


295,00 € – 995,00 €
Product details
Synonyms = claudin 3,C7orf1,CPE-R2,CPETR2,HRVP1,RVP1
Antibody type = Recombinant Rabbit monoclonal / IgG
Clone = HMV309
Positive control = Liver: A strong membranous CLDN3 staining should be seen in bile ducts. In addition, a weak to moderate membranous CLDN3 staining should be seen in hepatocytes (often seen predominantly at the bile secreting pole).
Negative control = Stomach: Most epithelial cells should be CLDN3 negative, while a strong membranous CLDN3 staining of a small subset of epithelial cells in the neck and in glandular pits must be seen.
Cellular localization = Membraneous
Reactivity = Human
Application = Immunohistochemistry
Dilution = 1:100 – 1:200
Intended Use = Research Use Only
Relevance of Antibody
Claudin 3 is a tight junction protein. Putative drug target.
Biology Behind
Claudin 3 (CLDN3) is a tight-junction (TJ) protein with four-transmembrane domains which is coded by the intron-less CLDN3 gene on chromosome 7q11.23. It is one of at least 27 members of the claudin protein family. Tight junctions (TJs) are cell-cell adhesion structures in epithelial and endothelial tissues that form a continuous seal around cells and act as a physical barrier to prevent (or enable) the passing of water and molecules through the paracellular space. Claudin-3 is a barrier forming and rather ubiquitously expressed TJ protein and also acts as a low-affinity receptor for Clostridium perfringens enterotoxin. Aberrant expression has been described to occur in cancer and was related to poor patient prognosis. Despite the widespread expression of CLDN3 in normal cells, it is considered a putative drug target, since the accessibility to TJ proteins is limited by the orchestrated cell growth in normal tissues, and the lower level of orientation may result in higher drug exposure of cancer cells.
Staining Pattern in Normal Tissues
Images describing the Claudin 3 staining pattern in normal tissues obtained by the antibody HMV309 are shown in our “Normal Tissue Gallery”.
| Brain | Cerebrum | Negative. |
| Cerebellum | Negative. | |
| Endocrine Tissues | Thyroid | Moderate to strong membranous CLDN3 staining of follicular epithelial cells. |
| Parathyroid | Weak to moderate membranous CLDN3 staining of epithelial cells | |
| Adrenal gland | A faint membranous CLDN3 staining of few epithelial cells can be seen in some samples. | |
| Pituitary gland | ||
| Respiratory system | Respiratory epithelium | Strong membranous CLDN3 staining of respiratory epithelial cells. |
| Lung | CLDN3 staining is only faint in regular pneumocytes. Strong membranous CLDN3 staining of bronchiolized alveolar cell. | |
| Gastrointestinal Tract | Salivary glands | Strong membranous CLDN3 staining of glandular cells. CLDN3 staining is only very faint in excretory duct cells. |
| Esophagus | Negative. | |
| Stomach | Strong membranous CLDN3 staining of a small subset of epithelial cells in the neck and in glandular pits. | |
| Duodenum | Strong membranous CLDN3 staining of all epithelial cells. | |
| Small intestine | Strong membranous CLDN3 staining of all epithelial cells. | |
| Appendix | Strong membranous CLDN3 staining of all epithelial cells. | |
| Colon | Strong membranous CLDN3 staining of all epithelial cells. | |
| Rectum | Strong membranous CLDN3 staining of all epithelial cells. | |
| Liver | Strong membranous CLDN3 staining of bile ducts. Weak to moderate membranous CLDN3 staining of hepatocytes, sometimes predominantly at the bile secreting pole. | |
| Gallbladder | Moderate to strong membranous CLDN3 staining of epithelial cells. | |
| Pancreas | Strong membranous CLDN3 staining of acinar cells. Staining is weaker in cells of islets of Langerhans. | |
| Genitourinary | Kidney | A strong membranous CLDN3 staining preferentially occurs in collecting ducts but can also be seen in individual tubular cells. |
| Urothelium | Weak to strong membranous CLDN3 staining of a subset of urothelial cells, predominantly in the upper half of the urothelium. | |
| Male genital | Prostate | Strong membranous CLDN3 staining of basal and acinar epithelial cells. |
| Seminal vesicles | Moderate to strong membranous CLDN3 staining of epithelial cells. | |
| Testis | Negative. | |
| Epididymis | Strong membranous CLDN3 staining of most epithelial cells in the cauda. Faint membranous CLDN3 staining of chief cells in the corpus. | |
| Female genital | Breast | Strong membranous CLDN3 staining of luminal cells. |
| Uterus, myometrium | Negative. | |
| Uterus, ectocervix | Negative. | |
| Uterus endocervix | Strong, predominantly basolateral membranous CLDN3 staining of epithelial cells. | |
| Uterus, endometrium | Strong membranous CLDN3 staining of epithelial cells. | |
| Fallopian Tube | Strong membranous CLDN3 staining of epithelial cells. | |
| Ovary | Weak to moderate, membranous CLDN3 staining of at least a large subset of corpus luteum cells. | |
| Placenta early | Faint to moderate, membranous CLDN3 staining of the surface membrane of the syncytiotrophoblast. | |
| Placenta mature | Usually negative. In some samples, an endothelial CLDN3 staining can occur. | |
| Amnion | Negative. | |
| Chorion | Negative. | |
| Skin | Epidermis | Negative. |
| Sebaceous glands | Negative. | |
| Muscle/connective tissue | Heart muscle | Negative. |
| Skeletal muscle | Negative. | |
| Smooth muscle | Negative. | |
| Vessel walls | Negative. | |
| Fat | Negative. | |
| Stroma | Negative. | |
| Endothelium | Negative. | |
| Bone marrow/ lymphoid tissue | Bone marrow | Distinct membranous CLDN3 staining of megacaryocytes. |
| Lymph node | Strong luminal membranous CLDN3 staining of at least a subset of high endothelial venules. Moderate to strong CLDN3 staining of a subset of (monocytic?) cells in germinal centres. | |
| Spleen | Moderate to strong CLDN3 staining of a subset of cells in the white pulp. | |
| Thymus | Strong membranous CLDN3 staining of cells of corpuscles of Hassall’s. | |
| Tonsil | Strong membranous CLDN3 staining of squamous epithelial cells of the crypts while surface epithelial cells remain unstained. Moderate to strong CLDN3 staining of a subset of (monocytic?) cells in germinal centres. | |
| Remarks |
In normal tissues, CLDN3 is extensively expressed in many epithelial cell types, especially in the intestine, but also in many other tissues. These findings are largely consistent with the RNA data described in the Human Protein Atlas (Tissue expression Claudin 3).
Positive control = Liver: A strong membranous CLDN3 staining should be seen in bile ducts. In addition, a weak to moderate membranous CLDN3 staining should be seen in hepatocytes (often seen predominantly at the bile secreting pole).
Negative control = Stomach: Most epithelial cells should be CLDN3 negative, while a strong membranous CLDN3 staining of a small subset of epithelial cells in the neck and in glandular pits must be seen.



Staining Pattern in Relevant Tumor Types
CLDN3 is most often expressed in ovarian, endometrial, colorectal and prostatic cancer, but can also occur in carcinomas of various other organs.
The TCGA findings on Claudin 3 RNA expression in different tumor categories have been summarized in the Human Protein Atlas.



Compatibility of Antibodies
Claudin 3 (HMV309) publication summary
Relevant publication: Büyücek et al. “Prevalence and clinical significance of Claudin‑3 expression in cancer: a tissue microarray study on 14,966 tumor samples” Published in Biomark Res. 2024 Dec 10;12(1) PMID: 39658782
A total of 12’314 tumors from 133 different tumor categories were successfully analyzed by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7.8 Target Retrieval Solution buffer. HMV309, at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries.
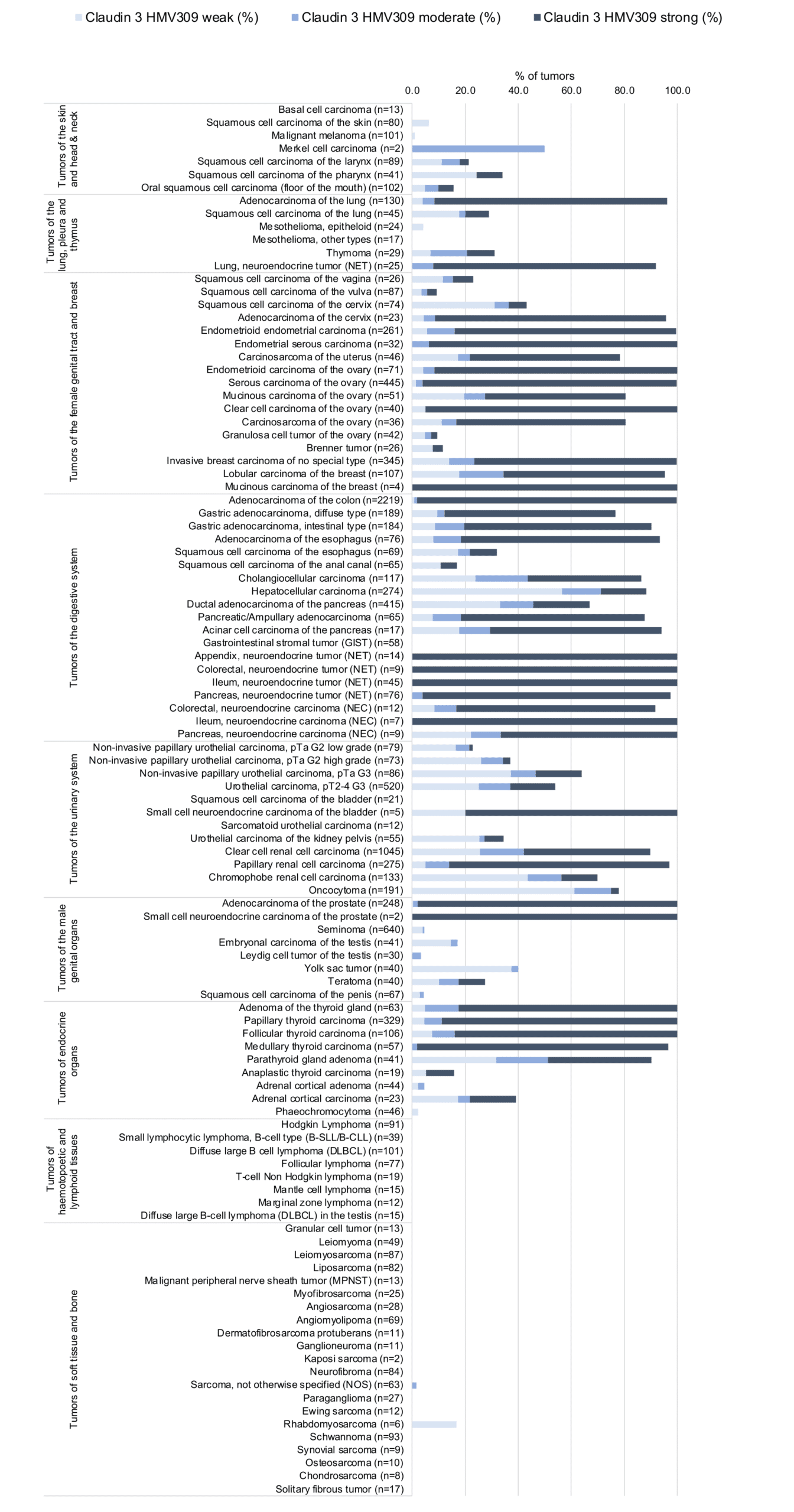
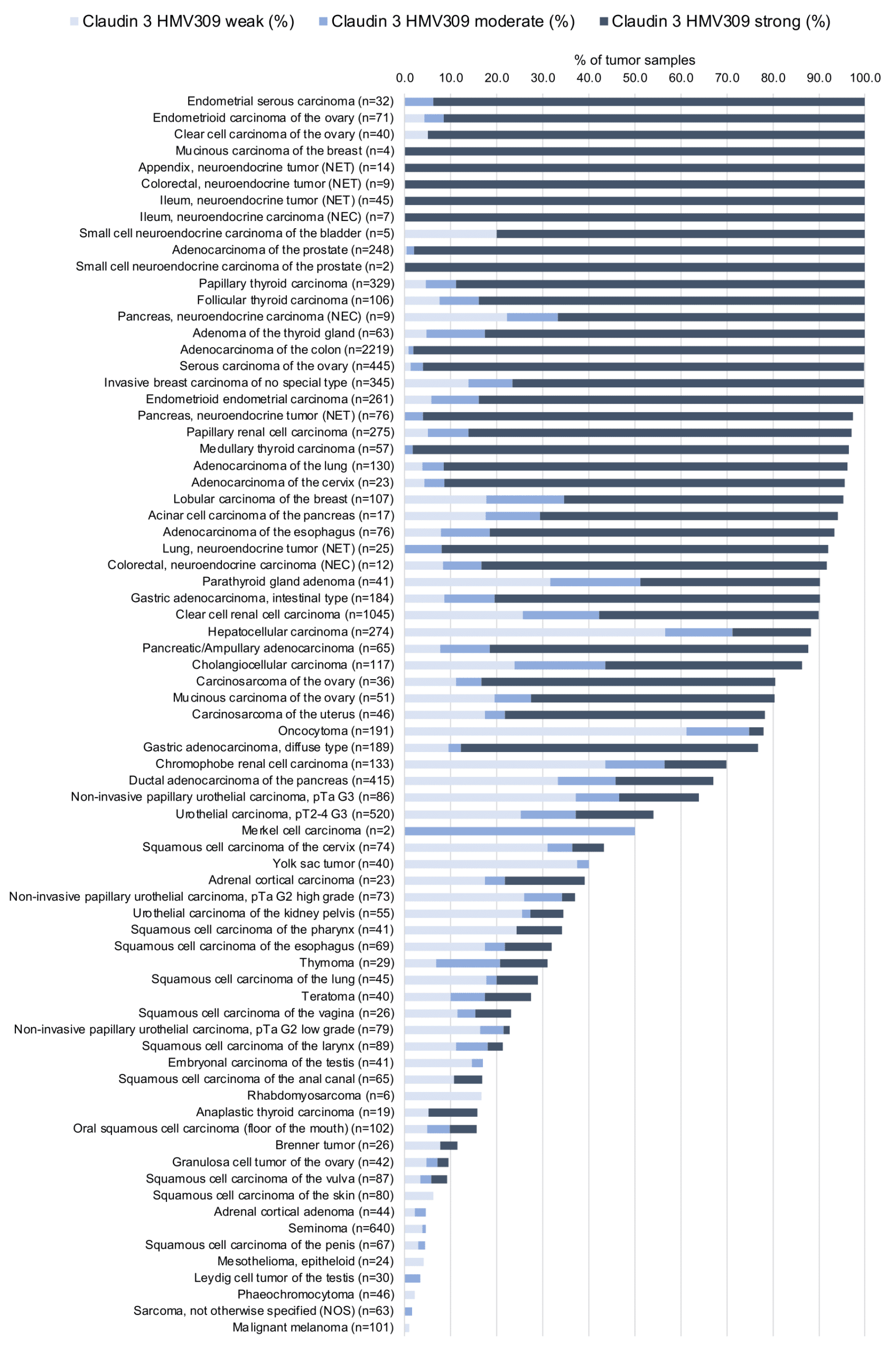
Overall, 96 of 133 tumor categories showed detectable Claudin 3 staining with 80 tumor categories showing at least one strongly positive case. The highest frequencies of Claudin-3 positivity were seen in adenocarcinomas (67–100%) and neuroendocrine neoplasms (92–100%) from different organs, as well as in several tumors of the female genital tract—including diverse subtypes of ovarian and endometrial carcinoma (up to 100%)—and in various subtypes of breast cancer (95.3–100%). The Claudin 3 positivity rates are shown in an “organ-systematic” (Figure 1) and in a “ranking order” figure (Figure 2) below (images based on data from Büyücek et al). Associations with clinical/pathological parameters are also summarized (Figure 3; based on data described by Büyücek et al).
Authors conclusions on the possible clinical role of Claudin 3 staining (Büyücek et al.):
- Both increased and decreased levels of CLDN3 can occur during tumor progression in a cancer type dependent manner.
- A strong association between low CLDN3 expression and unfavorable prognostic tumor features may suggest a clinically useful role of CLDN3 expression measurement in ccRCC.
Data from the publication: Büyücek et al. “Prevalence and clinical significance of Claudin‑3 expression in cancer: a tissue microarray study on 14,966 tumor samples” Published in Biomark Res. 2024 Dec 10;12(1) PMID: 39658782
Summarized in own graphics:
1. Claudin 3 staining in tumors “organ-specific” with antibody HMV309
2. Claudin 3 staining in tumors “ranking order” by positivity with antibody HMV309
Protocol Recommendations
IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein.
All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well.
Manual protocol
Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target Retrieval Solution buffer. Apply HMV309 at a dilution of 1:150 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent) according to the manufacturer’s directions.
Potential Research Applications
- The diagnostic and prognostic relevance of CLDN3 expression in tumors and in preneoplastic disease needs to be investigated.
- CLDN3 is a putative therapeutic target in cancer.
- The role of CLDN3 in non-neoplastic disease needs further investigation.
Evidence for Antibody Specificity in IHC
There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy).
Orthogonal validation: For the antibody HMV309 specificity is consistent with the particularly strong immunostaining in tissue types, for which three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression Claudin 3) had demonstrated the highest RNA levels such as the intestine, thyroid, pancreas, and the prostate. CLDN3 positivity by HMV309 was, however, also detectable in several tissues without documented CLDN3 RNA expression (germinal centre cells in lymphatic tissues, megakaryocytes in the bone marrow, squamous epithelium positivity in the thymus and the tonsil crypts, gallbladder, urothelium, placenta, epididymis, gastric mucosa, adrenal gland, and the parathyroidal gland) as well as in tissues with only very low CLDN3 RNA levels (endometrium) Some of these tissues without previously documented CLDN3 RNA expression but CLDN3 positivity by HMV309 had only very few positive cells that were probably not detected in RNA studies (megakaryocytes, urothelial cells, corpuscles of Hassall’s). For several other tissues, these discrepancies were more difficult to comprehend.
Comparison of antibodies: True expression of CLDN3 in all cell types found to be CLDN3 positive by HMV309 is corroborated by identical staining’s obtained by another commercially available independent antibody (termed “validation antibody”). This specifically applies to cell types from organs that were considered CLDN3 RNA negative (or only weakly positive) such as germinal centre cells in lymphatic tissues, megakaryocytes in the bone marrow, squamous epithelium in the thymus and the tonsil crypts, gallbladder, urothelium, endometrium, placenta, epididymis, gastric mucosa, adrenal gland, and the parathyroid gland. Because of the significant discrepancies with RNA data, the antibody validation also included a second independent commercial validation antibody which also confirmed all these stainings (and additionally showed a cross-reactivity with a gastric mucosa protein) (data not shown).
















































