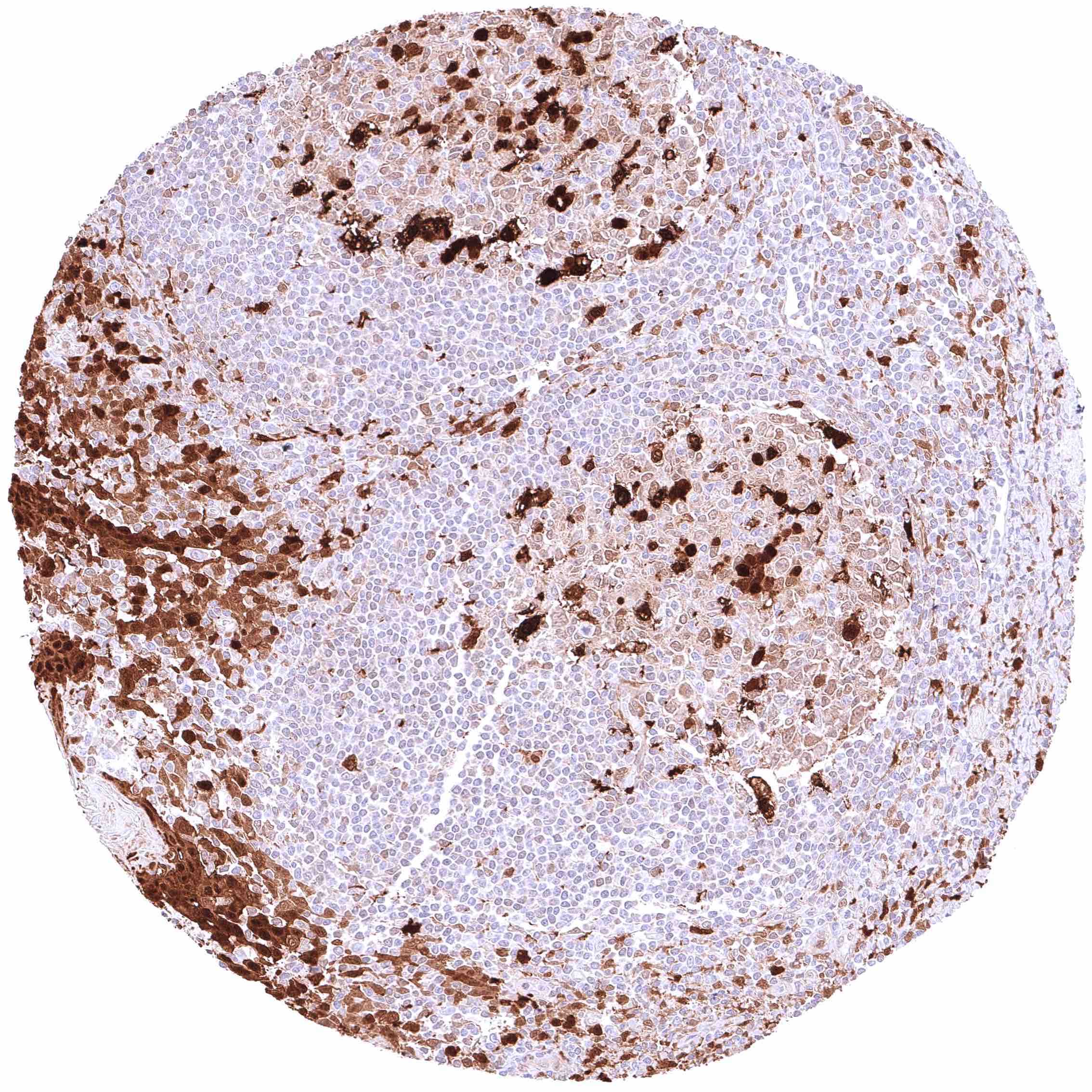
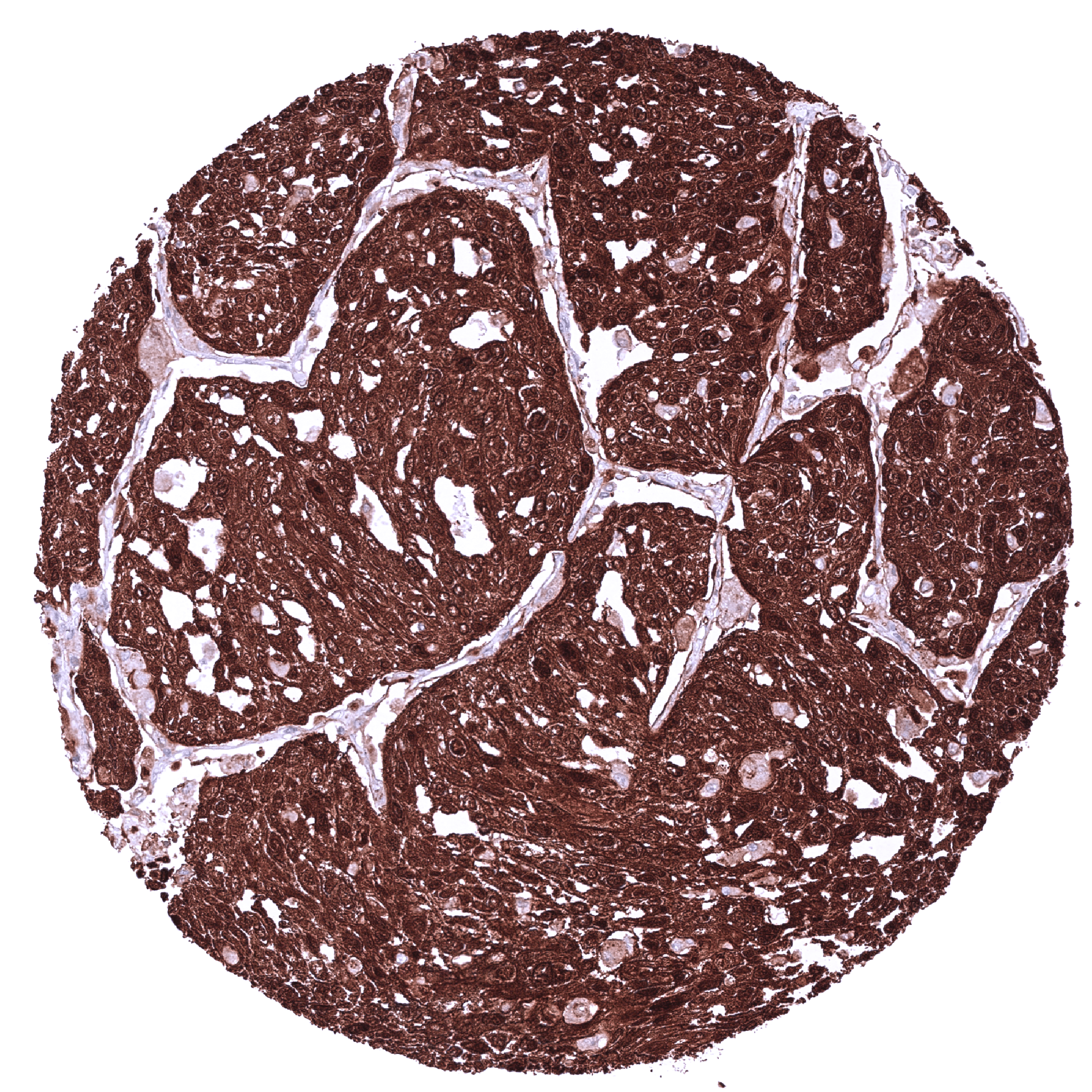
GSTP1 expression levels are highly variable in almost all cancer types. Types of aberrant expression vary from massive overexpression to complete loss of expression.
The TCGA findings on GSTP1 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.
It is of note, however, that RNA expression data have limited value for ubiquitously expressed proteins as the RNA levels reflect the protein quantity in both cancer cells and tumor stroma.
Compatibility of Antibodies
No data available at the moment
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply MSVA-685R at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The diagnostic utility of GSTP1 IHC for cancer and preneoplastic disease needs to be investigated.
- The prognostic relevance of GSTP1 expression in tumors should be explored further.
- The predictive role of increased and/or reduced or absent GSTP1 expression for cancer treatments needs to be evaluated.
- The interaction of GSTP1 with other cellular pathways needs to be better understood.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For GSTP, orthogonal validation is not well suited due to the ubiquitous expression of the protein. Ubiquitous GSTP1 protein expression seen by the antibody MSVA-685R is consistent, however, with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression GSTP1). Also in line with the summarized RNA data, GSTP1 immunostaining by MSVA-685R was largely absent in the testis and in the liver. These two organs exhibit – by far – the lowest levels of GSTP1 RNA expression (close to zero).
Comparison of antibodies: True GSTP1 protein expression in all cell types found by MSVA-685R is corroborated by identical stainings obtained by another commercially available independent antibody (termed “validation antibody”). The similarity of staining also includes the same variability of staining patterns between different cell types in individual tissues such as variations between different renal tubuli, different layers of squamous epithelium, and surface versus crypt differences in the intestinal epithelium staining. Additional cytoplasmic stainings seen in skeletal muscle and in maturing germ cells of the testis which were only observed by the validation antibody but not by MSVA-685R were considered cross-reactivities of the validation antibody.